Download presentation
Presentation is loading. Please wait.

1
GLP-1 Receptor Agonists
ADEA CASE SERIES GLP-1 Receptor Agonists Merlin Thomas Gary Kilov Nicole Frayne Giuliana Murfet Facilitator: Rachel McKeown, Professional Services Manager, ADEA (NSW)
")
2
<7 The right target... COMPROMISE TARGET Motivated/adherent
Good self-care Short duration Low hypo risk Long life expectancy No co-morbidity Good resources Non-compliant Poor self-care Longstanding High hypo risk Short life expectancy Co-morbidity Limited resources <7 COMPROMISE TARGET Adapted from Inzucchi et al Diabetes Care 2012

3
? Standard ….with the right agent Motivated/adherent Non-compliant
Good self-care Short duration Low hypo risk Long life expectancy No co-morbidity Good resources Non-compliant Poor self-care Longstanding High hypo risk Short life expectancy Co-morbidity Limited resources Standard ? Adapted from Inzucchi et al Diabetes Care 2012

4
How does GLP-1 lower glucose levels in diabetes?
1. BACKGROUND How does GLP-1 lower glucose levels in diabetes?

5
Incretins in -cell biology3,4
α β Up to 70% of total post-prandial insulin production is determined by incretins The effect and contribution varies with the size of the glucose challenge / the meal composition MEAL carbohydrate protein, fatty & bile acids vagal vagal Pancreas L GLP-1 GLPR Distal small intestine ileum and colon SLIDE 2. INCRETINS IN BETA-CELL BIOLOGY Incretins are gut hormones that amplify insulin secretion after a meal in a glucose-dependent manner. The two best-known incretins are glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) They exert their insulinotropic actions through activating specific G-protein-coupled receptors (3) This not only augments insulin secretion, but also improves glucose sensitivity in beta-cells that are sub-optimally responsive. Experimental data also suggest that GLP-1 may stimulate beta-cell proliferation and/or reduce apotosis (3). Whether this is sufficient to protect the pancreas against the ravages of diabetes is unclear. Every time a meal is eaten, the L-cells of the intestine release the incretin hormone, GLP-1. These L-cells are found the length of the intestine but are in highest concetration in the distal small intestine, ileum and colon. The initial stimulus to release GLP-1 is neurogenic, mediated by activation of the vagal nerve. Subsequently the passage of nutrients to the distal intestine triggers further larger GLP-1 release through activation of so called ‘nutrient sensing’ pathways (4). Glucose is taken up by the SGLT1 transporter in L-cells Oligopeptides are taken up by PEPT1-dependent uptake. Fatty acids (and especially MUFAs) are taken up by free fatty acid receptors. These stimuli acts to mobilise endogenous GLP-1 and amplify insulin secretion from the pancreas. The dramatic increase in GLP-1 after gastric bypass surgery is partly explained by the increasing the distal transit of nutrients to areas of the intestine rich in L-cells. (3) Campbell & Drucker. Cell Metabolism (2013) (4) Diakogiannaki, et al. Physiol. Behav. (2012). Amplified insulin secretion Improved glucose sensitivity -cell proliferation/neogenesis Reduced -cell apoptosis 3. Campbell & Drucker. Cell Metabolism (2013); 4. Diakogiannaki, et al. Physiol. Behav. (2012). 5
 and glucose-dependent insulinotropic polypeptide (GIP) They exert their insulinotropic actions through activating specific G-protein-coupled receptors (3) This not only augments insulin secretion, but also improves glucose sensitivity in beta-cells that are sub-optimally responsive. Experimental data also suggest that GLP-1 may stimulate beta-cell proliferation and/or reduce apotosis (3). Whether this is sufficient to protect the pancreas against the ravages of diabetes is unclear. Every time a meal is eaten, the L-cells of the intestine release the incretin hormone, GLP-1. These L-cells are found the length of the intestine but are in highest concetration in the distal small intestine, ileum and colon. The initial stimulus to release GLP-1 is neurogenic, mediated by activation of the vagal nerve. Subsequently the passage of nutrients to the distal intestine triggers further larger GLP-1 release. through activation of so called ‘nutrient sensing’ pathways (4). Glucose is taken up by the SGLT1 transporter in L-cells. Oligopeptides are taken up by PEPT1-dependent uptake. Fatty acids (and especially MUFAs) are taken up by free fatty acid receptors. These stimuli acts to mobilise endogenous GLP-1 and amplify insulin secretion from the pancreas. The dramatic increase in GLP-1 after gastric bypass surgery is partly explained by the increasing. the distal transit of nutrients to areas of the intestine rich in L-cells. (3) Campbell & Drucker. Cell Metabolism (2013) (4) Diakogiannaki, et al. Physiol. Behav. (2012). Amplified insulin secretion. Improved glucose sensitivity. -cell proliferation/neogenesis. Reduced -cell apoptosis. 3. Campbell & Drucker. Cell Metabolism (2013); 4. Diakogiannaki, et al. Physiol. Behav. (2012). 5.")
6
Incretins regulate a proportional response
SIGNAL AMPLIFICATION OUTPUT AMPLIFIER GLUCOSE GLP increased FOOD AMPLIFICATION INSULIN* of glucose/meal-stimulated insulin secretion (incret-ins)
")
7
incretin effect in diabetes?
What happens to the incretin effect in diabetes? As a consequence of hyperglycaemia and/or other metabolic manifestations of diabetes itself incretin effect is reduced by ~50% in diabetes8 Normal secretion of GLP-1, but.. Down-regulation of GLP-1 receptor8 Less substrate to act on (β-cells, δ-cells, etc) Gastroparesis8 Resistance to GLP-1 (which needs pharmacological doses to overcome it)8,10 Slide 8. LOSS OF THE INCRETIN EFFECT IN TYPE 2 DIABETES In patients with type 2 diabetes the incretin effect is reduced by approximately half (8). The loss of incretin effect is thought to significantly contribute importantly to the postprandial hyperglycemia in type 2 diabetes (9). The reasons why the incretin effects may be reduced continue to be actively studied. However, it is now thought that the reduction of the incretin effect is a consequence of hyperglycaemia and or other metabolic manifestations of diabetes itself rather than a primary cause of hyperglycemia. Moreover, the mechanism by which the incretin effect is impaired is not related to reduced secretion of GLP-1. In fact, GLP-1 levels appear to be normal in patients with type 2 diabetes (although they should be high give the glucose levels). By contrast there is marked down-regulation of GLP-1 receptor, especially on beta-cells Moreover, the loss of beta cells also means that there is less substrate (β-cells) to act on. Slowing of the stomach emptying in diabetes also attenuates some of the gastrointestinal benefits of GLP-1 that are achieved through slowing stomach emptying (see slide 12) Finally there also appears to be an innate resistance to GLP-1 which means that physiological levels are insufficient to amplify insulin production and pharmacological doses are required to overcome it. This provides the rationale for the high effective doses of GLP-1 Receptor agonists (e.g. exenatide) used in type 2 diabetes. (8) Nauck et al. Diabetologia (2011) (9) De Fronzo R. Diabetes (2009) (10) Vilsbøll T, et al. Diabetologia. (2002) 8. Nauck et al. Diabetologia (2013); 9. De Frionzo Diabetes (2009) 10. Vilsbøll T, et al. Diabetologia. (2002)
 Gastroparesis8. Resistance to GLP-1 (which needs. pharmacological doses to overcome it)8,10. Slide 8. LOSS OF THE INCRETIN EFFECT IN TYPE 2 DIABETES. In patients with type 2 diabetes the incretin effect is reduced by approximately half (8). The loss of incretin effect is thought to significantly contribute importantly to the postprandial hyperglycemia in type 2 diabetes (9). The reasons why the incretin effects may be reduced continue to be actively studied. However, it is now thought that the reduction of the incretin effect is a consequence of hyperglycaemia. and or other metabolic manifestations of diabetes itself rather than a primary cause of hyperglycemia. Moreover, the mechanism by which the incretin effect is impaired is not related to reduced secretion of GLP-1. In fact, GLP-1 levels appear to be normal in patients with type 2 diabetes (although they should be high give the glucose levels). By contrast there is marked down-regulation of GLP-1 receptor, especially on beta-cells. Moreover, the loss of beta cells also means that there is less substrate (β-cells) to act on. Slowing of the stomach emptying in diabetes also attenuates some of the gastrointestinal benefits of GLP-1. that are achieved through slowing stomach emptying (see slide 12) Finally there also appears to be an innate resistance to GLP-1 which means that physiological levels. are insufficient to amplify insulin production and pharmacological doses are required to overcome it. This provides the rationale for the high effective doses of GLP-1 Receptor agonists (e.g. exenatide) used in type 2 diabetes. (8) Nauck et al. Diabetologia (2011) (9) De Fronzo R. Diabetes (2009) (10) Vilsbøll T, et al. Diabetologia. (2002) 8. Nauck et al. Diabetologia (2013); 9. De Frionzo Diabetes (2009) 10. Vilsbøll T, et al. Diabetologia. (2002)")
8
Incretins and hypoglycaemia
NO SIGNAL AMPLIFICATION NO OUTPUT AMPLIFIER No GLUCOSE NO MORE NO FOOD INSULIN GLP1 Reduced risk of hypoglycaemia

9
No increase in insulin when glucose levels are low during a continuous infusion of GLP-11
SLIDE 7. THE INCRETIN EFFECT AND HYPOGLYCAEMIA (B) This study illustrates the exquisite glucose-dependence of the incretin effect and how it avoids hypoglycemia. In this study Glucagon-like peptide 1 (GLP-1) was infused into nine healthy volunteers with normal oral glucose tolerance. At the same time they received insulin to achieve plateaus of 4.3, 3.7, 3.0, and 2.3 mmol/liter for 90 min each (stepwise hypoglycaemic clamp); Notably GLP-1 stimulated insulin secretion only at plasma glucose concentrations of at least 4.3 mmol/liter. Below plasma glucose concentrations of 4.3 mmol/liter, the insulinotropic action of GLP-1 was negligible. If no additional insulin is (inappropriately) made when glucose levels are low, then the potential for hypoglycemia is significantly reduced when compared to sulphonylureas or exogenous insulin. (7) Nauck MA, et al. J Clin Endocrinol Metab Mar;87(3): 7. Nauck et al. JCEM (2002)
 This study illustrates the exquisite glucose-dependence of the incretin effect and how it avoids hypoglycemia. In this study Glucagon-like peptide 1 (GLP-1) was infused into nine healthy volunteers with normal oral glucose tolerance. At the same time they received insulin to achieve plateaus of 4.3, 3.7, 3.0, and 2.3 mmol/liter for 90 min each (stepwise hypoglycaemic clamp); Notably GLP-1 stimulated insulin secretion only at plasma glucose concentrations of at least 4.3 mmol/liter. Below plasma glucose concentrations of 4.3 mmol/liter, the insulinotropic action of GLP-1 was negligible. If no additional insulin is (inappropriately) made when glucose levels are low, then the potential for hypoglycemia. is significantly reduced when compared to sulphonylureas or exogenous insulin. (7) Nauck MA, et al. J Clin Endocrinol Metab Mar;87(3): Nauck et al. JCEM (2002)")
10
What happens to -cells in diabetes?
Diabetes is associated with the blunting of hyperglycaemia or postprandial suppression of glucagon secretion Reduced incretin effect Hyperplasia of -cells Increased sensitivity to glucagon Contributes to the inappropriately increased rate of hepatic glucose output characteristic of T2DM =ALPHA CELL ANARCHY SLIDE 9. DIABETES AND THE ALPHA CELL In type 2 diabetes, the production and secretion of glucagon is inappropriately high (in relation to ambient hyperglycaemia)(8). Under healthy conditions, the glycemic load from a meal or hyperglycemia act to suppress glucagon as a means to reduce hepatic glucose output and a time when glucose uptake is required. Part of this suppression is mediated by GLP-1. In type 2 diabetes, the loss of the incretin effect along with alpha cell hyperplasia and increased hepatic sensitivity to glucagon lead to blunting of hyperglycaemia-induced or postprandial suppression of glucagon secretion. This ambivalence to hyperglycemia is euphemistically known as “alpha cell anarchy” And contributes, alongside impaired insulin release and action, to inappropriately increased rates of hepatic glucose output in the fasting state and attenuated reduction after meals. Our patients frequently complain that their glucose levels are high, even if they don’t eat anything. (8). Defronzo. Diabetes (2009) 8. Defronzo. Diabetes (2009)
(8). Under healthy conditions, the glycemic load from a meal or hyperglycemia act to suppress glucagon. as a means to reduce hepatic glucose output and a time when glucose uptake is required. Part of this suppression is mediated by GLP-1. In type 2 diabetes, the loss of the incretin effect along with alpha cell hyperplasia and increased hepatic sensitivity to glucagon. lead to blunting of hyperglycaemia-induced or postprandial suppression of glucagon secretion. This ambivalence to hyperglycemia is euphemistically known as alpha cell anarchy And contributes, alongside impaired insulin release and action, to inappropriately increased rates of hepatic glucose output. in the fasting state and attenuated reduction after meals. Our patients frequently complain that their glucose levels are high, even if they don’t eat anything. (8). Defronzo. Diabetes (2009) 8. Defronzo. Diabetes (2009)")
11
GLP-1 in -cell biology3,4 β L GLP1 α GLPR MEAL
carbohydrate protein, fatty & bile acids vagal vagal Pancreas β L GLP1 GLPR α Distal small intestine ileum and colon SLIDE 10. GLP-1 AND ALPHA CELL BIOLOGY Glucagon-like peptide-1 (GLP-1) has significant effects on the glucagon-producing alpha-cells of the endocrine pancreas GLP-1 inhibits glucagon secretion in a glucose-dependent manner (3,4). The mechanism of this action is still debated. Certainly, insulin itself is able to suppress glucagon release from alpha cells, and increased insulin production via the incretin effect may have this action. However, the suppression of glucagon is still present in subjects with type 1 diabetes (although incretin based therapies are not indicated), suggesting that the β cells are not essential for transducing the glucagonostatic actions of GLP-1. There is some data to suggest that GLP-1 is able to stimulate the production of somatostatin from delta cells, which itself acts to suppress glucagon synthesis and release (3). Whatever the mechanism, it means that agents that mimic or increase GLP-1 (e.g. exenatide and saxagliptin respectively) are able to reduce inappropriately increased rates of hepatic glucose output in the fasting state and as well amplify its suppression with meals. Some researchers argue that this may be its major mechanism of action in patients with type 2 diabetes. This strategy is clearly synergistic with interventions like SGLT2 inhibitors that trigger compensatory hyperglucagonemia and increase hepatic glucose output in response to urinary glucose losses (11). (3) Campbell & Drucker. Cell Metabolism (2013) (4) Diakogiannaki, et al. Physiol. Behav. (2012) (11) JCI (2014) Augmented suppression of glucagon release Partly via increased insulin Partly via somatostatin (?) 3. Campbell & Drucker. Cell Metabolism (2013); 4. Diakogiannaki, et al. Physiol. Behav. (2012). 11
 has significant effects on the glucagon-producing alpha-cells of the endocrine pancreas. GLP-1 inhibits glucagon secretion in a glucose-dependent manner (3,4). The mechanism of this action is still debated. Certainly, insulin itself is able to suppress glucagon release from alpha cells, and increased insulin production via the incretin effect may have this action. However, the suppression of glucagon is still present in subjects with type 1 diabetes (although incretin based therapies are not indicated), suggesting that the β cells are not essential for transducing the glucagonostatic actions of GLP-1. There is some data to suggest that GLP-1 is able to stimulate the production of somatostatin from delta cells, which itself acts to suppress glucagon synthesis and release (3). Whatever the mechanism, it means that agents that mimic or increase GLP-1 (e.g. exenatide and saxagliptin respectively) are able to reduce inappropriately increased rates of hepatic glucose output in the fasting state. and as well amplify its suppression with meals. Some researchers argue that this may be its major mechanism of action in patients with type 2 diabetes. This strategy is clearly synergistic with interventions like SGLT2 inhibitors. that trigger compensatory hyperglucagonemia and increase hepatic glucose output in response to urinary glucose losses (11). (3) Campbell & Drucker. Cell Metabolism (2013) (4) Diakogiannaki, et al. Physiol. Behav. (2012) (11) JCI (2014) Augmented suppression of glucagon release. Partly via increased insulin. Partly via somatostatin ( ) 3. Campbell & Drucker. Cell Metabolism (2013); 4. Diakogiannaki, et al. Physiol. Behav. (2012). 11.")
12
No impairment of glucagon response (which protects against hypoglycaemia) during an infusion of GLP-1 Control GLP-1 SLIDE 11. GLUCAGON, GLP-1 AND HYPOGLYCAEMIA However, there are some times that glucagon production is vital, and inappropriate suppression of glucagon production may be dangerous. For example, compensatory production of glucagon is an important part of the neuro-hormonal counter-regulatory response to hypoglycemia In so far as GLP-1 suppresses glucagon secretion, it could lead to disturbances of hypoglycaemic counter-regulation. However, like the effect on insulin release, the effect on glucagon are exquisitely glucose-dependent In this same experiment shown earlier, Glucagon-like peptide 1 (GLP-1) was infused into nine healthy volunteers with normal oral glucose tolerance At the same time they received insulin to achieve plateaus of 4.3, 3.7, 3.0, and 2.3 mmol/liter for 90 min each (stepwise hypoglycemic clamp); Only during the euglycemic plateau (4.3 mmol/liter) did GLP-1 modestly suppress glucagon concentrations (4.1 +/- 0.4 vs /- 0.7 pmol/liter; P = 0.012); However, at all hypoglycaemic plateaus, glucagon increased similarly with GLP-1 or placebo, to maximum values greater than 20 pmol/liter (P = 0.97). This experiment clearly shows that while suppression of glucagon by GLP-1 does occur at euglycemia, it does not at hypoglycaemic plasma glucose concentrations. This contributes the reduced risk of hypoglycaemia seen with agents that target the incretin axis. (7) Nauck MA, et al. J Clin Endocrinol Metab Mar;87(3): 7. Nauck et al. JCEM (2002)
 was infused into nine healthy volunteers with normal oral glucose tolerance. At the same time they received insulin to achieve plateaus of 4.3, 3.7, 3.0, and 2.3 mmol/liter for 90 min each (stepwise hypoglycemic clamp); Only during the euglycemic plateau (4.3 mmol/liter) did GLP-1 modestly suppress glucagon concentrations (4.1 +/- 0.4 vs /- 0.7 pmol/liter; P = 0.012); However, at all hypoglycaemic plateaus, glucagon increased similarly with GLP-1 or placebo, to maximum values greater than 20 pmol/liter (P = 0.97). This experiment clearly shows that while suppression of glucagon by GLP-1 does occur at euglycemia, it does not at hypoglycaemic plasma glucose concentrations. This contributes the reduced risk of hypoglycaemia seen with agents that target the incretin axis. (7) Nauck MA, et al. J Clin Endocrinol Metab Mar;87(3): Nauck et al. JCEM (2002)")
13
Incretins in the stomach
MEAL carbohydrate protein, fatty & bile acids Stomach vagal afferents L GLP1 GLPR FULL Distal small intestine ileum and colon Reduced gut motility Delayed stomach emptying Delayed digestion and absorption of carbohydrates2 11. Shah & Vella Rev Endocr Metab Disord (2014); 12. Marathe et al. Diabetes Care (2013)
; 12. Marathe et al. Diabetes Care (2013)")
14
Exenatide slows emptying of the stomach as measured by the half-life of a 99TC -labelled meal13
* * 13. Linnebjerg et al. Regl Pept (2008)
")
15
Incretins in the brain L GLP1 GLPR MEAL brain
carbohydrate protein, fatty & bile acids vagal brain L GLP1 GLPR Distal small intestine ileum and colon Enhanced glucose disposal Increased satiety/fullness Reduced appetite Reduced food intake 2. Campbell & Drucker. Cell Metabolism (2013); 11. Shah & Vella Reviews in Endocrine and Metabolic Disorders (2014)
; 11. Shah & Vella Reviews in Endocrine and Metabolic Disorders (2014)")
16
Incretin biology and DPP4
MEAL carbohydrate protein, fatty & bile acids Short circulating half life (<2 min) vagal Pancreas Stomach Liver Brain L GLP1 GLPR Slide 15. DPP4 Despite the many important physiological effects, the actions of incretins in humans are limited by their short circualting half life. Once GIP and GLP-1 enters the capillaries surrounding the intestine, they undergo rapid degradation catalyzed by dipeptidyl peptidase- 4 (DDP-4), which cleaves the two NH2-terminal amino acids of GIP and GLP-1. The apparent half-lives for intact GIP and GLP-1 have been determined as approximately 5 and 2 min, respectively (2) Less that 25% of the GLP-1 leaving the intestine ever reaches the liver. Even less (~10–15%) of newly secreted GLP-1 reaches the systemic circulation and only a fraction of this is in its intact active intact form (2). This has led to the suggestion that direct stimulation of vagal afferents in the intestinal wall or in the portal vein largely mediate the incretin effect. DPP-4 has a widespread organ distribution (liver; gut; endothelial capillaries; acinar cells of mucous and salivary glands, pancreas; uterus; and immune organs such as thymus, spleen and lymph node) with the highest levels found in the kidney. Other physiological substrates of DPP-4 include neuropeptide-Y (NPY) which has role in appetite, energy homeostasis, and blood pressure control) and substance P (which has a role in pain and inflammation) (2) Campbell & Drucker. Cell Metabolism (2013) DPP4 Distal small intestine ileum and colon 2. Campbell & Drucker. Cell Metabolism (2013); 16
 vagal. Pancreas. Stomach. Liver. Brain. L. GLP1. GLPR. Slide 15. DPP4. Despite the many important physiological effects, the actions of incretins in humans are limited by their short circualting half life. Once GIP and GLP-1 enters the capillaries surrounding the intestine, they undergo rapid degradation catalyzed by dipeptidyl peptidase- 4 (DDP-4), which cleaves the two NH2-terminal amino acids of GIP and GLP-1. The apparent half-lives for intact GIP and GLP-1 have been determined as approximately 5 and 2 min, respectively (2) Less that 25% of the GLP-1 leaving the intestine ever reaches the liver. Even less (~10–15%) of newly secreted GLP-1 reaches the systemic circulation and only a fraction of this is in its intact active intact form (2). This has led to the suggestion that direct stimulation of vagal afferents in the intestinal wall or in the portal vein largely mediate the incretin effect. DPP-4 has a widespread organ distribution (liver; gut; endothelial capillaries; acinar cells of mucous and salivary glands, pancreas; uterus; and immune organs such as thymus, spleen and lymph node) with the highest levels found in the kidney. Other physiological substrates of DPP-4 include neuropeptide-Y (NPY) which has role in appetite, energy homeostasis, and blood pressure control) and substance P (which has a role in pain and inflammation) (2) Campbell & Drucker. Cell Metabolism (2013) DPP4. Distal small intestine ileum and colon. 2. Campbell & Drucker. Cell Metabolism (2013); 16.")
17
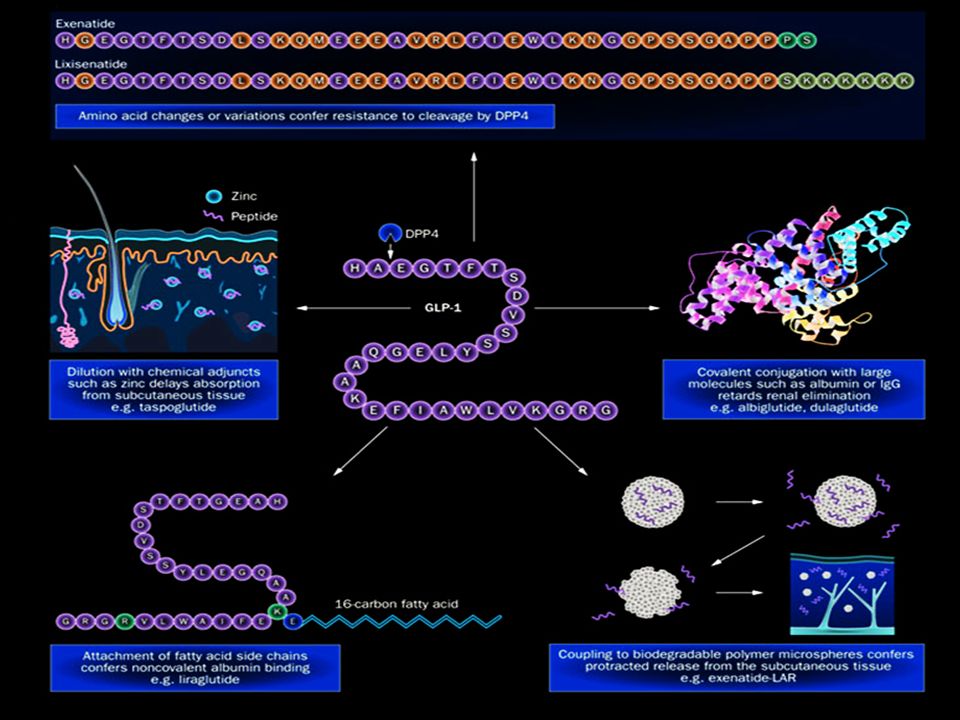
Rationale for GLP analoges1,2
GLP1 (amidated form) DPP4 GLP1 has a 1-4 min half-life (designed for grazing?) EXENATIDE plasma half-life of 2.4 hours and an action time of about 6-8 hours Resistant to DPP4
 DPP4. GLP1 has a 1-4 min half-life. (designed for grazing ) EXENATIDE. plasma half-life of 2.4 hours. and an action time of about 6-8 hours. Resistant to DPP4.")
18
The Gila monster

19
From Lizard Saliva to Diabetes Drug
“I want some of that (adaptation) for my patients”
 for my patients")
21
All lower the HbA1c by approximately the same amount when added-on metformin
40 RCT (n=17795): 6-12 months trials, added-on after MFM failure McIntosh B et al. Open Med 2011; 5:E35-E48
: 6-12 months trials, added-on after MFM failure. McIntosh B et al. Open Med 2011; 5:E35-E48.")
22
Exenitide lowers HbA1cin both dual and triple therapy
MET1 SU2 MET + SU3 *P<0.001 vs placebo †P< vs placebo ‡P< vs placebo Change in HbA1c Speaker notes Byetta provided significant improvements in glycaemic control across a range of background therapies:1-3 Across 3 clinical studies, Byetta (10 μg BID) provided significant HbA1c reductions of -0.8% to -0.9% from baseline. All data are from 30-week, double‐blind, placebo‐controlled registration trials of patients with type 2 diabetes taking Byetta 5 µg or 10 µg BID. Background therapies included MET, SU, and MET + SU. References: DeFronzo RA, et al. Diabetes Care 2005;28:1092100. Buse JB, et al. Diabetes Care 2004;27:262835. Kendall DM, et al. Diabetes Care 2005;28:108391. N 113 110 113 123 125 129 247 245 241 Baseline 8.2 8.3 8.2 8.7 8.5 8.6 8.5 8.5 8.5 Placebo BID Exenatide 5 μg BID Exenatide 10 μg BID Pivotal phase 3 clinical studies—combined intent-to-treat (ITT) 30-week data; mean . 1. DeFronzo RA ,et al. Diabetes Care 2005;28:1092– Buse JB, et al. Diabetes Care 2004;27:2628– Kendall DM, et al. Diabetes Care 2005;28:1083–91.
 provided significant HbA1c reductions of -0.8% to -0.9% from baseline. All data are from 30-week, double‐blind, placebo‐controlled registration trials of patients with type 2 diabetes taking Byetta 5 µg or 10 µg BID. Background therapies included MET, SU, and MET + SU. References: DeFronzo RA, et al. Diabetes Care 2005;28:1092100. Buse JB, et al. Diabetes Care 2004;27:262835. Kendall DM, et al. Diabetes Care 2005;28:108391. N Baseline Placebo BID. Exenatide 5 μg BID. Exenatide 10 μg BID. Pivotal phase 3 clinical studies—combined intent-to-treat (ITT) 30-week data; mean . 1. DeFronzo RA ,et al. Diabetes Care 2005;28:1092– Buse JB, et al. Diabetes Care 2004;27:2628– Kendall DM, et al. Diabetes Care 2005;28:1083–91.")
23
Exenatide was as effective as insulin at lowering HbA1c
Primary endpoint: Change in HbA1c (%) MET, SU, TZD (combination of 2 or 3)4 Background MET + SU1 MET + SU2 MET or SU3 MET5 52 weeks 26 weeks 16 weeks 26 weeks 52 weeks n=253 BL=8.6% n=248 BL=8.6% n=275 BL=8.2% n=260 BL=8.3% N=68 BL= 8.9% N=70 BL= 9% n=118 BL= 8.7% n=116 BL=8.5% n=36 BL= 7.6% n=33 BL= 7.4% Change in HbA1c Speaker notes In 5 head‐to-head trials, Byetta (as adjunct to metformin and/or a sulphonylurea TZD) was shown to be as effective as insulin glargine and insulin aspart at lowering HbA1c at 16 to 52 weeks: 1-5 These primary endpoint data show reductions in HbA1c were similar between Byetta combination therapy and insulin aspart and insulin glargine. This efficacy is achieved without the weight gain seen with insulin glargine. In the same 5 head-to-head trials, Byetta consistently provided weight loss as opposed to weight gain seen with all insulin comparators. Note that Byetta is not approved for the management of obesity. References: Nauck MA, et al. Diabetologia 2007;50(2):25967. Heine R, et al. Ann Int Med 2005;143(8):55969. Barnett A, et al. Clin Ther 2007;29(11):233348. Davies MJ, et al. Diabetes Obes Metab 2009;11(12):115362. Bunck MC, et al. Diabetes Care 2009;32(5):7628. exenatide 10 µg BID plus orals Insulin aspart 70/30 Insulin glargine Abbreviations: BL, baseline; MET, metformin, SU, sulphonylurea; TZD, thiazolidinedione 1. Nauck MA, et al. Diabetologia 2007; 50(2): 259– Heine RJ, et al. Ann Intern Med 2005; 143(8): 559– Barnett AH, et al. Clin Ther 2007; 29(11): 2333– Davies MJ, et al. Diabetes Obes Metab 2009; 11(12): 1153– Bunck MC, et al. Diabetes Care 2009; 32(5): 762–8.
 MET, SU, TZD. (combination of 2 or 3)4. Background. MET + SU1. MET + SU2. MET or SU3. MET5. 52 weeks. 26 weeks. 16 weeks. 26 weeks. 52 weeks. n=253 BL=8.6% n=248 BL=8.6% n=275 BL=8.2% n=260 BL=8.3% N=68 BL= 8.9% N=70 BL= 9% n=118 BL= 8.7% n=116 BL=8.5% n=36 BL= 7.6% n=33 BL= 7.4% Change in HbA1c. Speaker notes. In 5 head‐to-head trials, Byetta (as adjunct to metformin and/or a sulphonylurea TZD) was shown to be as effective as insulin glargine and insulin aspart at lowering HbA1c at 16 to 52 weeks: 1-5. These primary endpoint data show reductions in HbA1c were similar between Byetta combination therapy and insulin aspart and insulin glargine. This efficacy is achieved without the weight gain seen with insulin glargine. In the same 5 head-to-head trials, Byetta consistently provided weight loss as opposed to weight gain seen with all insulin comparators. Note that Byetta is not approved for the management of obesity. References: Nauck MA, et al. Diabetologia 2007;50(2):25967. Heine R, et al. Ann Int Med 2005;143(8):55969. Barnett A, et al. Clin Ther 2007;29(11):233348. Davies MJ, et al. Diabetes Obes Metab 2009;11(12):115362. Bunck MC, et al. Diabetes Care 2009;32(5):7628. exenatide 10 µg BID plus orals. Insulin aspart 70/30. Insulin glargine. Abbreviations: BL, baseline; MET, metformin, SU, sulphonylurea; TZD, thiazolidinedione. 1. Nauck MA, et al. Diabetologia 2007; 50(2): 259– Heine RJ, et al. Ann Intern Med 2005; 143(8): 559– Barnett AH, et al. Clin Ther 2007; 29(11): 2333– Davies MJ, et al. Diabetes Obes Metab 2009; 11(12): 1153– Bunck MC, et al. Diabetes Care 2009; 32(5): 762–8.")
24
Starting GLP-1R agonists
CASE#1

25
Graham presents to his GP
Patient history Age 50 years Married, 3 children Works as a taxi driver BP 132/85 mmHg BMI 30 kg/m2 Non-smoker Diet and exercise not optimal Graham, aged 50 Medical history Diabetes diagnosed 18 months ago Dyslipidaemia and hypertension diagnosed 3 years ago Current Medications Metformin 1500 mg/day Rosuvastatin 20 mg/day Telmisartan/hydrochlorothiazide 80/12.5 mg fixed dose combination Laboratory parameters HbA1c 7.9% Total cholesterol: 3.8 mmol/L Normal albuminuria and eGFR

26
What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability CVD Risk No HYPO Tolerability Cost

27
What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability CVD Risk No HYPO Tolerability Cost Question 1. How well will he tolerate an GLP-1R agonist?

28
Common side effects Nausea (20-30%) Vomiting (~10%) Diarrhoea (~10%)
Injection site reactions (10-20%)
")
29
Nausea and vomiting with exenatide
Exenatide Exenatide LAR attenuates slowly (weeks to months) attenuates rapidly (4-8 weeks)
 attenuates rapidly (4-8 weeks)")
30
Tricks for tolerability
Cautious dose escalation 5µg bd to 10µg bd Reducing the size as well as the fat content of meals can sometimes help get patients through. Although exenatide can be injected at any time within 60 minutes of meal, starting off at ~15 minutes prior meal and slowly extending this depending on tolerability can also help. Question 1a. What other tricks do you have?

31
What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability CVD Risk No HYPO Tolerability Cost Question 2. What about driving on a GLP-1RA?

32
Meta-analysis: Overall hypoglycemia for medications added-on metformin
34 RCT (n=16704): 6-12 months trials, added-on after metformin failure McIntosh B et al. Open Med 2011; 5:E35-E48
: 6-12 months trials, added-on after metformin failure. McIntosh B et al. Open Med 2011; 5:E35-E48.")
33
GLP1 doesn’t cause hypoglycemia
GLP-1 actions on the β cell are normally tightly coupled to the level of ambient glucose. The insulinotropic actions of GLP-1 are rapidly terminated once the plasma glucose falls into the normal range

34
But they do make it easier for SUs to cause hypoglycemia
GLP-1RA Closer to the edge, reduced food intake as well as uncoupling of GLP-1 from its glucose dependence by sulphonylureas

35
Byetta added to metformin does not increase the risk of hypoglycaemia; with SU consider dose reduction Placebo 30-Week, randomised, placebo-controlled Exenatide 5 g Exenatide 10 g 40 36% 28% 30 Incidence of hypoglycaemia (%) 19% 20 14% 13% 10 5% 5% 5% 3% Speaker notes: • Byetta’s effects are mediated by glucose-dependent stimulation of insulin secretion and suppression of inappropriately elevated glucagon levels typical of patients with type 2 diabetes.1 • When Byetta is used with MET, there is no increased risk of hypoglycaemia compared with placebo. 2 • The incidence of hypoglycaemia was increased over that of placebo when Byetta was used in combination with an SU (with or without MET).3,4 • To reduce the risk of hypoglycaemia, reduction in the dose of sulphonylurea should be considered.3,5 References: DeFronzo RA, et al. Diabetes Care. 2005;28:1092100. Tenzer-Iglesias P, Brunton S. J Fam Prac 2008; 57: S17S24 Buse JB, et al. Diabetes Care. 2004;27:262835. Kendall DM, et al. Diabetes Care. 2005;28:108391 Byetta Approved Product Information 7 September 2012. EX + SU1 (n=337; ITT population) EX + MET2 (n=336; ITT population) EX + SU + MET3 (n=733; ITT population) 1. Buse JB, et al. Diabetes Care. 2004; 27: 2628– DeFronzo RA, et al. Diabetes Care. 2005; 28: 109– Kendall DM, et al. Diabetes Care. 2005; 28: 1083–91.
 19% % 13% 10. 5% 5% 5% 3% Speaker notes: • Byetta’s effects are mediated by glucose-dependent stimulation of insulin secretion and suppression of inappropriately elevated glucagon levels typical of patients with type 2 diabetes.1. • When Byetta is used with MET, there is no increased risk of hypoglycaemia compared with placebo. 2. • The incidence of hypoglycaemia was increased over that of placebo when Byetta was used in combination with an SU (with or without MET).3,4. • To reduce the risk of hypoglycaemia, reduction in the dose of sulphonylurea should be considered.3,5. References: DeFronzo RA, et al. Diabetes Care. 2005;28:1092100. Tenzer-Iglesias P, Brunton S. J Fam Prac 2008; 57: S17S24. Buse JB, et al. Diabetes Care. 2004;27:262835. Kendall DM, et al. Diabetes Care. 2005;28:108391. Byetta Approved Product Information 7 September EX + SU1 (n=337; ITT population) EX + MET2 (n=336; ITT population) EX + SU + MET3 (n=733; ITT population) 1. Buse JB, et al. Diabetes Care. 2004; 27: 2628– DeFronzo RA, et al. Diabetes Care. 2005; 28: 109– Kendall DM, et al. Diabetes Care. 2005; 28: 1083–91.")
36
GLP-1 in the presence of a sulfonylurea agent leads to enhanced insulin secretion and suppressed glucagon even at normal or low glucose concentrations GLP1 control De Heer et al Diabetes 2007

37
What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Loss Sustainability CVD Risk No HYPO Tolerability Cost Question 3. How will GLP-1R agonist affect his weight?

38
Meta-analysis: Body weight change for medications added-on metformin
30 RCT (n=15265): 6-12 months trials, added-on after MFM failure McIntosh B et al. Open Med 2011; 5:E35-E48
: 6-12 months trials, added-on after MFM failure. McIntosh B et al. Open Med 2011; 5:E35-E48.")
39
Change in body weight (kg)
Exenatide 10 μg BID provided long-term glycaemic control without weight gain over 156 weeks*† Changes in body weight1 -1 -2 -3 -4 -5 -6 -7 -8 -9 -10 26 52 78 104 130 156 ‡P<0.0001 Mean baseline body weight: 99 ± 18 kg reduction from baseline -1.6 kg at week 12 -5.3 kg at 3 years N=217 Change in body weight (kg) Treatment (weeks) > 85% patients lose weight ‡ Speaker notes As a secondary endpoint, Byetta provided weight loss as early as 12 weeks, and progressive weight loss continued over a period of 3 years.1 In this open-label extension study, Byetta patients achieved a mean weight loss at 3 years of -5.3 kg from baseline.1 It is important to note that Byetta is not indicated for the management of obesity. Also, in patients treated with exenatide, weight loss >1.5 kg/week has been observed. Weight loss at this rate may have harmful consequences.2 References: Klonoff DC, et al. Curr Med Res Opin 2008;24: Byetta Approved Product Information 7 September 2012. *Of 527 subjects, 217 completed 156 weeks of the study, of which 84% lost weight and 50% lost at least 5% of baseline body weight.1 †Exenatide is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. Weight loss >1.5 kg per week has been observed in patients treated with exenatide2 Weight loss of this rate may have harmful consequences2 Klonoff DC et al. Curr Med Res Opin 2008; 24: 275– Byetta Approved Product information 17 September2012 .
 Treatment (weeks) > 85% patients lose weight. ‡ Speaker notes. As a secondary endpoint, Byetta provided weight loss as early as 12 weeks, and progressive weight loss continued over a period of 3 years.1. In this open-label extension study, Byetta patients achieved a mean weight loss at 3 years of -5.3 kg from baseline.1. It is important to note that Byetta is not indicated for the management of obesity. Also, in patients treated with exenatide, weight loss >1.5 kg/week has been observed. Weight loss at this rate may have harmful consequences.2. References: Klonoff DC, et al. Curr Med Res Opin 2008;24: Byetta Approved Product Information 7 September *Of 527 subjects, 217 completed 156 weeks of the study, of which 84% lost weight and 50% lost at least 5% of baseline body weight.1 †Exenatide is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. Weight loss >1.5 kg per week has been observed in patients treated with exenatide2. Weight loss of this rate may have harmful consequences2. Klonoff DC et al. Curr Med Res Opin 2008; 24: 275– Byetta Approved Product information 17 September")
40
Potential for weight loss with Exenatide versus weight gain with insulin glargine
(Mean baseline body weight 88.3 kg) (Mean baseline body weight 87.5 kg) * * * * * Speaker notes This efficacy is achieved without the weight gain seen with insulin glargine.1,2 In the same head-to-head trials, Byetta consistently provided weight loss as opposed to weight gain seen with insulin glargine. 1,2 This randomised, controlled, open-label, parallel-arm study of 26 weeks in duration involves adult patients with type 2 diabetes suboptimally controlled with metformin and a sulfonylurea.1 Body weight decreased 2.3 kg with exenatide and increased 1.8 kg with insulin glargine (difference, 4.1 kg [CI, 4.6 to 3.5 kg]).1 Baseline demographics included1 - Age range: years BMI range: 25 kg/m2 to 45 kg/m2, with a history of stable body weight (10% variation for 3 months before screening). Byetta is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. References Heine R, et al. Ann Int Med 2005;143(8):55969. Barnett A, et al. Clin Ther 2007;29(11):233348. * Insulin glargine n = Byetta n = Weeks *P < compared with insulin glargine measure at the same time point. †Exenatide is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. Adapted from Heine RJ, et al. Ann Intern Med 2005; 143(8): 559–69.
 (Mean baseline body weight 87.5 kg) * * * * * Speaker notes. This efficacy is achieved without the weight gain seen with insulin glargine.1,2. In the same head-to-head trials, Byetta consistently provided weight loss as opposed to weight gain seen with insulin glargine. 1,2. This randomised, controlled, open-label, parallel-arm study of 26 weeks in duration involves adult patients with type 2 diabetes suboptimally controlled with metformin and a sulfonylurea.1. Body weight decreased 2.3 kg with exenatide and increased 1.8 kg with insulin glargine (difference, 4.1 kg [CI, 4.6 to 3.5 kg]).1. Baseline demographics included1. - Age range: years. BMI range: 25 kg/m2 to 45 kg/m2, with a history of stable body weight (10% variation for 3 months before screening). Byetta is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. References. Heine R, et al. Ann Int Med 2005;143(8):55969. Barnett A, et al. Clin Ther 2007;29(11):233348. * Insulin glargine n = Byetta n = Weeks. *P < compared with insulin glargine measure at the same time point. †Exenatide is not indicated for the management of obesity, and weight change was a secondary endpoint in clinical trials. Adapted from Heine RJ, et al. Ann Intern Med 2005; 143(8): 559–69.")
41
50 y.o. What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability 50 y.o. CVD Risk No HYPO Tolerability Cost Q4. How well will an GLP-1RA keep working?

42
Sustainability – the NIKE effect
Exhaustion (nike effect) Sustainability – the NIKE effect
 Sustainability – the NIKE effect.")
43
Exenatide 10 μg BID provides sustained HbA1c reduction over 156 weeks*
Mean change in HbA1c from baseline 10 9 8 7 6 5 4 3 2 1 Mean baseline HbA1c: 8.2% reduction from baseline -1.1% at week 12 reduction from baseline -1.0% at 3 years † Mean HbA1c (%) Speaker notes Byetta provided sustained HbA1c reductions over 3 years:1 156‐week data demonstrate the sustained glycaemic control achieved with Byetta over time. In a combined open‐label, uncontrolled extension trial of the three 30‐week registration trials, Byetta‐treated patients experienced a mean HbA1c reduction of 1% from baseline after 3 years. Results are from three 30‐week, double‐blind, placebo‐controlled registration trials of Byetta 10 µg as adjunct to metformin and/or a sulphonylurea (N=483) and their open‐label, uncontrolled extension trials. Self-selected patients with type 2 diabetes (N=217) from the registration trials entering the open‐label extension continued treatment with metformin and/or a sulphonylurea and were treated with Byetta 5 µg BID for 4 weeks before receiving Byetta 10 µg BID for > 3 years. All patients in the open‐label extension had been treated with Byetta for at least 3 years irrespective of their treatment group in the registration trials. Reference Klonoff DC, et al. Curr Med Res Opin 2008;24:27586. †P<0.0001 26 52 78 104 130 156 N=217 Treatment (weeks) *Of 527 subjects, 217 completed 156 weeks of the study, of which 46% achieved HbA1c of ≤7%. Adapted from Klonoff DC, et al. Curr Med Res Opin 2008; 24: 275–86.
 Speaker notes. Byetta provided sustained HbA1c reductions over 3 years:1. 156‐week data demonstrate the sustained glycaemic control achieved with Byetta over time. In a combined open‐label, uncontrolled extension trial of the three 30‐week registration trials, Byetta‐treated patients experienced a mean HbA1c reduction of 1% from baseline after 3 years. Results are from three 30‐week, double‐blind, placebo‐controlled registration trials of Byetta 10 µg as adjunct to metformin and/or a sulphonylurea (N=483) and their open‐label, uncontrolled extension trials. Self-selected patients with type 2 diabetes (N=217) from the registration trials entering the open‐label extension continued treatment with metformin and/or a sulphonylurea and were treated with Byetta 5 µg BID for 4 weeks before receiving Byetta 10 µg BID for > 3 years. All patients in the open‐label extension had been treated with Byetta for at least 3 years irrespective of their treatment group in the registration trials. Reference. Klonoff DC, et al. Curr Med Res Opin 2008;24:27586. †P< N=217. Treatment (weeks) *Of 527 subjects, 217 completed 156 weeks of the study, of which 46% achieved HbA1c of ≤7%. Adapted from Klonoff DC, et al. Curr Med Res Opin 2008; 24: 275–86.")
44
Five-Year Efficacy and Safety Data of Exenatide Once Weekly
DURATION1. Mayo Clin Proc (2015)
")
45
What are Graham’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability CVD Risk No HYPO Tolerability Cost Question 5. Will a GLP1RA protect his heart?

46
CV Outcomes and GLP-1RA SUSTAIN-6 Semaglutide (N = 3260) 2012 2013 2014 2015 2016 2017 2018 2019 ELIXA Lixisenatide (N = 6000) LEADER Liraglutide (N = 9341) EXSCEL Exenatide (N = 9500) REWIND Dulaglutide (N = 9622)
 LEADER. Liraglutide (N = 9341) EXSCEL. Exenatide. (N = 9500) REWIND. Dulaglutide (N = 9622)")
47
What are Graham’s treatment priorities? Question 5. Is it subsidised?
Compliance Lower HbA1c Weight Sustainability CVD risk No HYPO Tolerability Cost Question 5. Is it subsidised?

48
GLP-1RA in addition to insulin
CASE#2 GLP-1RA in addition to insulin

49
Kevin presents to his GP
Patient history Age 50 years BP 142/75 mmHg BMI 37 kg/m2 Non-smoker Diet and exercise not optimal Kevin aged 50 Medical history Diabetes diagnosed 5 years ago Failed oral therapy Now on insulin injections But control is still suboptimal Current Medications Metformin 2g/day Insulin 100U/day Rosuvastatin 20 mg/day Telmisartan/hydrochlorothiazide 80/12.5 mg fixed dose combination Laboratory parameters HbA1c 8.2% Total cholesterol: 5.8 mmol/L eGFR 125 ml/min/1.73m2

50
Weight What are Kevin’s treatment priorities?
Compliance Lower HbA1c Weight Sustainability CVD Risk No HYPO Tolerability Cost Q 6. How well will an GLP1RA work for Kevin (on top of his insulin regimen)?
")
51
Over the past 3 years, however, the effectiveness of combining GLP-1 receptor agonists (both shorter-acting and newer weekly formulations) with basal insulin has been demonstrated, with most studies showing equal or slightly superior efficacy to the addition of prandial insulin, and with weight loss and less hypoglycemia. The available data now suggest that either a GLP-1 receptor agonist or prandial insulin could be used in this setting, with the former arguably safer, at least for short-term outcomes Inzucchi Diabetes (2015)
")
52
Exenatide lowers HbA1c when used in combination with basal insulin1
Speaker notes Results of a 30-week, double-blind, randomised study showed that insulin glargine, alone or in combination with metformin and/or pioglitazone , and titrated using a treat-to-target algorithm:1,2 plus placebo reduced HbA1c levels 1.04% from baseline during the study period in combination with Byetta, reduced HbA1c levels 1.74% from baseline during the study period. Please note that Byetta is not indicated for use with metformin plus pioglitazone in Australia.1 Byetta and insulin have complementary modes of action.1 A potential benefit of adding Byetta to basal insulin include improved glycaemic control by targeting both fasting plasma glucose (FPG), and postprandial plasma glucose (PPG).2* *When Byetta is used in combination with insulin, the dose of insulin should be evaluated. In patients at increased risk of hypoglycaemia, consider reducing the insulin dose.1 References Byetta Approved Product Information, 3 May 2013. Buse JB, et al. Ann Intern Med 2011;154:103−12. 1. Buse JB, et al. Ann Intern Med 2011; 154: 103–12 ;
, and postprandial plasma glucose (PPG).2* *When Byetta is used in combination with insulin, the dose of insulin should be evaluated. In patients at increased risk of hypoglycaemia, consider reducing the insulin dose.1. References. Byetta Approved Product Information, 3 May Buse JB, et al. Ann Intern Med 2011;154:103− Buse JB, et al. Ann Intern Med 2011; 154: 103–12 ;")
53
No increased risk of weight gain or hypoglycaemia when exenatide is added to basal insulin1,2**†
Change in weight* Minor hypoglycaemia Exenatide Speaker notes There was no increased hypoglycaemia risk or weight gain vs. titrated basal insulin alone or in combination with metformin and/or pioglitazone. Change in weight was a secondary endpoint in this study. 1 Note Byetta is not indicated as a weight reduction agent.2 When Byetta is used in combination with insulin, the dose of insulin should be evaluated. In patients at increased risk of hypoglycaemia, consider reducing the insulin dose.2 References Buse JB, et al. Ann Intern Med 2011;154:103−12. Byetta Approved Product information, 3 May 2013. 1. Buse JB, et al. Ann Intern Med 2011; 154: 103–12.;.

54
THANK YOU FOR YOUR PARTICIPATION
ADEA CASE SERIES THANK YOU FOR YOUR PARTICIPATION Merlin Thomas Gary Kilov Nicole Frayne

Similar presentations

 + GIP = incretin effect =Augmentation of insulin after oral glucose Type 2 diabetics little incretin effect Reduced GLP-1 secretion.>")
 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")














 8 : 20 ~ 8 : 50 B 棟 8 階カンファレンスルーム 薬剤部 TTSP 石井 英俊.>")
 Trial Overview Large international randomized controlled trial in patients with.>")
