Download presentation
Presentation is loading. Please wait.

1
COMPLICATIONS OF PREGNANCY Jeanie Ward 1 1 1

2
Risk Factors Age – under 17 over 35 Gravida and Parity
Socioeconomic status Psychological well-being Predisposing chronic illness – diabetes, heart conditions, renal, etc. Pregnancy related conditions – hyperemesis gravidarum, PIH, etc.

3
High Risk Pregnancy Goals of Care
Provide with optimum care for the mother and the fetus Assist the patient and her family to understand and cope with the variations in a High Risk Pregnancy and cope with her feelings 1 1 1 1

4
Gestational Onset Disorders

5
Take report: Mrs. R. admitted to L&D
Initial Data Chief complaint: moderate amount vaginal bleeding Vital Signs: T. 98.4; P. 100, R. 22, B/P 100/66 G i P 0 Last menstrual period: 8/12; EDC: May 19 Allergies: none known Nauseated Mild pain HCG levels – normal for pregnancy

6
Bleeding Disorders 2 2 2 2

7
Abortions Termination of pregnancy at any time before the fetus has reached the age of viability Either: spontaneous – occurring naturally induced – artificial Question 1 3 3 3 3

8
Etiology / Predisposing Factors
Chromosomal abnormalities - Faulty germ plasm -- imperfect ova or sperm, genetic make-up (chromosomal disorders), congenital abnormalities Faulty implantation Decrease in the production of progesterone Drugs or radiation Maternal causes -- infections, endocrine disorders, malnutrition, hypertension, cervix disorder 4 4 4 4
, congenital abnormalities. Faulty implantation. Decrease in the production of progesterone. Drugs or radiation. Maternal causes -- infections, endocrine disorders, malnutrition, hypertension, cervix disorder")
9
Assessment Types of Abortions Threatened
Signs and Symptoms vaginal bleeding, spotting Mild cramps, backache Cervix remains CLOSED Treatment and Nursing Care Bed rest, sedation, Avoid stress and intercourse Progesterone therapy A period of “watchful waiting” 5 5 5 5

10
Imminent Abortion Signs and Symptoms Treatment and Nursing Care
Loss is certain Bleeding is more profuse Painful uterine contractions Cervix DILATES Treatment and Nursing Care Assess all bleeding. Save all pads. (May need to weigh the pads) Use the bedpan to assess all products expelled Treated by evacuation of the uterus usually be a D & C or suction Provide Psychological Support 6 6 6 6
 Use the bedpan to assess all products expelled. Treated by evacuation of the uterus usually be a D & C or suction. Provide Psychological Support")
11
Complete Abortion All products of conception are expelled
No treatment is needed, but may do a D & C 7 7 7 7

12
Incomplete Abortion Parts of the products of conception are expelled, with placenta and membranes retained Treated with a D & C or suction evacuation Provide support to the family 8 8 8 8

13
Missed Abortion The fetus dies in-utero and is not expelled
Uterine growth ceases Breast changes regress Maceration occurs Treatment: D & C Hysterotomy 9 9 9 9

14
Question??? What are two main complications related to a missed abortion? 1. 2.

15
Recurrent / Habitual Abortion Premature Cervical Dilation
Abortion occurs consecutively in _____ or more pregnancies Usually due to an Incompetent Cervical Os Occurs most often about weeks gestation. 10 10 10 10

16
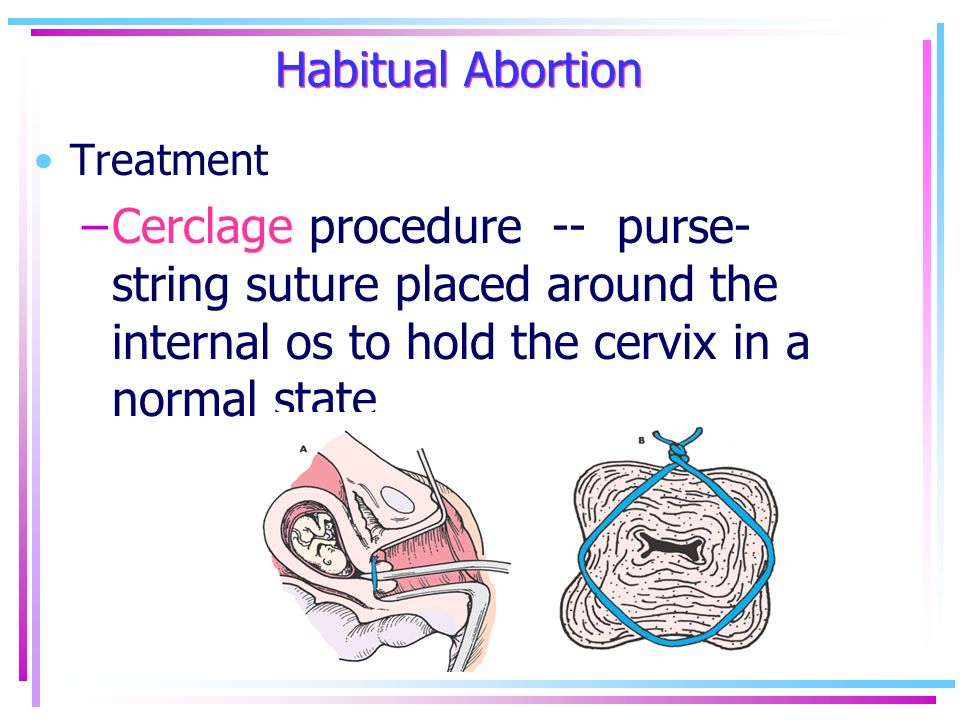
Habitual Abortion Treatment Cerclage procedure -- purse-string suture placed around the internal os to hold the cervix in a normal state 11 11 11 11
17
Nursing Care Bedrest in a slight trendlenburg position to decrease the pressure on the new sutures Teach: Assess for leakage of fluid, bleeding Assess for contractions Assess fetal movement and report decrease movement (if old enough) Assess temperature for elevations
 Assess temperature for elevations.")
18
Delivery options: When time for delivery there are several options:
physician will clip suture and allow patient to go into labor on her own induce labor cesarean delivery

19
Key Concepts to Remember!!
If a woman is Rh-, RhoGam is given within 72 hours Provide emotional support. Feelings of shock or disbelief are normal Encourage to talk about their feelings. It begins the grief process 13 13 13 13

20
Bleeding Disorders Ectopic Pregnancy
Implantation of the blastocyst in ANY site other than the endometrial lining of the uterus ovary (5) Cervical Question 2 14 14 14 14
 Cervical. Question")
21
Etiology / Contributing Factors
Salpingitis Pelvic Inflammatory Disease, PID Endometriosis Tubal atony or spasms Imperfect genetic development Question 3 16 16 16

22
Assessment Ectopic Pregnancy
Early: Missed menstruation followed by vaginal bleeding (scant to profuse) Unilateral pelvic pain, sharp abdominal pain Referred shoulder pain Cul-de-sac mass Acute: Shock – blood loss poor indicator Cullen’s sign -- bluish discoloration around umbilicus Nausea, Vomiting Faintness 15 15 15 15
 Unilateral pelvic pain, sharp abdominal pain. Referred shoulder pain. Cul-de-sac mass. Acute: Shock – blood loss poor indicator. Cullen’s sign -- bluish discoloration around umbilicus. Nausea, Vomiting. Faintness")
23
Diagnostic Tests Ectopic Pregnancy
Diagnosis: Ultrasound Culdocentesis Laparoscopy 17 17 17

24
Treatment Options / Nursing Care
Combat shock / stabilize cardiovascular Draw blood for type and cross match Give blood replacements IV’s. Laparotomy Psychological support Linear salpingostomy Methotrexate – used prior to rupture. Destroys fast growing cells Question 4

25
Gestational Trophoblastic Disease Hydatiform Molar Pregnancy Etiology
A DEVELOPMENTAL ANOMALY OF THE PLACENTA WITH DEGENERATION OF THE CHORIONIC VILLI As cells degenerate, they become filled with fluid and appear as fluid filled grape-size vessicles. Question 5 18 18 18

26
Assessment: Vaginal Bleeding -- scant to profuse, brownish in color (prune juice) Enlargement of the uterus out of proportion to the duration of the pregnancy Vaginal discharge of grape-like vesicles May display signs of pre-eclampsia early Hyperemesis gravidarium No Fetal heart tone or Quickening Abnormally elevated levels of HCG Question 6 19 19 19

27
Interventions and Follow-Up
Empty the Uterus by D & C or Hysterotomy Follow-Up for One Year Assess for the development of choriocarcinoma Blood tests for levels of HCG frequently Chest X-rays Placed on oral contraceptives If the levels rise, then chemotherapy started usually Methotrexate Question 7 20 20 20

28
Critical Thinking Exercise
A woman who just had an evacuation of a hydatiform mole tells the nurse that she doesn’t believe in birth control and does not intend to take the oral contraceptives that were prescribed for her. How should the nurse respond?

29
Placenta Previa Low implantation of the placenta in the uterus
Etiology Usually due to reduced vascularity in the upper uterine segment from an old cesarean scar or fibroid tumors Three Major Types: Low or Marginal Partial Complete Question 8 21 21 21

30
Abruptio Placenta Premature separation of the placenta from the implantation site in the uterus Etiology: Chronic Hypertension Sudden decompression of an over-distended uterus Trauma Injudicious use of Pitocin Smoking / Caffeine / Cocaine Vascular problems 22 22

31
Placenta Previa Abruptio Placenta PAINLESS vaginal bleeding
Bright red bleeding First episode of bleeding is slight then becomes profuse Signs of blood loss comparable to extent of bleeding Uterus soft, non-tender Fetal parts palpable; FHT’s countable Blood clotting defect absent Abruptio Placenta Bleeding accompanied Abruptio by PAIN Dark red bleeding First episode of bleeding usually profuse Signs of blood loss out of proportion to visible amount Uterus board-like, painful Fetal parts non-palpable, FHT’s non-countable Blood clotting defect (DIC) likely 23 23 23
 likely")
32
Signs of Concealed Hemorrhage
Increase in fundal height Hard, board-like abdomen High uterine baseline tone on electronic fetal monitoring Persistent abdominal pain Systemic signs of hemorrhage Question 8-C

33
Interventions and Nursing Care
Placenta Previa Bed-rest Assessment of bleeding Electronic fetal monitoring If it is low lying, then may allow to deliver vaginally Cesarean delivery for All other types of previa Abruptio Placenta Deliver by cesarean delivery immediately Combat shock – blood replacement / fluid replacement Blood work – assessment of DIC 24 24

34
Critical Thinking Mrs. A. , G3 P2, 38 weeks gestation is admitted to L & D with bleeding. What is the priority nursing intervention at this time? Assess the fundal height for a decrease Place a hand on the abdomen to assess if hard, board-like, tetanic Place a clean pad under the patient to assess the amount of bleeding Prepare for an emergency cesarean delivery 25 25

35
Disseminated Intravascular Coagulation (DIC)
Anti-coagulation and Pro-coagulation effects existing at the same time. Question 9 27 27

36
Etiology Defect in the Clotting Cascade
An abnormal overstimulation of the coagulation process Activation of Coagulation with release of thromboplastin ê Thrombin (powerful anticoagulant) is produced Fibrinogen fibrin which enhances platelet aggregation Widespread fibrin and platelet deposition in capillaries and arterioles 26 26
 is produced. Fibrinogen fibrin which enhances platelet aggregation. Widespread fibrin and platelet deposition in capillaries and arterioles")
37
Resulting in Thrombosis (multiple small clots)
Excessive clotting activates the fibrinolytic system Lysis of the new formed clots create fibrin split products These products have anticoagulant properties and inhibit normal blood clotting A stable clot cannot be formed at injury sites Hemorrhage occurs Ischemia of organs follows from vascular occlusion of numerous fibrin thrombi Multisite hemorrhage results in shock and can result in death

38
Disseminated Intravascular Coagulation (DIC)
Precipating Factors: Abruptio placenta PIH Sepsis Retained fetus (fetal demise) Fetal placenta fragments
 Fetal placenta fragments.")
39
Assessment Signs and Symptoms
Spontaneous bleeding -- from gums and Epistasis, and injection and IV sites, incisions Excessive bleeding -- Petechiae at site of blood pressure cuff, pulse points. Ecchymosis Tachycardia, diaphoresis, restlessness, hypotension Hematuria, oliguria, occult blood in stool Mental changes if brain affected. Question 9-C 28 28

40
Diagnostic Tests Lab work reveals: PT – Prothrombin time is prolonged
PTT – Partial Thromboplastin Time increased D-Dimer – increased Product that results from fibrin degradation. More specific marker of the degree of fibrinolysis Platelets -- decreased Fibrin Split Products – increase An increase in both FSP and D-Dimer are indicative of DIC

41
DIC Interventions and Nursing Care
Remove Cause Evaluate vital signs Replace blood and blood products Fluid replacement May give Heparin Question 9-D: E 29 29

42
Hyperemesis Gravidarum

43
HYPEREMESIS GRAVIDARIUM
**Pernicious vomiting during Pregnancy Question 10 3 3 3

44
Hyperemesis Gravidarium
Etiology Increased levels of HCG 4 4 4

45
Assessment Persistent nausea and vomiting
Weight loss from pounds May become severely dehydrated with oliguria increased specific gravity, and dry skin Depletion of essential electrolytes Metabolic alkalosis -- Metabolic acidosis Starvation 5 5 5

46
Nursing Care / Interventions Hyperemesis Gravidarium
Control vomiting Maintain adequate nutrition and electrolyte balance Allow patient to eat whatever she wants If unable to eat – Hyperalimentation Combat emotional component – provide emotional support Weigh daily Check urine for output, ketones Question 11 & 12 6 6 6

47
Pregnancy Induced Hypertension

48
PREGNANCY INDUCED HYPERTENSION
A hypertensive disease of pregnancy. Known as pre-eclampsia and eclampsia. Pre-eclampsia = hypertension, edema proteinuria, Eclampsia = other signs plus convulsions It develops between the 20th and 24th week of gestation and disappears after the tenth day postpartum Question 13 7 7 7

49
PREDISPOSING FACTORS MULTIPLE PREGNANCY PRIMIGRAVIDA
UNDER 17 AND OVER 35 HYDATIFORM MOLE PREDISPOSING FACTORS FAMILY HISTORY VASCULAR DISEASE Diabetes, renal LOWER SOCIOECONOMIC STATUS Severe malnutrition, decrease Protein intake Question 14 Inadequate or late prenatal care 8 8 8

50
PATHOLOGICAL CHANGES PIH is due to: Endothelial CELL DAMAGE
INCREASED PERIPHERAL RESISTANCE; IMPEDED BLOOD FLOW ( in blood pressure) GENERALIZED ARTERIOLAR CYCLIC VASOSPASMS Endothelial CELL DAMAGE (decrease in diameter of blood vessel) Intravascular Fluid Redistribution Decreased Organ Perfusion Question 15 Multi-system failure Disease 9 9 9
 GENERALIZED. ARTERIOLAR. CYCLIC. VASOSPASMS. Endothelial. CELL DAMAGE. (decrease in diameter. of blood vessel) Intravascular. Fluid Redistribution. Decreased Organ. Perfusion. Question 15. Multi-system failure Disease")
51
Clinical Manifestation
HYPERTENSION Earliest and The Most Dependable Indicator of PIH 10 10 10

52
Hypertension B/P = 140 / 90 if have no baseline.
mm. Hg. systolic increase or a 15 mm. Hg. diastolic increase (two occasions four to six hours apart) 2. Increase in MAP > 20 mm.Hg over baseline or >105 mm. Hg. with no baseline Positive Roll Over Test 11 11 11
 2. Increase in MAP > 20 mm.Hg. over baseline or >105 mm. Hg. with no baseline. Positive Roll Over Test")
53
Rationale for HYPERTENSION
The blood pressure rises due to: ARTERIOLAR VASOSPASMS AND VASOCONSTRICTION causing (Narrowing of the blood vessels) an increase in peripheral resistance fluid forced out of vessels HEMOCONCENTRATION Increased blood viscosity = Increased hematocrit
 an increase in peripheral resistance. fluid forced out of vessels. HEMOCONCENTRATION. Increased blood viscosity = Increased hematocrit.")
54
Key Point to Remember ! HEMOCONCENTRATION develops because:
Vessels became narrowed forcing fluid to shift Fluid leaves the intracellular spaces and moves to extracellular spaces Now the blood viscosity is increased (Hemocrit is increased) **Very difficult to circulate thick blood 12 12 12
 **Very difficult to circulate thick blood")
55
Test Yourself ! Which of these readings indicates hypertension in the patient whose blood pressure normally is 100 / 60 and MAP of 77? a. 120 / 76; MAP 96 b. 110 / 70; MAP 83 c. 130 / 80; MAP 98 d. 125 / 70; MAP 88 13 13 13

56
Proteinuria With Renal vasospasms, narrowing of glomular capillaries which leads to decreased renal perfusion and decreased glomerular filtration rate (damage to glomeruli) PROTEINURIA Spilling of 1+ of protein is significant to begin treatment Oliguria and tubular necrosis may precipitate acute renal failure 16 16 16
 PROTEINURIA. Spilling of 1+ of protein is significant to begin treatment. Oliguria and tubular necrosis may precipitate. acute renal failure")
57
Significant Lab Work Changes in Serum Chemistry
Decreased urine creatinine clearance ( mL/ min) Increased BUN (12-30 mg./dl.) Increased serum creatinine ( mg./dl) Increased serum uric acid ( mg./dl.) Question 17
 Increased BUN (12-30 mg./dl.) Increased serum creatinine ( mg./dl) Increased serum uric acid ( mg./dl.) Question 17.")
58
Weight Gain and Edema Edema may appear rapidly
Clinical Manifestation: Edema may appear rapidly Begins in lower extremities and moves upward Pitting edema and facial edema are late signs Weight gain is directly related to accumulation of fluid

59
WEIGHT GAIN AND EDEMA Rationale:
Decreased blood flow to the kidneys causes a loss of plasma proteins and albumin This leads to a decreased colloid osmotic pressure. A in COP allows fluid to shift from from intravascular to extravascular. Now there is an accumulation of fluid in the tissues. Increased angiotensin and aldostersone triggers retention of sodium and water. 14 14 14

60
The Nurse Must Know The difference between dependent edema and generalized edema is important. The patient with PIH has generalized edema because fluid is in all tissues.

61
Decreased Placental Perfusion and Placental Aging
With Vasospasms and Vasoconstriction of the the vessels in the placenta. Decreased Placental Perfusion and Placental Aging Positive OCT / __________Decelerations With Prolonged decreased Placental Perfusion: Fetal Growth is retarded - IUGR, SGA 17 17 17

62
Condition is Worsening

63
Oliguria – 100ml./4 hrs or less than 30 cc. / hour
Edema moves upward and becomes generalized (face, periorbital, sacral) Excessive weight gain – greater than 2 pounds per week
 Excessive weight gain – greater than 2 pounds per week.")
64
Central Nervous System Changes
Cerebral edema -- forcing of fluids to extracellular Headaches -- severe, continuous Hyperreflexia Level of Consciousness changes – changes in affect Convulsions / seizures

65
Visual Changes Retinal Edema and spasms leads to: Blurred vision
Double vision Retinal detachment Scotoma (areas of absent or depressed vision)
")
66
Nausea and Vomiting Epigastric pain –often sign of impending coma

67
Pre-Eclampsia Mild Severe
B/P / /110 Protein Edema , lower legs Weight <1 lb. / week >2lb. / week Reflexes brisk (Hyperreflexia) Clonus present Retina Blurred vision, Scotoma Retinal detachment GI, Hepatic N & V, Epigastric pain, changes in liver enzymes CNS Headache, LOC changes Fetus Premature aging of placenta IUGR; late decelerations Question 16 18 18 18
 Clonus present. Retina 0 Blurred vision, Scotoma. Retinal detachment. GI, Hepatic 0 N & V, Epigastric pain, changes in liver enzymes. CNS 0 Headache, LOC changes. Fetus 0 Premature aging of placenta. IUGR; late decelerations. Question")
68
Interventions and Nursing Care
Home Management Decrease activities and promote bed rest Sedative drugs Lie in left lateral position Remain quiet and calm – restrict visitors and phone calls Dietary modifications increase protein intake to g/day maintain sodium intake Caffeine avoidance Weigh daily at the same time Keep record of fetal movement - kick counts Check urine for Protein Question 18 20

69
Hospitalization CBC, platelets; type and cross match
If symptoms do not get better then the patient needs to be hospitalized in order to further evaluate her condition. Common lab studies: CBC, platelets; type and cross match Renal blood studies -- BUN, creatitine, uric acid Liver studies -- AST, LDH, Bilirubin DIC profile -- platelets, fibrinogen, FSP, D-Dimer

70
Hospital Management Nursing Care Goal
1. Decrease CNS Irritability 2. Control Blood Pressure 3. Promote Diuresis 4. Monitor Fetal Well-Being 5. Deliver the Infant 20 21 21

71
Decrease CNS Irritability
Provide for a Quiet Environment and Rest 1. MONITOR EXTERNAL STIMULI Explain plans and provide Emotional Support Administer Medications 1. Anticonvulsant -- Magnesium Sulfate 2. Sedative -- Diazepam (Valium) 3. Apresoline (hydralazine) Assess Reflexes Assess Subjective Symptoms Keep Emergency Supplies Available 21 22 22
 3. Apresoline (hydralazine) Assess Reflexes. Assess Subjective Symptoms. Keep Emergency Supplies Available")
72
Magnesium Sulfate ACTION CNS Depressant, reduces CNS irritability Calcium channel blocker- inhibits cerebral neurotransmitter release ROUTE IV effect is immediate and lasts 30 min. IM onset in 1 hour and lasts 3-4 hours Prior to administration: Insert a foley catheter with urimeter for assessment of hourly output 22 23 23

73
Magnesium Sulfate NURSING IMPLICATIONS
1. Monitor respirations > 14-16; < 12 is critical 2. Assess reflexes for hyporeflexia -- D/C for hyporeflexia 3. Measure Urinary Output >100cc in 4 hrs. 4. Measure Magnesium levels – normal is mg/dl Therapeutic is 4-8mg/dl.; Toxicity - >9mg/dl; Absence of reflexes is >10 mg/dl; Respiratory arrest is mg/dl; Cardiac arrest is > 15 mg/dl. Have Calcium Gluconate available as antagonist

74
Test Yourself ! A Woman taking Magnesium Sulfate has a
respiratory rate of 10. In addition to discontinuing the medication, the nurse should: a. Vigorously stimulate the woman b. Administer Calcium gluconate c. Instruct her to take deep breaths d. Increase her IV fluids 23 24 24

75
Nursing Care: Hospital Management
1. Decrease CNS Irritability 2. Control Blood Pressure 3. Promote Diuresis 4. Monitor Fetal Well-Being 5. Deliver the Infant 20 21 21

76
Control Blood Pressure
Check B / P frequently. Give Antihypertensive Drugs Hydralzine ( apresoline) Labetalol Aldomet Procardia Check Hemocrit Do NOT want to decrease the B/P too low or too rapidly. Best to keep diastolic ~90. WHY? 24 25 25
 Labetalol. Aldomet. Procardia. Check Hemocrit. Do NOT want to decrease the B/P too low or too rapidly. Best to keep diastolic ~90. WHY")
77
Nursing Care: Hospital Management
1. Decrease CNS Irritability 2. Control Blood Pressure 3. Promote Diuresis 4. Monitor Fetal Well-Being 5. Deliver the Infant 20 21 21

78
Promote Diuresis **Don’t give Diuretic, masks the symptoms of PIH
Bed rest in left or right lateral position Check hourly output -- foley cath with urimeter Dipstick for Protein Weigh daily -- same time, same scale 25 26 26

79
Nursing Care: Hospital Management
1. Decrease CNS Irritability 2. Control Blood Pressure 3. Promote Diuresis 4. Monitor Fetal Well-Being 5. Deliver the Infant 20 21 21

80
Monitor Fetal Well-Being
FETAL MONITORING-- assessing for late decelerations. NST -- Non-stress test OCT --oxytocin challenge test If all else fails ---- Deliver the baby 26 27 27

81
Key Point to Remember ! SEVERE COMPLICATIONS OF PIH:
PLACENTAL SEPARATION - ABRUPTIO PLACENTA; DIC PULMONARY EDEMA RENAL FAILURE CARDIOVASCULAR ACCIDENT IUGR; FETAL DEATH HELLP SYNDROME 19 19 19

82
HELLP Syndrome A multisystem condition that is a form of severe preeclampsia - eclampsia H = hemolysis of RBC EL = elevated liver enzymes LP = low platelets <100,000mm (thrombocytopenia) Question 19 28 28
 Question")
83
Etiology of HELLP Hemolysis occurs from destruction of RBC’s
Release of bilirubin Elevated liver enzymes occur from blood flow that is obstructed in the liver due to fibrin deposits Vascular vasoconstriction endothelial damage platelet aggregation at the sites of damage low platelets.

84
HELLP Syndrome Assessment:
1. Right upper quadrant pain and tenderness 2. Nausea and vomiting 3. Edema 4. Flu like symptoms 5. Lab work reveals – a. anemia – low Hemoglobin b. thrombocytopenia – low platelets. < 100,000. c. elevated liver enzymes: -AST asparatate aminotransferase (formerly SGOT) exists within the liver cells and with damage to liver cells, the AST levels rise > 20 u/L. - LDH – when cells of the liver are lysed, they spill into the bloodstream and there is an increase in serum > 90 u/L/
 exists within the liver cells and with. damage to liver cells, the AST levels rise > 20 u/L. - LDH – when cells of the liver are lysed, they spill. into the bloodstream and there is an increase in. serum > 90 u/L/")
85
HELLP Intervention: 1. Bedrest – any trauma or increase in intra-
abdominal pressure could lead to rupture of the liver capsule hematoma. 2. Volume expanders 3. Antithrombic medications

86
Infections

87
Urinary Tract Infection
Most common infection complicating Pregnancy Etiology Pressure on ureters and bladder causing Stasis with compression of ureters Reflux Hormonal effects cause decrease tone of bladder Assessment Dysuria, frequency, urgency lower abdominal pain; costal vertebral pain fever 25 25

88
Interventions Knee chest position Complication Monthly cultures
Oral Sulfonamides; Amoxicillin, Ampicillin, Cephalosporins, NO tetracyclines Increase fluid intake to 3 – 4 liters / day Knee chest position Complication Premature labor

89
T O R C H A Infections T = Toxoplasmosis O = Other R = Rubella
Syphilis, Gonorrhea, Chlamydial,Hepatitis A or B R = Rubella C = Cytomegalovirus H = Herpes A = Aids Question 20 26 26

90
Toxoplasmosis Etiology Maternal and Fetal Effects
Protozoan infection. Raw meat and cat litter Maternal and Fetal Effects Mom - flu-like symptoms, lymphadenopathy Fetus – stillborn, premature birth, microcephaly; mental retardation Interventions / Nursing Care * Instruct to cook meat thoroughly * Avoid changing cat litter * Advise to wear gloves when working in the garden Treatment: Sulfa drugs 27 27

91
Syphilis Etiology Maternal and Fetal Effects
Spirochete – Treponema Pallium Maternal and Fetal Effects May pass across the placenta to fetus causing spontaneous abortion. Major cause of late,second trimester abortions Infant born with congenital anomalies 28 28

92
Syphilis Intervention: 1. Penicillin
2. Advise to return for prenatal visits monthly to assess for reinfection. 3. Advise that if treated early, fetus may not be infected

93
Gonorrhea Treated with Etiology – Neisseria Gonorrhoeae
Maternal and Fetal Effects: May get infected during vaginal delivery causing Ophthalmia neonatorium (blindness) in the infant Mom will experience dysuria, frequency, urgency Major cause Pelvic Inflammatory Disease which leads to infertility. Treated with Rocephin Spectinomycin Treat partner!! 29 29
 in the infant. Mom will experience dysuria, frequency, urgency. Major cause Pelvic Inflammatory Disease which leads to infertility. Treated with. Rocephin. Spectinomycin. Treat partner!!")
94
Chlamydia Maternal and Fetal Effects
Three times more common than gonorrhea. Etiology - Chlamydia trachomatis Maternal and Fetal Effects Mom – pelvic inflammatory disease, dysuria, abortions, pre-term labor Fetus -- Stillbirth, Chylamydial pneumonia Interventions Erythromycin, doxycycline, zithromax Advise treatment of both partners is very important 30 30

95
Hepatitis A or B Highly contagious when transmitted by direct contact with blood or body fluids Maternal and Fetal Effects: All moms should be tested for Hep B during pregnancy Fetus may be born with low birth weight and liver changes\ May be infected through placenta, at time of birth, or breast milk Intervention: Recommend Hepatitis B vaccination to both mother and baby after delivery. 31

96
Rubella Etiology Spread by droplet infection or through direct contact with articles contaminated with nasopharyngeal secretions. Crosses placenta Maternal and Fetal Effects Mom– fever, general malaise, rash Most serious problem is to the fetus--causes many congenital anomalies (cataracts, heart defects) Intervention Determine immune status of mother. If titer is low, vaccine given in early postpartum period 32 32
 Intervention. Determine immune status of mother. If titer is low, vaccine given in early postpartum period")
97
CYTOMEGALOVIRUS Etiology -- Member of the Herpes virus
Crosses the placenta to the fetus or contracted during delivery. Cannot breast feed because transmitted through breast milk Effects on Mom and Fetus Mom – no symptoms, not know until after birth of the baby Fetus -- Severe brain damage; Eye damage Intervention No drug available at this time Teach mom should not breast feed baby Isolate baby after birth 33 33

98
Herpes Simplex Type 2 Maternal and Fetal Effects
Painful lesions, blisters that may rupture and leave shallow lesions that crust over and disappear in 2-6 weeks Culture lesions to detect if Herpes, No cure If mom has an outbreak close to delivery, then cannot deliver vaginally. Must deliver by Cesarean birth *Virus is lethal to fetus if inoculated at birth Intervention: Zivorax 34 34

99
AIDS Etiology: Human Immunodeficiency Virus, HIV
Transmission of HIV to the fetus occurs through: The placenta; birth canal Through breast milk **The virus must enter the baby’s bloodstream to produce infection. 35 35

100
Maternal and Fetal Effects:
Mom - brief febrile illness after exposure to with symptoms of fatigue and lymphadenopathy Fetus has a 2-5% chance of being infected. No symptoms until about 1 year of age Diagnosis: The mother can be diagnosed by the ELISA test and confirmed using the Western Blot. Assessment of viral load, CD4 cell count Goal: reduce viral load to below 50 copies /ml. and increase the CD4 cell count. Question 21 36 36

101
Diagnosis: ELISA test – identifies antibodies specific to HIV. If positive = person has been exposed and formed antibodies Western Blot – used to confirm seropositivity when ELISA is positive. Viral load - measures HIV RNA in plasma. It is used to predict severity – lower the load the longer survival. CD4 cell count – markers found on lymphocytes to indicate helper T4 cells. HIV kills CD4 cells which results in impaired immune system. Goal: reduce viral load to below 50 copies /ml. and increase the CD4 cell count.

102
Nursing Care: **Provide Emotional Support
**Teach measures to promote wellness AZT – oral during pregnancy; IV during labor, liquid to newborn for 6 weeks. **Provide information about resources

103
Fetal Demise / Intrauterine Fetal Death
DEFINITION: Death of a fetus after the age of viability 2 2 2

104
Assessment: 1. First indication is usually NO fetal movement 2. NO fetal heart tones Confirmed by ultrasound 3. Decrease in the signs and symptoms of pregnancy

105
Treatment: Deliver the fetus How???

106
Pre-Gestational Onset Disorders

107
Substance Abuse Drugs that commonly misused are:
Tobacco Alcohol Cocaine Marijuana Amphetamines, barbiturates , hallucinogens Heroin Others Effects – vary depending on the drug, time exposed, etc. See table 14-1.

108
Substance Abuse Patient Teaching
Very dangerous to use any drugs during the first 8 weeks of gestation Drugs that cross the placenta may cause possible problems in the infant: mental retardation Microcephaly FAS IUGR Congenital heart defects

109
Diabetes in Pregnancy

110
Diabetes in Pregnancy Diabetes creates special problems which affect pregnancy in a variety of ways. Successful delivery requires work of the entire health care team 13 13

111
Endocrine Changes During Pregnancy
There is an increase in activity of maternal pancreatic islets which result in increase production of insulin. 15 15

112
Counterbalanced by: Placenta’s production of Human Chorionic Somatomammotropin (HCS) Increased levels of progesterone and estrogen--antagonistic to insulin Human placenta lactogen – reduces effectiveness of circulating insulin d. Placenta enzyme-- insulinase 16 16

113
GESTATIONAL DIABETES Diabetes diagnosed during pregnancy, but unidentifable in non-pregnant woman Known as Type III Diabetes - intolerance to glucose during pregnancy with return to normal glucose tolerance within 24 hours after delivery Glucose tolerance test: 3 hr oral gtt – check levels at 1,2,3 hours Gestational diabetes if: Fasting – 95 mg / dl 1 hour mg/ dl 2 hour mg/ dl 3 hour – 140mg/dl 17 17

114
Treatment for the patient with Gestational Diabetes:
Treatment - controlled mainly by diet No use of oral hypoglycemics

115
Effects of Diabetes on the Pregnancy
MATERNAL Increase incidence of INFECTION Fourfold greater incidence of Pre-eclampsia Increase incidence of Polyhydramnios Dystocia – large babies Rapid Aging of Placenta 21 21

116
FETAL COMPLICATIONS Increase morbidity Increase Congenital Anomalies
neural tube defect (AFP) Cardiac anomalies Spontaneous Abortions Large for Gestation Baby, LGA Increase risk of RDS 22 22
 Cardiac anomalies. Spontaneous Abortions. Large for Gestation Baby, LGA. Increase risk of RDS")
117
Effects of Pregnancy on the Diabetic
Insulin Requirements are Altered First Trimester--may drop slightly Second Trimester-- Rise in the requirements Third Trimester-- double to quadruple by the end of pregnancy Fluctuations harder to control; more prone to DKA Possible acceleration of vascular diseases 18 18

118
Key Point to Remember! If the insulin requirements do not rise as pregnancy progresses that is an indication that the placenta is not functioning well. 19 19

119
Test Yourself? Mrs. R.’s is 31 weeks gestation and her insulin requirements have dropped. What additional test could be performed to assess fetal well-being? a. L/S ratio b. Estriol levels c. Oxytocin Challenge Test 20 20

120
Interventions /Nursing Care
I. Diet Therapy dietary management must be based on BLOOD GLUCOSE LEVELS Pre-pregnant diet usually will not work II. Insulin Regulation maintaining optimal blood glucose levels require careful regulation of insulin. Sometimes placed on insulin pump. III. Blood Glucose Monitoring teach how to keep a record of results of home glucose monitoring 23 23

121
IV. EXERCISE A consistent and structured exercise program is O.K.
V. MONITOR FETAL WELL-BEING The objective is to deliver the infant as near to term as possible and prevent unnecessary prematurity NST Ultrasound L / S ratio 24 24

122
Heart Disease in Pregnancy

123
Cardiac Response in All Pregnancies
Every Pregnancy affects the cardiovascular system Increase in Cardiac Output 30% - 50% Expanded Plasma Volume Increase in Blood (Intravascular) Volume A woman with a healthy heart can tolerate the stress of pregnancy,but a woman with a compromised heart is challenged Hemodynamically and will have complications 1 1
 Volume. A woman with a healthy heart can tolerate the stress of. pregnancy,but a woman with a compromised heart is. challenged Hemodynamically and will have complications")
124
Effects of Heart Disease on Pregnancy
Growth Retarded Fetus Spontaneous Abortion Premature Labor and Delivery 2 2

125
Effects of Pregnancy on Heart Disease
The Stress of Pregnancy on an already weakened heart may lead to cardiac decompensation (failure). The effect may be varied depending upon the classification of the disease 3 3
. The effect may be varied depending upon the classification of the disease")
126
Classification of Heart Disease
Uncompromised No alteration in activity No anginal pain, no symptoms with activity Class 2 Slight limitation of physical activity Dyspnea, fatigue, palpitations on ordinary exertion comfortable at rest p. 669 4 4

127
Class 3 Class 4 Marked limitation of physical activity
Excessive fatigue and dyspnea on minimal exertion Anginal pain with less than ordinary exertion Class 4 Symptoms of cardiac insufficiency even at rest Inability to perform any activity without discomfort Anginal pain Maternal and fetal risks are high p. 669 5 5

128
Nursing Care - Antepartum
Decrease Stress Teach the importance of REST! watch weight assess for infections - stay away from crowds assess for anemia assess home responsibilities Teach signs of cardiac decompenstion 6 6

129
Key Point to Remember Signs of Congestive Heart Failure
Cough (frequent, productive, hemoptysis) Dyspnea, Shortness of breath, orthopnea Palpitations of the heart Generalized edema, pitting edema of legs and feet Moist rales in lower lobes, indicating pulmonary edema 9 9
 Dyspnea, Shortness of breath, orthopnea. Palpitations of the heart. Generalized edema, pitting edema of legs and feet. Moist rales in lower lobes, indicating pulmonary edema")
130
low in sodium and calories ( fat )
Teach about diet high in iron, protein low in sodium and calories ( fat ) Watch weight gain Teach how to take their medicine Supplemental iron Heparin, not coumarin – monitor lab work Diuretics – very careful monitoring Antiarrhythmics –Digoxin, quinidine, procainamide. *Beta-blockers are associated with fetal defects. Reinforce physicians care 7 7
 Watch weight gain. Teach how to take their medicine. Supplemental iron. Heparin, not coumarin – monitor lab work. Diuretics – very careful monitoring. Antiarrhythmics –Digoxin, quinidine, procainamide. *Beta-blockers are associated with fetal defects. Reinforce physicians care")
131
Key point to remember ! Never eat foods high in Vitamin K while on
an anticoagulant! ( raw green leafy vegetables) 8 8
")
132
Nursing Care: Intrapartum
Labor in an upright or side lying position Restrict fluids On O2 per mask throughout labor and cardiac monitoring. Sedation / epidural given early Report fetal distress or cardiac failure Stage 2 - gentle pushing, high forceps delivery 10 10

133
Nursing Care Postpartum
The immediate post delivery period is the MOST significant and dangerous for the mom with cardiac problems Following delivery, fluid shifts from extravascular spaces into the blood stream for excretion Cardiac output increases, blood volume increases Strain on the heart! Watch for cardiac failure 11 11

134
Test Yourself ! Mrs. B. has mitral valve prolapse. During the second trimester of pregnancy, she reports fatigue and palpitations during routine housework. As a cardiac patient, what would her functional classification be at this time? a. Class I b. Class II c. Class III d. Class IV 12 12

135
The End

Similar presentations
















 – presence of severe birth defects in babies born to mothers who drink alcohol during pregnancy. Includes damage.>")


