Download presentation
Presentation is loading. Please wait.

1
How do professional record standards support timely communication and information flows for all participants in health and social care? 1 Gurminder Khamba Clinical Lead for Secondary Care Gurminder.khamba@hscic.gov.uk

2
Outline The Need For Standards Clinical Document Generic Record Standards PRSB CDA

6
Sharing of clinical information across systems –allows new ways of working –reduces repetition of work –reduces potential errors –allows safe and consistent sharing of information –supports Information Governance

7
Information Flow Primary Care Secondary Care Social Care Allied Professions Message

9
Clinical Message It’s about the patient and their problem Problem being chest pain, arm pain, leg pain etc. It needs context –Background of other medical problems, medications, living conditions What we want done with it

10
Does he have Ischaemic Heart Disease? Patient A Has Chest Pain Needs Physiotherapy and Occupational therapy Patient B having difficulty mobilising Need to work with Social Services Patient C needs Residential Placement

11
Information Stored Primary Care Secondary Care Social Care Clinical Message

12
However the information stored in each system is unique The terminologies and classifications for each system use nomenclature and coding schema which are not easily made compatible

13
Clinical Translation JapaneseArabicRussian Translation

14
How we Share Information Verbal Letters Fax Email PDF Spreadsheet

15
However we would like to be more clever with information exchange. Clinicians and Systems are expecting standard information –Demographics, Problem list, Medications etc.

16
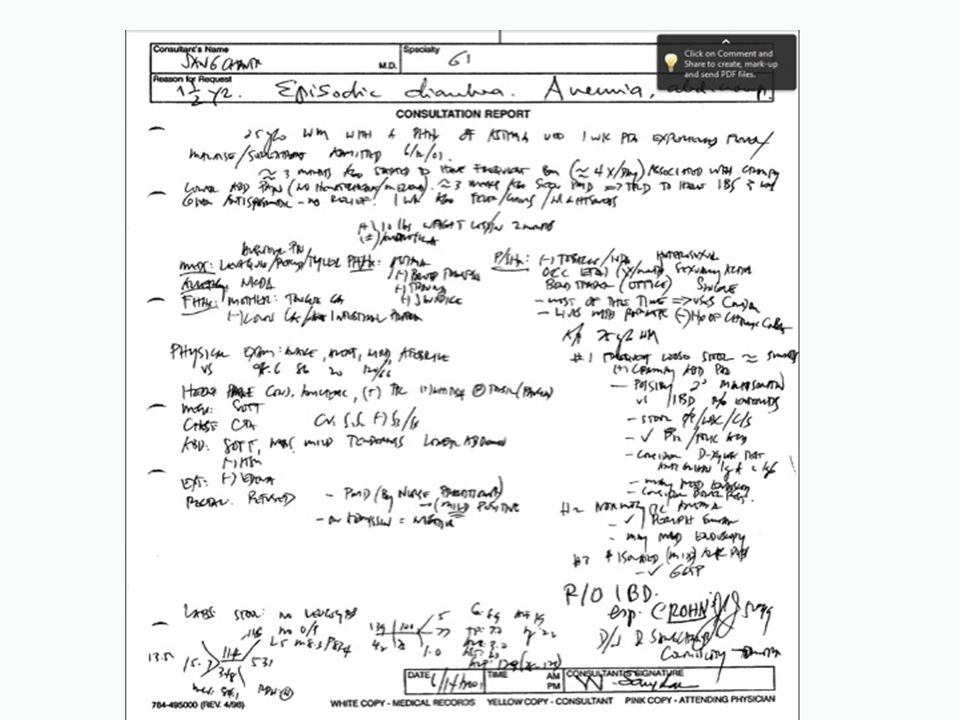
The Clinical Model Clinical Documentation has a certain workflow to it which is universal to clinical method used by clinicians

17
The clinical document for it to make sense is hierarchal and structured. Each of the sections contains information which is pertinent and logical and often context and time sensitive.

18
Presenting Complaint History of Presenting Complaint Medications Results Differential Plan

19
Core Clinical Model

20
There is no reason why certain information under these sections cannot be used to pre-populate for the destination system However, Computer Systems are simple

21
Computers need to be told everything all the time “Medications history” and “Drug history” might mean the same to a human But to a computer it is completely different.

22
Standardisation Therefore, these headings need to be standardised and used uniformly across the health and social care spectrum.

23
2008 documentation available from RCP and AoMRC websites

26
Initial Priorities Deployment of a full set of electronic referral, transfer & discharge documents, incorporating the core model for clinical coded data Fully assured technical standards with agreed professional data components Focus on specific use cases based on market demand e.g. Medications, Mental Health Discharge Summary

27
April 2013

28
Founder Members National VoicesRoyal College of Physicians Allied Health Professions FederationRoyal College of Nursing British Computer SocietyRoyal College of General Practitioners Royal College of PathologistsAcademy of Medical Royal Colleges Royal College of Surgeons of England Royal College of Psychiatrists Association of Directors of Adult Social Services Royal College of Paediatrics and Child Health

29
PRSB - Functions PRSB Quality Assurance Coherence Brokerage Advice

30
PRSB - Value Proposition One Stop Shop Patient View Increased Adoption Increase d Quality Reduced Cost and Timescale

31
CLINICAL DOCUMENT ARCHITECTURE

32
Level 1 – CDA Header is Described – Document Type(s) Level 2 – Assumes XML Body Content – Prescribes: the Sections, their Order and Section Identifier Codes Level 3 – CDA Entries – Vocabulary [Codes] – Relationships – Semantics Header Body Section Entries
![Level 1 – CDA Header is Described – Document Type(s) Level 2 – Assumes XML Body Content – Prescribes: the Sections, their Order and Section Identifier Codes Level 3 – CDA Entries – Vocabulary [Codes] – Relationships – Semantics Header Body Section Entries](http://images.slideplayer.com/24/7037977/slides/slide_32.jpg "Level 1 – CDA Header is Described – Document Type(s) Level 2 – Assumes XML Body Content – Prescribes: the Sections, their Order and Section Identifier Codes Level 3 – CDA Entries – Vocabulary [Codes] – Relationships – Semantics Header Body Section Entries")
33
Header Document Type Sender Receiver Patient Body Section(s) Admission Details Primary/Secondary Diagnosis Observations Medications Follow-up Entries Admission Details Primary/Secondary Diagnosis Observations Medications CODEDCODED TEXTTEXT
 Admission Details Primary/Secondary Diagnosis Observations Medications Follow-up Entries Admission Details Primary/Secondary Diagnosis Observations Medications CODEDCODED TEXTTEXT")
34
Newcastle Discharge Venogram done 13/6/12 Arrived on system 13/6/12

35
Standards which are professionally assured are needed to ensure that information can flow across systems and care settings By ensuring that standards are built into clinical documentation, the use of data to provide information to help guide service will add much valued insight.

Similar presentations








![Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.](/12/3498778/big_thumb.jpg "Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.>")










 Information Standards.>")

