Download presentation
Presentation is loading. Please wait.

1
Diagnosis and treatment of neuroendocrine tumors Dan Granberg

3
Neuroendocrine tumors Carcinoids – – Bronchial – – Thymic – – Gastric – – Duodenal – – Small bowel – – Appendiceal – – Large bowel – – Rectal Endocrine pancreatic tumors – – Gastrinomas – – Insulinomas – – Glucagonomas – – VIPomas – – Somatostatinomas – – Non-functioning – – Mixed

4
Diagnosis Biochemistry Radiology – – CT – – MRI – – Ultrasonography – – Endoscopic ultrasonography Somatostatin receptor scintigraphy = octreoscan Positron emission tomography = PET Biopsy Echocardiography Endoscopy

5
Histopathology – Tumour biology Neuroendocrine markers – Chromogranin A – Synaptophysin Specific markers – gastrin, serotonin Proliferation marker – Ki-67, PCNA Adhesion molecules – CD44 Angiogenic factors – VEGF, bFGF, TGF Tyrosine kinase receptors Somatostatin receptors – SSTR 1-5

7
Biochemistry P-chromogranin A (P-chromogranin B) U-5’HIAA U-MeImAA P-ACTH U-cortisol S-gastrin S-PP (pancreatic polypeptide) P-glucagon P-VIP S-calcitonin S-insulin S-proinsulin S-C-peptide Secretin test Gastric pH 72-hour fasting Meal stimulation test
 U-5’HIAA U-MeImAA P-ACTH U-cortisol S-gastrin S-PP (pancreatic polypeptide) P-glucagon P-VIP S-calcitonin S-insulin S-proinsulin S-C-peptide Secretin test Gastric pH 72-hour fasting Meal stimulation test")
8
Biochemistry P-chromogranin A: Most sensitive marker Early detection of recurrence (Welin et al) Treatment monitoring Pitfalls – – Impaired renal function – – Treatment with proton pump inhibitors – – Chronic atrophic gastritis – – Inflammatory bowel disease – – Decreased liver function – – High spontaneous variation
 Treatment monitoring Pitfalls – – Impaired renal function – – Treatment with proton pump inhibitors – – Chronic atrophic gastritis – – Inflammatory bowel disease – – Decreased liver function – – High spontaneous variation")
9
Plasma chromogranin A Spontaneous variation Patients: Midgut carcinoid 21 Sporadic EPT 12 MEN1 with EPT 7 Healthy subjects 8 Total 48 Plasma chromogranin A measured on 2 consecutive days Granberg 1999

10
Plasma chromogranin A Spontaneous variation Results: DiagnosisnMean variation Tumor patients4029% (0–113.5%) Elevated CgA3729.5% (0–113.5%) Normal CgA327% (9–39%) Healthy subjects821% (0–47%) Granberg 1999
 Elevated CgA3729.5% (0–113.5%) Normal CgA327% (9–39%) Healthy subjects821% (0–47%) Granberg 1999")
11
Plasma chromogranin A Spontaneous variation Granberg 1999

12
Radiology CT scan – – native – – i.v. contrast enhancement late arterial phase = portal venous phase venous phase MRI Ultrasonography – – biopsy Endoscopic ultrasonography Intaoperative ultrasonography Echocardiography – – carcinoid heart disease

13
64 patients with GE-NETs Examined by CT, MRI and SRS In 40 pats (62,5%) liver metastases were found Maximum number of lesions detected for each patient (by SRS or CT or MRI) were added = Total number Relative sensitivity = number of lesions detected by method divided by total number of lesions. In a lesion-by-lesion analysis the sensitivities were: SRS49% (204 mets) CT79% (325 mets) MRI 95% (394 mets) Dromain 2005 CT in neuroendolrine tumors
 CT79% (325 mets) MRI 95% (394 mets) Dromain 2005 CT in neuroendolrine tumors.")
20
Somatostatin receptor scintigraphy Neuroendocrine tumors: Carcinoids – – Midgut>90% – – Bronchial 67% Endocrine pancreatic tumors – – Gastrinomas>90% – – Insulinomas<50% Paragangliomas>90% Pheocromocytomas 86% Neuroblastomas 90% Medullary thyroid carcinomas 65%

21
Somatostatin receptor scintigraphy Other malignancies: Small cell lung cancer100% Non small cell lung cancer100% Malignant lymphoma – – Hodgkin’s diease>95% – – Non-Hodgkin’s lymphoma 80% Meningeoma100% Thyroid cancer 80% Pituitary tumors 70-75% Astrocytoma 65% Breast cancer 65%

22
Somatostatin receptor scintigraphy Non-malignant diseases: Sarcoidosis100% Wegener’s granulomatosis100% Tuberculosis 65% Grave’s disease Rheumatoid arthritis100% Sjögren’s syndrome 80% Pneumonia

23
Diagnosis What information does somatostatin receptor scintigraphy provide? Finding occult tumors Staging Surgery Medical treatment Radiotherapy

24
Diagnosis What information does somatostatin receptor scintigraphy provide? Surgery Guidance: Depicts accessible lesions for extirpation

25
Guidance in surgery

27
Intrathoracic metastases of carcinoid

28
after 1st operation ….

29
after 2nd operation…

30
Diagnosis What information does somatostatin receptor scintigraphy provide? Medical treatment Grade of uptake in the tumor allows prediction of value of treatment with Somatostatin analogues (cost effectiveness!)
.")
32
Diagnosis What information does somatostatin receptor scintigraphy provide? Radiotherapy Might depict field of external beam irradiation Grade of uptake: determines feasibility of receptor guided isotope treatment Dosimetry

34
Diagnostic problems Small tumors Staging Grade of malignancy and tumor biology Early detection of residual disease or recurrence Treatment effects

35
Is a technique for in vivo tracer studies labeled with radionuclides ( 11 C, 18 F, 15 O, 68 Ga) biologically unchanged molecules images a physiological principle (receptor binding, metabolism, tissue perfusion, blood flow etc) FDG-PET ( 18 fluorodeoxyglucose) images glucose transport Positron emission tomography (PET)
 biologically unchanged molecules images a physiological principle (receptor binding, metabolism, tissue perfusion, blood flow etc) FDG-PET ( 18 fluorodeoxyglucose) images glucose transport Positron emission tomography (PET)")
36
PET 18 FDG 11 C-methionine 11 C-L-DOPA 18 F-DOPA 11 C-5-Hydroxytryptophane (5-HTP) 11 C-Hydroxyephedrine (HED) 11 C-Metomidate 68 Ga-DOTATOC
 11 C-Hydroxyephedrine (HED) 11 C-Metomidate 68 Ga-DOTATOC")
37
Whole-Body 18 F-DOPA PET for Detection of Gastrointestinal Carcinoid Tumors. Overall sensitivities: 18 F-DOPA 65%, FDG-PET 29% Octreoscan 57%, CT/MRI 73% “PET enabled best localization of primary tumors and lymph node metastases” PET Hoegerle 2001

38
Comparison of PET with 11 C-5-HTP, Octreoscan + SPECT and CT Tumours were imaged by: – PET in 95% (36/38) – SRS in 84% (32/38) – CT in 79% (30/38) PET could visualise the primary tumour in 84% (16/19), compared to SRS in 58% (11/19) and in CT 47% (9/19) of patients In 58% PET could detect more lesions than SRS and CT Örlefors 2005 PET
 – SRS in 84% (32/38) – CT in 79% (30/38) PET could visualise the primary tumour in 84% (16/19), compared to SRS in 58% (11/19) and in CT 47% (9/19) of patients In 58% PET could detect more lesions than SRS and CT Örlefors 2005 PET")
39
Conclusions: 1. 1.Whole-body PET with 11 C-5-HTP can detect more tumors than CT and Octreoscan; staging 2. 2. 11 C-5-HTP can be used in all types of neuroendocrine tumors: general tracer 3. 3.Of value to find small primary tumors, detect residual disease or recurrence 4. 4.FDG-PET in poorly differentiated tumors Örlefors 2005

42
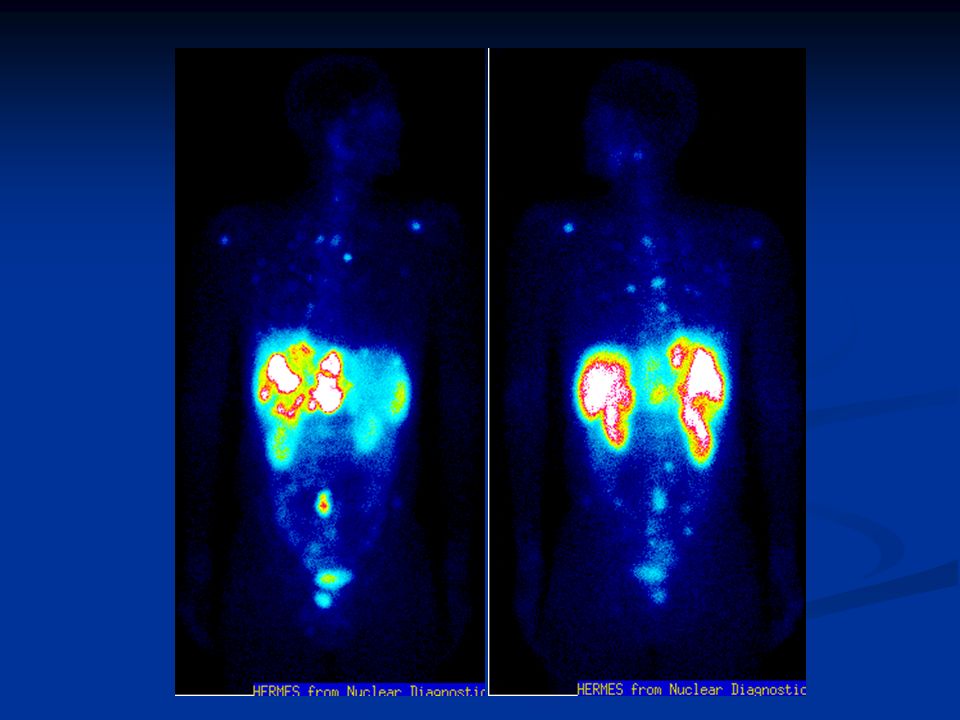
11 C-5-HTP-PET of a patient with elevated gastrin levels showing a duodenal gastrinoma not detected by other methods

43
68 Ga-DOTATOC PET Patients, n=84 Diagnosis of suspected NET, n=13 Staging of histologically proven NET, n=36 Detection of recurrence after therapy, n=35 Endocrine symptoms, n=27, non-functioning, n=57 Comparison with: 111 In-DOTATOC-scintigraphy with SPECT, n=33 n=18 99m Tc-HYNICTOC-scintigraphy with SPECT, n=33 CT Gabriel 2007

44
68 Ga-DOTATOC PET Results: Gabriel 2007 PETSPECTCT Sensitivity97% (69/71)52% (37/71)61% (41/67 Specificity92% (12/13) 71% (12/17) Accuracy96% (81/84)58% (49/84)63% (53/84) Combination of PET and CT: 100% sensitivity Further clinically relevant information in comparison with: Diagnostic CT – 18 patients (21.4%) Scintigraphy – 12 patients (14.3%)
52% (37/71)61% (41/67 Specificity92% (12/13) 71% (12/17) Accuracy96% (81/84)58% (49/84)63% (53/84) Combination of PET and CT: 100% sensitivity Further clinically relevant information in comparison with: Diagnostic CT – 18 patients (21.4%) Scintigraphy – 12 patients (14.3%)")
45
68 Ga-DOTATOC PET Conclusions: PET using 68 Ga-DOTATOC yields higher detection rates compared to 111 In-octreotide scintigraphy and diagnostic CT with clinical impact in a considerable number of patients The combination of PET and CT showed the highest accuracy Gabriel 2007

46
Functional imaging of endocrine tumors with PET is promising Pros: Specific tracers for certain tumors provide excellent visualization. Prospective studies are needed to established the diagnostic efficacy and cost-benefit Cons: Lack of availability ( 11 C-5-HTP, 18 F, 68 Ga) PET/CT will improve morphological localization PET– Conclusion
 PET/CT will improve morphological localization PET– Conclusion.")
47
Treatment Surgery Liver embolization – – Particles – – Chemoembolization – – SIRT Radiofrequency ablation Biotherapy – – Interferon - – – Somatostatin analogs Chemotherapy Targeted irradiation therapy

Similar presentations















 are derived from the diffuse neuroendocrine system, which is made up of.>")






 in Colorectal Cancer Dr Chan Wai Keung Department of Surgery Ruttonjee and Tang Shiu Kin Hospitals.>")







