Download presentation
Presentation is loading. Please wait.

1
Congenital megacolon 浙江大学医学院附属儿童医院 江米足

2
Definition Also called: Description:
Hirschsprung disease, HD Description: characterized by the absence of myenteric and submucosal ganglion cells in the distal intestine; usually affects the last 1-2 feet of the colon, causes problems with the movement in the affected bowel segment, results in an obstruction of the bowel.

4
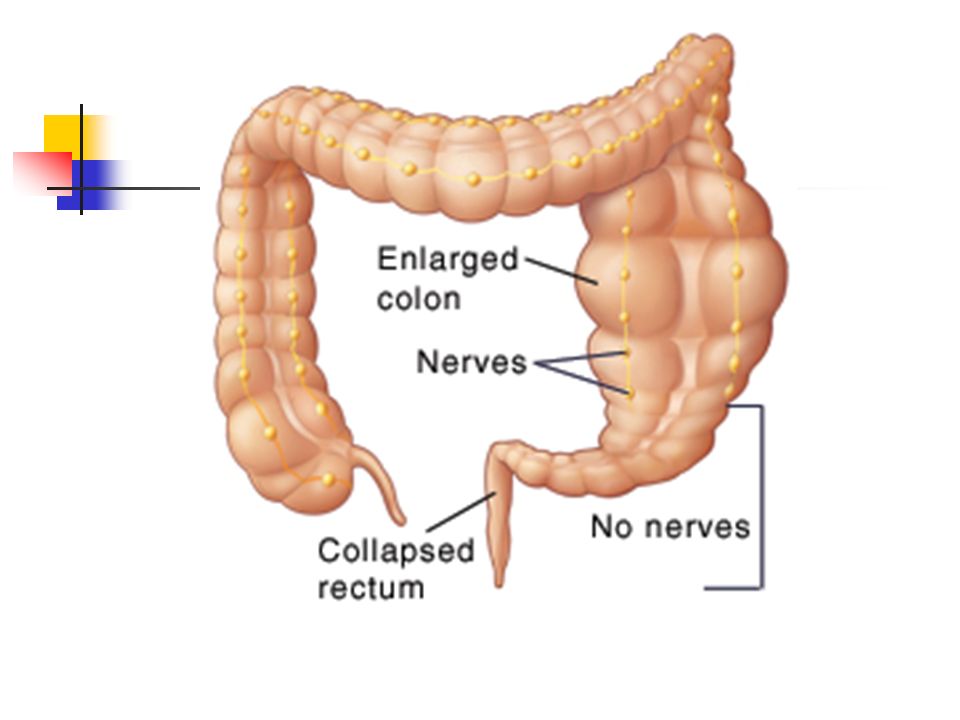
Organs involved aganglionic segment always involves rectum and extends proximally without skip areas dilated colon found proximal to aganglionic segment

5
Histopathology Absence of ganglionic cells
Hypertrophic cholinergic nerve trunks Limited number of adrenergic fiber

6
Who is most affected infancy, may go undiagnosed for years
96% are term infants, 4% are premature infants The male to female ratio is 4:1. If the entire colon is involved, the sex ratio is about 1:1 With an affected sibling, the incidence rises to 12-33% occurs in 0.8% of patients with trisomy 21 Down syndrome Incidence/Prevalence: 1/1,000-1,500 live births

7
Risk factor Risk factors for Hirschsprung's include:
Family members with the disease More common in males May be associated with other congenital defects

8
Causes and pathogenesis
absence of submucosal and myenteric (muscular, Auerbach's) parasympathetic ganglion cells Pathogenesis: neuroblasts from neural crest fail to complete caudal migration to Meissner's and Auerbach's plexuses failure of relaxation/normal peristalsis dilatation of colon
 parasympathetic ganglion cells. Pathogenesis: neuroblasts from neural crest fail to complete caudal migration to Meissner s and Auerbach s plexuses. failure of relaxation/normal peristalsis. dilatation of colon.")
9
Types 1 aganglionic segment limited to rectosigmoid in 80%
colon aganglionic from anus to hepatic flexure in 15% (long segment HD) entire colon lacks ganglion cells in 3% - total colonic aganglionosis, sometimes involves variable segment of distal ileum
 entire colon lacks ganglion cells in 3% - total colonic aganglionosis, sometimes involves variable segment of distal ileum.")
10
Type 2 Classical HD (85% of cases): Rectosegmoid
Short segment HD (10% of cases) Long segment HD (4% of cases) Total colonic aganglionosis (1% of cases) rare variants include the following: Total intestinal aganglionosis Ultra-short-segment HD (involving the distal rectum below the pelvic floor and the anus
 Long segment HD (4% of cases) Total colonic aganglionosis (1% of cases) rare variants include the following: Total intestinal aganglionosis. Ultra-short-segment HD (involving the distal rectum below the pelvic floor and the anus.")
11
History Chief concern (CC):
in infants and older children - overflow diarrhea, vomiting, abdominal distention may be enterocolitis (high mortality rate) early symptoms of megacolon range from complete acute bowel obstruction in neonates to intermittent episodes of chronic constipation in older children
 early symptoms of megacolon range from complete acute bowel obstruction in neonates to intermittent episodes of chronic constipation in older children.")
12
History Chief concern (CC):
sometimes there is diarrhea, episodes of constipation and diarrhea may alternate with periods of apparent normality, diarrhea may develop into a fulminant enterocolitis leading to severe fluid and electrolyte imbalance older children in severe cases may present with failure to thrive (FTT) and can be confused with malabsorption syndromes
 and can be confused with malabsorption syndromes.")
13
History of present illness (HPI)
in infants and older children - suspect any patient with chronic unexplained illness with abnormal bowel pattern dating back to early infancy delayed passage of meconium at birth Past medical history (PMH): in infants and older children - history of obstipation, constipation, failure to thrive
: in infants and older children - history of obstipation, constipation, failure to thrive.")
14
Physical General physical: Abdomen: Rectal:
in newborns - meconium ileus, intestinal obstruction, severe constipation, bilious vomiting, delayed passage of meconium (usually passed within 24 hours, 48 hours in preemies) Abdomen: abdominal distention, occasionally loops of stool-filled bowel palpable Rectal: increased sphincter tone, no stool in rectal vault, classically explosion of watery stool on removal of finger
 Abdomen: abdominal distention, occasionally loops of stool-filled bowel palpable. Rectal: increased sphincter tone, no stool in rectal vault, classically explosion of watery stool on removal of finger.")
15
What are the symptoms? HD is usually diagnosed in infancy, but can also be found later. Symptoms can differ with age

16
Symptoms In newborns In young children In teenagers
Failure to pass meconium within the first 48 hours of life (Meconium is a dark sticky substance that is the first bowel movement) Vomiting after eating Abdominal distention In young children Severe constipation Diarrhea Anemia Growth delay In teenagers Severe constipation for most of their lives
 Vomiting after eating. Abdominal distention. In young children. Severe constipation. Diarrhea. Anemia. Growth delay. In teenagers. Severe constipation for most of their lives.")
17
Rule out intestinal atresia or stenosis, congenital duodenal obstruction imperforate anus necrotizing enterocolitis cystic fibrosis malrotation less causes of neonatal obstruction intussusception Meckel diverticulum duplications medical conditions associated with bilious vomiting and ileus sepsis hypothyroidism meconium plug syndrome

18
“Red flags” for HD diagnosis
Delayed (>24 h) meconium —Present in 70-87% of cases of HD and in <1% of normal children Neonatal constipation —Present in 90-95% of cases but in <7% of children with functional constipation Family history (affected sibling) —Present in 12-33% of cases Poor growth—Present in 25-30% of cases Abdominal distension —Present in 76-85% of cases but in 20% of patients with functional constipation Down’s syndrome and other chromosomal anomalies —HD is present in 1.5% of patients with Down’s syndrome, but 5-10% of patients with Down’s have functional constipation Three or more red flags are present in 18% of patients with the disease. No red flags are present in <1% of patients with the disease
 meconium —Present in 70-87% of cases of HD and in <1% of normal children. Neonatal constipation —Present in 90-95% of cases but in <7% of children with functional constipation. Family history (affected sibling) —Present in 12-33% of cases. Poor growth—Present in 25-30% of cases. Abdominal distension —Present in 76-85% of cases but in 20% of patients with functional constipation. Down’s syndrome and other chromosomal anomalies —HD is present in 1.5% of patients with Down’s syndrome, but 5-10% of patients with Down’s have functional constipation. Three or more red flags are present in 18% of patients with the disease. No red flags are present in <1% of patients with the disease.")
19
Tests for HD diagnosis Barium enema —injection of fluid into the rectum that makes the colon show up on an x-ray Rectal suction biopsy —removal of a sample of bowel tissue to check for ganglia, full-thickness biopsy if necessary Anorectal manometry—measurement of the pressures of the internal and external sphincter with a rectal balloon

20
Imaging studies Plain X ray: air/fluid levels, no air in rectum
Contrast enema: -Narrow distal segment -Funnel-shaped transition zone -Dilation of proximal colon -After hours the contrast material is in the bowel -Mucosal irregularity (enterocolitis)
")
21
Abdominal x ray image showing gaseous distension of the large bowel with air absent from the rectum (typical of HD)
")
22
Biopsy and pathology no ganglion cells in submucosal plexus confirms diagnosis types of rectal biopsies seromuscular biopsy at laparotomy full-thickness transrectal biopsy requires bowel prep, general anesthesia check for Auerbach's plexus alternative - suction biopsy small specimens, requires experienced pathologist can be done at bedside check for Meissner's plexus

23
Anorectal manometry Normal basal internal anal sphincteric tone
No reflex relaxation of the internal sphincter with rectal distention It can be put through safely in newborn age as well

24
The rectoanal inhibitory reflex

25
Other diagnostic testing
Fingerprint chromatogram model of serum protein (3 protein markers) had 100% sensitivity and 100% specificity for identifying HD in 78 serum specimens (42 of HD, 16 of adhesive ileus and 20 normal controls)
 had 100% sensitivity and 100% specificity for identifying HD in 78 serum specimens (42 of HD, 16 of adhesive ileus and 20 normal controls)")
26
Treatment The primary treatment for HD is surgery to remove the affected portion of the colon. There are three potential phases to the surgery, but all three phases may not be needed. Your doctor will discuss the best methods for you or your child's condition.

27
Surgery Colostomy—This involves surgically creating an opening into the colon, which is brought to the abdominal surface. Stool contents are excreted through this opening and into a bag. Pull-through operation—The affected area of the colon is removed, then the healthy colon is brought down to the rectum and joined to the rectal wall. Closure of the colostomy—The colostomy opening is closed, and bowel function gradually returns to normal.

28
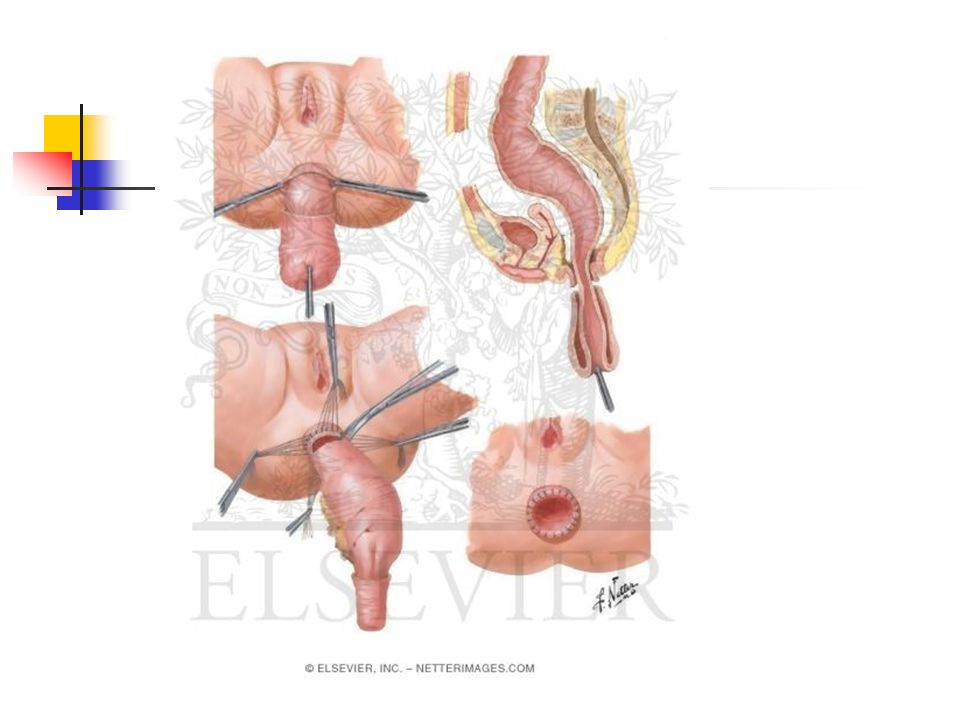
Treatment Transanal Endorectal Pull-Trough
It can be performed safely in infant as well Generally one-stage surgery No abdominal phase The anastomosis is happening in a “safe” place at the pectinate line

30
Operative sequelae Enterocolitis rare but up to 60% mortality
Perforation of the intestine Short gut syndrome Anal dilation may be intermittently necessary if constipation secondary to retained aganglionic internal anal sphincter Occasional incontinence and fecal soiling

31
Outcome Symptoms are eliminated in 90% of children after surgical treatment. A better outcome is associated with early treatment, and shorter bowel segment involvement.

Similar presentations





 Clase 10: Fisiología del colon Dr. Michel Baró A.>")




 Department of Pediatrics>")








