Download presentation
Presentation is loading. Please wait.

1
INTRAVENOUS REOLYSIN IN BONE AND SOFT TISSUE SARCOMA METASTATIC TO LUNG M Mita, MD, MSc Clinical Investigator Assistant Professor of Medicine, IDD at CTRC/UTHSCSA San Antonio

2
BACKGROUND Reolysin (reovirus serotype 3) –Dearing strain, naturally occurring, ubiquitous, non-enveloped human reovirus –Genome 10 segments of double-stranded RNA –Community-acquired infection is mild and limited to the upper respiratory and GI tract. –Virus replicates specifically in transformed cells possessing an activated Ras pathway.

3
BACKGROUND –The preferential lysis of cells with activated Ras pathway by reovirus appears to be due to the inhibition of double-stranded RNA-activated protein kinase (PKR) in these cells. –In cells with Ras non-activated pathway, PKR autophosphorylates in the presence of viral transcripts, which activates it and results in inhibition of viral protein synthesis, thus preventing viral replication. –In cells with activated RAS pathway the autophosphorylation of PKR is inhibited keeping it in an inactive state and allowing viral replication and eventually oncolysis.

4
Reovirus in a cell with non- activated Ras pathway

5
Reovirus growth in a cell with Ras activated pathway

6
RATIONALE Sarcomas –Rare tumors –Very heterogeneous –Incurable when metastatic, median survival 12 m. –Available treatments are few with low RR and high toxicity –There is an acute need for new drugs for treatment of sarcoma

7
RATIONALE in vitro cytotoxicity assays in Ewing’s sarcoma, rhabdomyosarcoma, synovial sarcoma, and osteosarcoma cell lines revealed complete cell kill. (Kolb et al., AACR 2006) in vivo antitumor effect seen in xenograft models of pediatric sarcomas. (Ewing’s sarcoma and rhabdomyosarcoma). In all tumor lines evaluated, the reovirus exhibited significant antitumor activity, including a complete response in a rhabdomyosarcoma line. CONCLUSION : –REOLYSIN demonstrated excellent anti-tumor activity in vitro and in vivo in sarcoma cell lines.
 in vivo antitumor effect seen in xenograft models of pediatric sarcomas. (Ewing’s sarcoma and rhabdomyosarcoma). In all tumor lines evaluated, the reovirus exhibited significant antitumor activity, including a complete response in a rhabdomyosarcoma line. CONCLUSION : –REOLYSIN demonstrated excellent anti-tumor activity in vitro and in vivo in sarcoma cell lines..")
8
PHASE II multi-institutional, open-label, single agent study designed to characterize the efficacy and safety of REOLYSIN given IV every 28 days in patients with bone and soft tissue sarcoma metastatic to lung.

9
OBJECTIVES 1. 1. To measure tumor response and duration of response and describe any evidence of antitumor activity of intravenous multiple dose REOLYSIN in patients with bone and soft tissue sarcomas metastatic to the lung. 2. 2. To evaluate safety of intravenous multiple dose of REOLYSIN

10
STUDY DESIGN IV infusion over 60 minutes days 1-5 REOLYSIN DOSE 3 X 10 10 TCID 50 Simon two-stage design –38 patients will be accrued to the first stage –If 1 or more responses (prolonged SD > 6 months, partial or complete response) up to 52 patients will be accrued –The agent will be considered active if 3 or more responses or prolonged SD are observed
 up to 52 patients will be accrued –The agent will be considered active if 3 or more responses or prolonged SD are observed")
11
INCLUSION CRITERIA Pts with bone or soft tissue sarcoma metastatic to the lung unresponsive to, or untreatable by, standard therapies (histologies include osteosarcoma, Ewing sarcoma family tumors, malignant fibrous histiocytoma, synovial sarcoma, fibrosarcoma, and leiomyosarcoma). The patients must have no sites of active disease other than lungs unless agreed by the sponsor. Have 2 or more measurable metastatic lesions in the lungs detectable on CT scan. (RECIST) At least 16 years of age Have no continuing adverse effects from prior therapies; all such effects must have resolved to CTC AE version 3 ≤ grade 1
 At least 16 years of age Have no continuing adverse effects from prior therapies; all such effects must have resolved to CTC AE version 3 ≤ grade 1.")
12
INCLUSION CRITERIA Have received NO chemotherapy, radiotherapy, immunotherapy, hormonotherapy or surgery within 28 days prior to receiving REOLYSIN ECOG PS ≤ 2 Life expectancy of at least 3 months Laboratory results: –ANC ≥ 1.5 X 10 9 –Plats ≥ 100 X 10 9 –HB ≥ 9.0 g/dl –Creatinine ≤ 1.5 X ULN –Bilirubin ≤ 1.5 X ULN –AST/ALT ≤ ULN –Negative pregnancy test for females of childbearing potential

13
EXCLUSION CRITERIA Concurrent therapy with any other investigational anticancer agent while on study. Have inadequate pulmonary function defined as a forced expiratory volume in 1 second (FEV1) less than 50 % of predicted Be on immunosuppressive therapy; have known HIV infection or active hepatitis B or C Be a pregnant or breast feeding woman Have clinically significant pulmonary or cardiac disease including pre-existing arrhythmia, uncontrolled angina pectoris, myocardial infarction 1 year prior to study entry, or grade 2 or higher compromised LVEF Dementia or altered mental status Any severe, acute or chronic medical or psychiatric condition
 less than 50 % of predicted Be on immunosuppressive therapy; have known HIV infection or active hepatitis B or C Be a pregnant or breast feeding woman Have clinically significant pulmonary or cardiac disease including pre-existing arrhythmia, uncontrolled angina pectoris, myocardial infarction 1 year prior to study entry, or grade 2 or higher compromised LVEF Dementia or altered mental status Any severe, acute or chronic medical or psychiatric condition.")
14
ENROLLMENT 35 patients Tumor types –MFH 8 patients –Synovial sarcoma 8 patients –Osteosarcoma 6 patients –Leiomyosarcoma 6 patients –Undifferentiated round cell sarcoma 1 patient –Ewing sarcoma 1 –Liposarcoma 1 –Rhabdomyosarcoma 1 –Chordoma 1 –High grade sarcoma 1 –Alveolar sarcoma 1

15
PATIENT CHARACTERISTICS Characteristics –35 patients –Age 19-70 (median 51) –Sex Female -16 patients Male -19 patients –PS 0 -12 patients 0 -12 patients 1 - 23 patients 1 - 23 patients
 –Sex Female -16 patients Male -19 patients –PS patients patients patients patients")
16
PREVIOUS TREATMENTS Previous treatment lines for metastatic disease More than 3 lines: 11 patients 1-3 lines: 20 patients None: 4 patients Previous treatments –Chemo only: 15 patients –Chemo and XRT: 11 patients –None: 4 patients –Biological agents: 5 patients (sorafenib, mTOR inhibitors, bevacizumab)
")
17
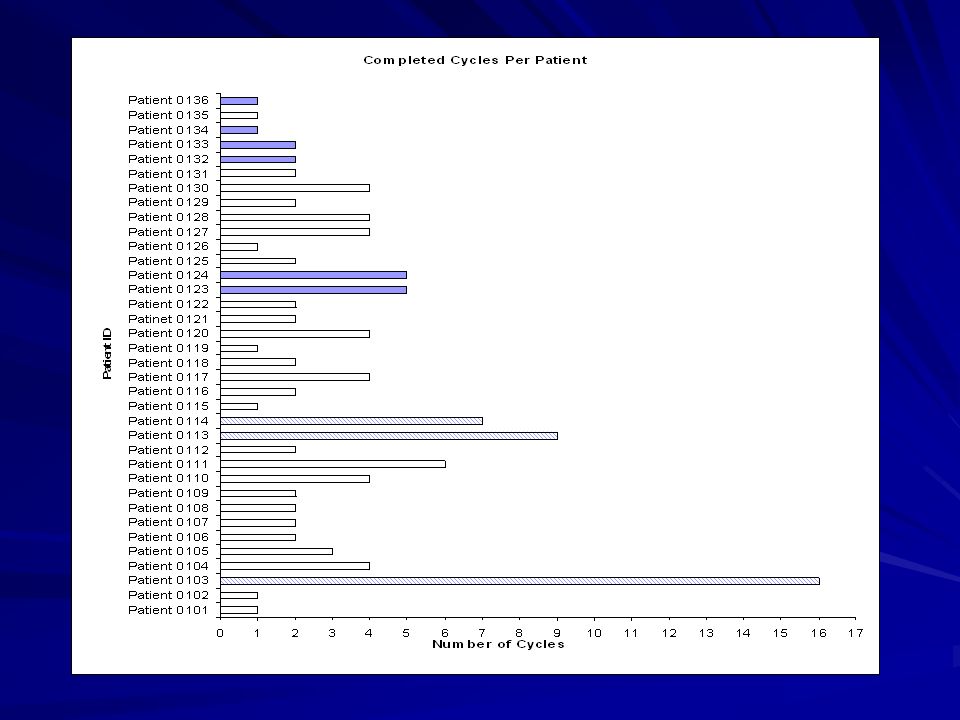
TOXICITIES (based on 25 patients enrolled at IDD) Constitutional grade 1 (fever, chills, fatigue, myalgias): 22 patients Respiratory grade 1 (cough, congestion): 14 patients Gastro-intestinal grade 1 (diarrhea): 10 patients Hematological: occurring during the week of treatment: –Grade 2 ANC: 1 patient; Grade 3 ANC: 3 patients; grade 4 ANC-1 patient (1 day- C2D3, C3D3). –Pt KS (received 16 cycles) grade 2-3 ANC during 13 cycles of treatment (day 3-4). No neutropenia over the last 3 cycles. –Grade 2 thrombocytopenia – 2 patients –Grade 1 anemia- 3 patients. Transaminitis: grade 2 AST/ALT – 1 patient (C1D8, C2D8, C3-5 D 5); grade 1 AST/ALT – 2 patients (C1D3 and C2D3) Palpitations: 2 patients (both with osteosarcoma, large lung mets). 1 patient had objective findings (arrythmia) received B blockers (etiology: possibly hypoxia).
 grade 2-3 ANC during 13 cycles of treatment (day 3-4). No neutropenia over the last 3 cycles. –Grade 2 thrombocytopenia – 2 patients –Grade 1 anemia- 3 patients. Transaminitis: grade 2 AST/ALT – 1 patient (C1D8, C2D8, C3-5 D 5); grade 1 AST/ALT – 2 patients (C1D3 and C2D3) Palpitations: 2 patients (both with osteosarcoma, large lung mets). 1 patient had objective findings (arrythmia) received B blockers (etiology: possibly hypoxia)..")
18
EFFICACY 1 patient (synovial sarcoma) SD after cycle 16 (ongoing). 1 patient Ewing sarcoma SD after 8 cycles (ongoing). 1 patient with osteosarcoma SD after 6 cycles (ongoing). 3 other patients SD after 4 cycles (leiomyosarcoma, chordoma, MFH). 15 patients SD after 2 cycles. 15 patients PD. No tumor reduction. 6/29 patients had SD > 16 weeks 21% 15/29 patients had SD for at least 8 weeks (2-16 months) 52% 4 patients are too early for evaluation; 2 patients came off study before tumor evaluation.
. 1 patient with osteosarcoma SD after 6 cycles (ongoing). 3 other patients SD after 4 cycles (leiomyosarcoma, chordoma, MFH). 15 patients SD after 2 cycles. 15 patients PD. No tumor reduction. 6/29 patients had SD > 16 weeks 21% 15/29 patients had SD for at least 8 weeks (2-16 months) 52% 4 patients are too early for evaluation; 2 patients came off study before tumor evaluation..")
21
CONCLUSION REOLYSIN PHASE II SARCOMA –35 patients enrolled to date –Mild to moderate toxicities –2 nd cycle better tolerated than 1st –3 patients SD for at least 6 months –21% patients SD >16 weeks –52% patients SD for at least 8 weeks

22
CONCLUSION The study achieved the established objectives after the first 33 patients enrolled Enrollment will continue to 52 patients Future studies with Reolysin in combination with chemotherapy are planned in this patient population

23
Acknowledgements IDD at CTRC/UTHSCSA: Tony Carmona, Alain Mita, John Sarantopoulos, Kamalesh Sankhala, Francis Giles Montefiore Medical Center: Sanjay Goel Mayo Clinic: Scott Okuno U Michigan Cancer Center: Rashmi Chugh Oncolytics: Karl Mettinger, Matt Coffey, Brad Thompson, Merle Kirkpatrick, Cathy Ward.

24
THANK YOU

25
The Institute for Drug Development A leader in anticancer drug development

Similar presentations
 CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 E V A L U A.>")

 evaluating the mTOR inhibitor ridaforolimus as maintenance therapy in advanced sarcoma patients.>")
 are a group of highly chemotherapy resistant tumors Doxorubicin is the only APPROVED 1 st line chemotherapy.>")




 STUDY Study Update.>")




 Sant P. Chawla,>")

 upregulation Dose- and time-dependent upregulation of TP in human colon cancer xenografts 20 15 10 5 0 20 15 10 5 0 PaclitaxelDocetaxel.>")
 in Metastatic Castration-Resistant Prostate Cancer (mCRPC): Results from a Phase II Randomized Discontinuation Trial Hussain M et.>")


