Download presentation
Presentation is loading. Please wait.

1
FAHAD ALOSAIMI MD psychiatry and psychosomatic medicine consultant Assistant professor KSU, Riyadh Psychotic disorders theme

2
Psychotic disorders

3
Case of Mr.Schi Mr. Schi is a 28 year-old single male who was brought to Emergency room by his family because of gradual changes in his behavior started 9 months ago. Since then, he became agitated; eat only canned food but not cooked food made by his family, afraid of being poisoned. He talks to himself and stares occasionally on the roof of his room.

4
Case of Mr.Schi He had two brief psychiatric hospitalizations in last 3 years that were precipitated by anger at his neighbor and voices commenting about his behavior. His personal history indicated that he was a healthy child, but his parents report that he was a bed wetter and seemed slower to develop than his brothers and sisters.

5
Analyze the symptoms & signs, both presented and expected in this case including mood, thoughts, cognition, perception and physical aspects. Discuss possible etiological reasons Discuss differential diagnosis

6
Schizophrenia - It is not a single disease but a group of disorders with heterogeneous etiologies. - Found in all societies and countries with equal prevalence & incidence worldwide. - A life prevalence of 0.6 – 1.9 % - Annual incidence of 0.5 – 5.0 per 10,000 - Peak age of onset are 10-25 years for ♂ & 25-35 years for ♀

7
Etiology Exact etiology is unknown. 1- Stress-Diathesis Model: Integrates biological, psychosocial and environmental factors in the etiology of schizophrenia. Symptoms of schizophrenia develop when a person has a specific vulnerability that is acted on by a stressful influence.

8
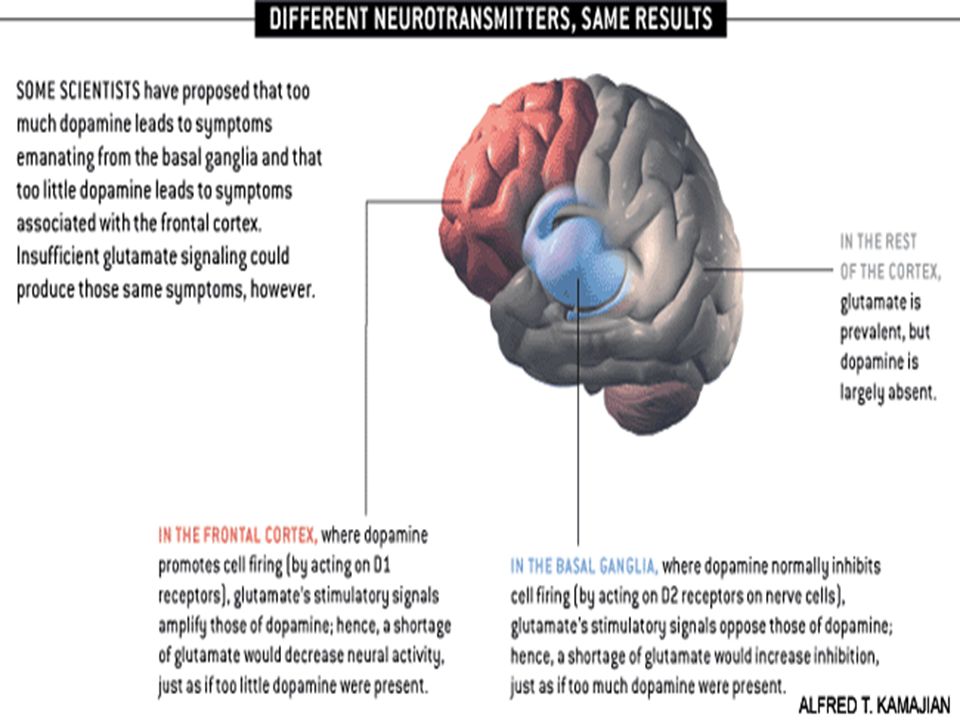
2- Neurobiology * Certain areas of the brain are involved in the pathophysiology of schizophrenia: the limbic system, the frontal cortex, cerebellum, and the basal ganglia. a- Dopamine Hypothesis; Too much dopaminergic activity ( whether it is ↑ release of dopamine, ↑ dopamine receptors, hypersensitivity of dopamine receptors to dopamine, or combinations is not known ). b- Other Neurotransmitters; Serotonin, Norepinephrine, GABA, Glutamate & Neuropeptides
. b- Other Neurotransmitters; Serotonin, Norepinephrine, GABA, Glutamate & Neuropeptides.")
10
c- Neuropathology; Neuropathological and neurochemical abnormalities have been reported in the brain particularly in the limbic system, basal ganglia and cerebellum. Either in structures or connections.

13
d- Psychoneuroimmunology; ↓ T-cell interlukeukin-2 & lymphocytes, abnormal cellular and humoral reactivity to neurons and presence of antibrain antibodies. These changes are due to neurotoxic virus ? or endogenous autoimmune disorder ? e- Psychoneuroendocrinology; Abnormal dexamethasone-suppression test ↓ LH/FSH A blunted release of prolactin and growth hormone on stimulation.

14
3- Genetic Factors - A wide range of genetic studies strongly suggest a genetic component to the inheritance of schizophrenia that outweights the environmental influence. - These include: family studies, twin studies and chromosomal studies.

16
Schizophrenia: genes plus stressors Schizophrenia is mostly caused by various possible combinations of many different genes (which are involved in neurodevelopment, neuronal connectivity and synaptogenesis) plus stressors from the environment conspiring to cause abnormal neurodevelopment. There is also abnormal neurotransmission at glutamate synapses, possibly involving hypofunctional NMDA receptors. Stephen M The Genetics Of Schizophrenia Converge,Upon,The NMDA Glutamate Receptor, CNS Spectr. 2007

17
4- Psychosocial Factors; In family dynamics studies, no well-controlled evidence indicates specific family pattern plays a causative role in the development of schizophrenia. High Expressed Emotion family : increase risk of relapse.

18
Weight of different RF: Family history comes first PLOS Medicine

19
Diagnosis # DSM-5 Diagnostic Criteria for Schizophrenia: A- ≥ two characteristic symptoms for one month, at least one of them is (1),(2) or (3) 1- Delusions 2- Hallucinations 3- Disorganized speech (frequent derailment or incoherence) 4- Grossly disorganized or catatonic behavior 5- Negative symptoms ( diminished emotional expression or lack of drive (avolition))
,(2) or (3) 1- Delusions 2- Hallucinations 3- Disorganized speech (frequent derailment or incoherence) 4- Grossly disorganized or catatonic behavior 5- Negative symptoms ( diminished emotional expression or lack of drive (avolition))")
20
B- Social, Occupation or self-care dysfunction C- Duration of at least 6 months of disturbance (include at least one month of active symptoms that meet Criterion A; in addition of periods of prodromal and residual symptoms). D- Schizoaffective & mood disorder exclusion E- The disturbance is not due to Substance or another medical condition. F- If there is history of autism spectrum disorder or a communication disorder of childhood onset, schizophrenia diagnosis is made only if delusion or hallucinations plus other criteria are present.

21
Clinical Features No single clinical sign or symptom is pathognomonic for schizophrenia Patient's history & mental status examination are essential for diagnosis. Premorbid history includes schizoid or schizotypal personalities, few friends & exclusion of social activities. Prodromal features include obsessive compulsive behaviors, attenuated positive psychotic features.

22
- Picture of schizophrenia includes positive and negative symptoms. - Positive symptoms like: delusions & hallucinations. - Negative symptoms like: affective flattening or blunting, poverty of speech, poor grooming, lack of motivation, and social withdrawal.

23
Cognitive deficits in schizophrenia

24
Mental status examination - Appearance & behavior ( variable presentations) - Mood, feelings & affect ( reduced emotional responsiveness, inappropriate emotion) - Perceptual disturbances ( hallucinations, illusions ) - Thought: Thought content ( delusions) Form of thought ( looseness of association) Thought process ( thought blocking, poverty of thought content, poor abstraction, perseveration ) - Impulsiveness, violence, suicide & homicide - Cognitive functioning - Poor insight and judgment
 - Mood, feelings & affect ( reduced emotional responsiveness, inappropriate emotion) - Perceptual disturbances ( hallucinations, illusions ) - Thought: Thought content ( delusions) Form of thought ( looseness of association) Thought process ( thought blocking, poverty of thought content, poor abstraction, perseveration ) - Impulsiveness, violence, suicide & homicide - Cognitive functioning - Poor insight and judgment")
25
Course Acute exacerbation with increased residual impairment Full recovery: very rare Longitudinal course: downhill

27
Prognosis Good P.FPoor P.F 1.Late age of onset 2.Acute onset 3.Obvious precipitating factors 4.Presence of mood component 5.Good response to Tx 6.Good supportive system 1.Young age of onset 2.Insidious onset 3.Lack of P.F. 4.Multiple relapses 5.Low IQ 6.Poor premorbid personality 7.Negative symptom 8.Positive family history

28
Differential Diagnosis Secondary psychiatric disorders: -Substance-induced disorders -Psychotic disorders due to another medical disorder : Epilepsy ( complex partial) CNS diseases Trauma Others Primary Psychiatric disorders: Schizophreniform disorder Brief psychotic disorder Delusional disorder Schizoaffective disorder Mood disorders Personality disorders ( schizoid, schizotypal & borderline personality) Factitious disorder Malingering
 CNS diseases Trauma Others Primary Psychiatric disorders: Schizophreniform disorder Brief psychotic disorder Delusional disorder Schizoaffective disorder Mood disorders Personality disorders ( schizoid, schizotypal & borderline personality) Factitious disorder Malingering")
29
Criteria of other Psychotic Disorders Psychotic Disorders due to another medical condition Substance-induced psychotic disorder Schizophreniform disorder ; 1-6 month of disturbance Brief psychotic disorder: <1month of disturbance Delusional disorder(delusion only >1m)
")
30
An uninterrupted period of illness that includes either a major depressive disorder or a manic episode along with at least two active symptoms of schizophrenia (hallucinations, delusions, disorganized speech, severely disorganized or catatonic behaviors, negative symptoms like decreased emotional expression or movement) Delusions or hallucinations occur at least two weeks without major depressive or manic symptoms at some time during the illness. The major mood symptoms occur for most of the duration of the illness. The illness is not the result of a medical condition or the effects of alcohol, other drugs of abuse, or a medication. DSM-5 Diagnostic Criteria for Schizoaffective disorder

31
Case Development 1 Schi smokes tobacco frequently to calm himself. During his early adolescence he used to smokes Hash heavily plus occasional use of amphetamine. He stopped both Hash and Amphetamine use 5 years ago. His father disclosed to his psychiatrist that that Schi used to have brief fixed persecutory (paranoid) ideas towards his brothers associated with the use of amphetamine.
 ideas towards his brothers associated with the use of amphetamine..")
32
Analyze the symptoms & signs, both presented and expected in this case including mood, thoughts, cognition, perception and physical aspects. Discuss possible etiological reasons Discuss differential diagnosis Discuss management especially of amphetamine induced psychotic disorder.

33
Potentially severe, usually temporary. Context of substances of abuse, medications, or toxins of any of the 10 classes of substances. Clinically significant presentation of a secondary psychiatric disorder. Evidence in history, PE, MSE and labs of: Develop during or within 1 month of use Capable of producing mental disorder seen Not an independent mental disorder Preceded onset of use Persists for substantial time after use (more that a month after off of substance use) Substance-Induced psychiatric Disorder
 Substance-Induced psychiatric Disorder.")
34
Case Development 2 Pre-morbidly, Schi used to have chronic sense of insecurity and suspiciousness towards others with few and superficial social relations and having difficulties to initiate new relationships. Discuss cluster A personality traits Discuss commonly used defense mechanisms by such patients.

35
Personality Traits Attitude to self (self-appraisal, performance, satisfaction, past achievements and failures, future..) Moral and religious attitudes and standards. Prevailing mood and emotions. Reaction to stress (ability to tolerate frustration and disappointments, pattern of coping strategies). Personal interests, habits, hobbies and leisure activities. Interpersonal relationships.
. Personal interests, habits, hobbies and leisure activities. Interpersonal relationships..")
36
Characteristics of personality traits 1. Influenced by Genetics 2. Influenced by Environment 3. Determine how an individuals cope with stress 4. Quantitative, spectrum. 5. Overlap between personality traits/disorders is common. Note: No body is complete Every body has some minor abnormal traits ( but not personality disorders)
.")
37
DSM Criteria of personality disorder 1. Pattern of behavior/inner experience that deviates from the person’s culture and is manifested in two or more of the following ways: Cognition Affect Personal relations Impulse control 2. The pattern: Is pervasive and inflexible in a broad range of situations Is stable and has an onset no later than adolescence or early adulthood Leads to significant distress in functioning Is not accounted for by another mental/medical illness or by use of a substance

38
DS M-5 Classification of Personality Disorders: ClusterDescriptionDisorders Aperceived as being eccentric and “weird.” 1-Paranoid 2-Schizoid 3- Schizotypal. Boften emotional, impulsive, and dramatic 1. Histrionic 2.Narcissistic 3. Borderline 4.Antisocial Cappear anxious and fearful 1. Avoidant 2.Dependant 3.Obsessive Comp.

39
Cluster A Paranoid personality Schizoid personality Schizotypal personality

40
Cluster A – Paranoid Personality Two main features: - suspiciousness - sensitivity to criticism Caution=(beyond normal) Constant look for attempts by others to harm them argumentative Combative attitude Looking for other people’s mistakes Readily feel humiliated
 Constant look for attempts by others to harm them argumentative Combative attitude Looking for other people’s mistakes Readily feel humiliated")
41
Cluster A – Paranoid Personality Interpersonal Relationship = Disturbed “Touchy people” “Difficult people” Projection = is the defence mechanism Basic defect= weakness they compensate by strong feeling of self importance.

42
Cluster A – Paranoid Personality How to deal with them: (Rx) No effective Rx Avoid close contact too quickly Dealing with stress Supportive psychotherapy Short courses of psychotropic drugs during crises Rx of concurrent mental illness
 No effective Rx Avoid close contact too quickly Dealing with stress Supportive psychotherapy Short courses of psychotropic drugs during crises Rx of concurrent mental illness")
43
Cluster A – Schizoid Personality The main problems are: The emotions. Cold or lack of warmth Isolation Self sufficient Relationship= neither desired nor enjoyable Often remain single Not sensitive They don't need or want Rx

44
Cluster A – Schizotypal Personality Debatable issue i.e. is it actually a form of schizophrenia? Odd ideas Inappropriate affect Unable to make close relationship Unusual perceptual experiences Suspiciousness Unable to make close relationship

45
Case Development 3 He sees a psychiatrist for 15 minutes every two months but sometimes misses his appointment. His parents support him financially and he has a social worker whom he sees often. Schi was treated with Haloperidol which gave him muscle cramps especially in his neck, he was then treated with Olanzapine and gained 10 kg and developed Diabetes Mellitus. During his illness course, the patient’s family became less supportive to him & he became less compliant on his treatments. His psychiatrist would like to switch him to long acting injectable antipsychotic treatment but Schi is afraid of injections and isn't sure that he needs medication.

46
Considering this case: Discuss management of schizophrenia. Discuss the types of antipsychotics, indication, side effects, etc Discuss the role of psychotherapy, the role of family and other social approaches Discuss in detail Extrapyramidal side effect and Neuroleptic malignant syndrome(NMS)
.")
47
Treatment What are the indications for hospitalization? Diagnostic purpose Patient & other's safety Initiating or stabilizing medications Establishing an effective association between patient & community supportive systems

48
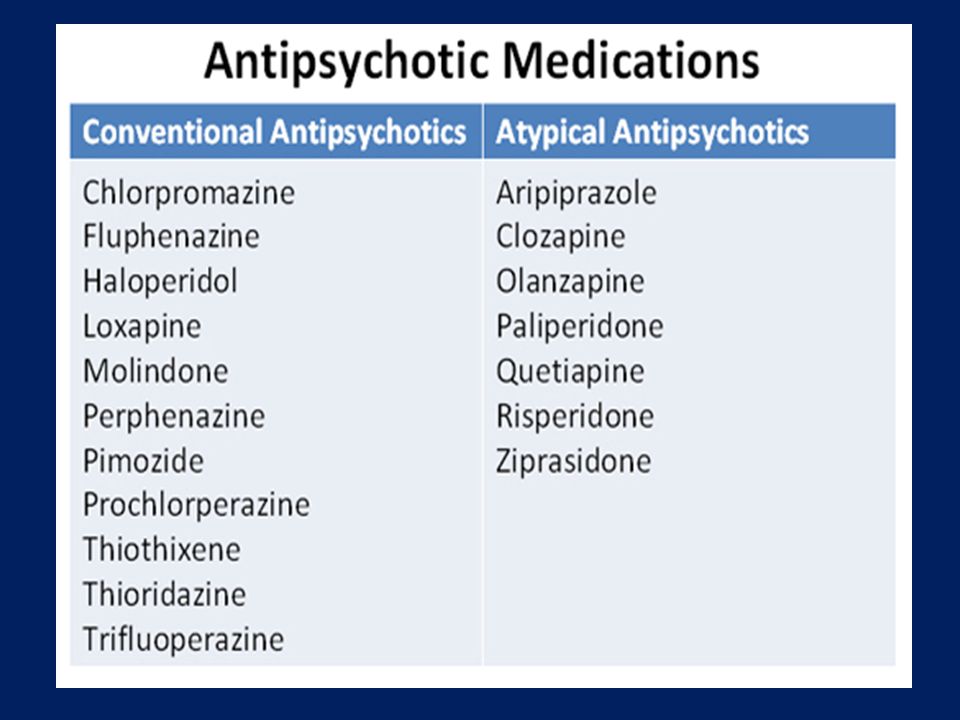
Biological therapies Antipsychotic medications are the mainstay of the treatment of schizophrenia. Generally, they are remarkably safe. Two major classes: -Dopamine receptor antagonists ( haloperidol, chlorpromazine ) -Serotonin-dopamine receptor antagonists ( Risperidone, clozapine, olanzapine ). Depot forms of antipsychotics eg. Risperidone Consta is indicated for poorly compliant patients. - Electroconvulsive therapy (ECT) for catatonic or poorly responding patients to medications
 -Serotonin-dopamine receptor antagonists ( Risperidone, clozapine, olanzapine ). Depot forms of antipsychotics eg. Risperidone Consta is indicated for poorly compliant patients. - Electroconvulsive therapy (ECT) for catatonic or poorly responding patients to medications.")
50
Antipsychotics and dopamine system

51
Pharmacolog ical Treatment Algorithm Adapted from the Maudsley prescribing Guidelines (Taylor et al, 2005)
")
52
Common side effects of antipsychotic medication (Taylor et al, 2005)
")
53
Side effects of antipsychotics High Potency typical antipsychotics: Neurological side effects Low Potency typical and atypical antipsychotics: many other side effects

54
Side effects of antipsychotics

56
Side effects of atypical antipsychotics

57
Metabolic effects of atypical antipsychotics

58
Narcoleptic malignant syndrome Psychosomatic medicine,, J Amos

59
Psychosocial therapies Social skills training Family oriented therapies Group therapy Individual psychotherapy Assertive community treatment Vocational therapy

60
Aggression assessment and management

61
Case Development 4 9 months later, patient was brought to ER in a state of severe verbal and physical aggression. Moreover, His father reported he was destructive to properties at home. How to assess Aggressive Patient? How to manage Aggressive Patient?

62
Assessment of Agitated and Aggressive Patients What is agitation: Tension state in which anxiety is manifested in psychomotor area with hyperactivity. Seen in depression, schizophrenia & mania. What is aggression: Hostile or angry feelings, thoughts or actions directed towards an object or person. Seen in impulsive disorders, impulse control disorders & mania.

63
Patients with mental disorders do not commit most violent crimes The probability of violent behavior among patients with mental disorders is greater than that for the general population especially in low-crime countries. A Sweden study (1)from found that patients with severe mental illness commit 1 in 20 violent crimes). Young, male, Substance abuser esp. Alcohol has the highest relative risk for violence. Using case registries in Australia (N = 4156), the odds ratio for violent offenses was 2.4 for male individuals with schizophrenia with no substance abuse problems and 18.8 for schizophrenia complicated by substance abuse(1). ( 1) Fazel S, Grann M. 2006 (2)Wallace C,1993 Epidemiology
from found that patients with severe mental illness commit 1 in 20 violent crimes). Young, male, Substance abuser esp. Alcohol has the highest relative risk for violence. Using case registries in Australia (N = 4156), the odds ratio for violent offenses was 2.4 for male individuals with schizophrenia with no substance abuse problems and 18.8 for schizophrenia complicated by substance abuse(1). ( 1) Fazel S, Grann M (2)Wallace C,1993 Epidemiology.")
64
A) Male B) young C) previous aggression D) Dx : 1) schizophrenia 2) Major depression 3) Bipolar disorder 4) substance abuse 5) antisocial or borderline personality 6) Dementia 7) delirium 8) traumatic brain injury 9) Epilepsy Risk factors of aggression among mentaly ill patients
 Male B) young C) previous aggression D) Dx : 1) schizophrenia 2) Major depression 3) Bipolar disorder 4) substance abuse 5) antisocial or borderline personality 6) Dementia 7) delirium 8) traumatic brain injury 9) Epilepsy Risk factors of aggression among mentaly ill patients")
65
E) Symptoms of : confusion intoxication akathesia fearfulness agitation paranoid delusion command hallucination ****** specific IN-PATIENT medical setting : Post-operative delirium Pain First 48 hours ( withdrawal state) Risk factors of aggression among mentaly ill patients
 Symptoms of : confusion intoxication akathesia fearfulness agitation paranoid delusion command hallucination ****** specific IN-PATIENT medical setting : Post-operative delirium Pain First 48 hours ( withdrawal state) Risk factors of aggression among mentaly ill patients")
66
Patients factors intoxication Psychiatric disorders including personality Involuntary negative perception of hospital staffs possession of weapon at presentation staff factors Impoliteness insensitivity inadequate training Environmental factors high noise level overcrowding uncomfortable waiting rooms System factors pts volume Increase waiting time decrease staff decreased training in management of aggressive patients Risk factors of aggression in Emergency setting

67
impulsive Relatively unplanned Decrease CSF 5HIAA premeditated Deliberate Predatory Pathological Increase DA,NE Mechanism of aggression

68
History : setting-sequences-outcome MSE: repeated assessment of dangerousness, suicide & insight. P/E : V/S, exclude injury Evaluation of aggression

69
Clinical progression of aggression in general hospital

70
Investigations: blood tests (anemia,infection, electrolytes, biochemistry) Toxicology EEG CT scan or MRI FORMULATION Evaluation of aggression
 Toxicology EEG CT scan or MRI FORMULATION Evaluation of aggression")
71
I. Self-protection Know as much as possible about the patients before meeting them. Leave physical restraint procedures to those who are trained. Be alert to risks of impending violence. Attend to the safety of the physical surroundings (e.g., door access, room objects). Have others present during the assessment if needed. Have others in the vicinity. Attend to developing an alliance with the patient (e.g., do not confront or threaten patients with paranoid psychoses). II. Prevent harm Prevent self-injury and suicide. Use whatever methods are necessary to prevent patients from hurting themselves during the evaluation. General Strategy in Evaluating the Patient
. Have others present during the assessment if needed. Have others in the vicinity. Attend to developing an alliance with the patient (e.g., do not confront or threaten patients with paranoid psychoses). II. Prevent harm Prevent self-injury and suicide. Use whatever methods are necessary to prevent patients from hurting themselves during the evaluation. General Strategy in Evaluating the Patient.")
72
Prevent violence toward others. During the evaluation, briefly assess the patient for the risk of violence. If the risk is deemed significant, consider the following options: 1) Inform the patient that violence is not acceptable. 2) Approach the patient in a nonthreatening manner. 3) Reassure, calm, or assist the patient's reality testing. 4) Offer medication. 5) Inform the patient that restraint or seclusion will be used if necessary. 6) Have teams ready to restrain the patient. 7) When patients are restrained, always closely observe them, and frequently check their vital signs. Isolate restrained patients from surrounding agitating stimuli. Immediately plan a further approach e.g. medication, reassurance, medical evaluation. III. Rule out secondary psychiatric disorders. IV. Rule out impending psychosis. General Strategy in Evaluating the Patient
 Inform the patient that violence is not acceptable. 2) Approach the patient in a nonthreatening manner. 3) Reassure, calm, or assist the patient s reality testing. 4) Offer medication. 5) Inform the patient that restraint or seclusion will be used if necessary. 6) Have teams ready to restrain the patient. 7) When patients are restrained, always closely observe them, and frequently check their vital signs. Isolate restrained patients from surrounding agitating stimuli. Immediately plan a further approach e.g. medication, reassurance, medical evaluation. III. Rule out secondary psychiatric disorders. IV. Rule out impending psychosis. General Strategy in Evaluating the Patient.")
73
Assess the risk of violence 1) Consider violent ideation, wish, intention, plan, availability of means, implementation of plan, wish for help. 2) Consider demographics e.g.sex (male), age (15 to 24), socioeconomic status (low), social supports (few). 3) Consider past history: violence, nonviolent antisocial acts, impulse dyscontrol (e.g., gambling, substance abuse, suicide or self-injury, psychosis). 4) Consider overt stressors (e.g., marital conflict, real or symbolic loss). Assessing and Predicting Violent Behavior
 Consider demographics e.g.sex (male), age (15 to 24), socioeconomic status (low), social supports (few). 3) Consider past history: violence, nonviolent antisocial acts, impulse dyscontrol (e.g., gambling, substance abuse, suicide or self-injury, psychosis). 4) Consider overt stressors (e.g., marital conflict, real or symbolic loss). Assessing and Predicting Violent Behavior.")
74
Differential diagnoses of violent behavior

75
Assess the environment for potential dangers (e.g., objects that can be thrown or used as a weapon). Assess the physical demeanor of the patient (e.g., many patients make a fist before punching or kicking). Know where the patient is at all times (e.g., do not turn your back to the patient; do not leave the patient alone and therefore unobserved). Take verbal threats seriously. Remain several feet away to avoid crowding the patient. Nonpharmacological management of aggressive behavior
. Know where the patient is at all times (e.g., do not turn your back to the patient; do not leave the patient alone and therefore unobserved). Take verbal threats seriously. Remain several feet away to avoid crowding the patient. Nonpharmacological management of aggressive behavior.")
76
Clear the area of other patients. Call for additional help (a "show of force" or a "show of concern"); this is not a time for heroics. Remain calm, maintain a confident and competent demeanor, and attempt to deescalate by engaging the patient in conversation. Avoid arguments between staff members in front of the patient. If restraints are necessary, have at least 4 people available. Nonpharmacological management of aggressive behavior
; this is not a time for heroics. Remain calm, maintain a confident and competent demeanor, and attempt to deescalate by engaging the patient in conversation. Avoid arguments between staff members in front of the patient. If restraints are necessary, have at least 4 people available. Nonpharmacological management of aggressive behavior.")
77
Multimodal ( behavioral, psycho educational & family) Behavioral : token economy aggression replacement strategies Decelarative techniques psycho educational : Pts & family must learn to identify warning behaviors e.g. cursing, threatening and then apply alternative pleasurable behaviors Family : increase coping & ability to manage aggressive behaviors Non pharmacological Tx of chronic aggression

78
BDZ Lorazepam P.O 0.5-2 mg every 1-6 hours IM or I.V If I.V route push slowly < 2mg/ min Antipsychotics Haloperidol 1-5 mg Give 1-5 mg each 30 min until aggression is controlled P.O,IM or I.V others seclusion restraint Tx of acute agitated behavior

79
Tx of chronic aggression

Similar presentations