Download presentation
Presentation is loading. Please wait.

2
Renal Stone Hossein Hamidi MD. Isfahan university of Medical Sciences

3
Epidemiology 12% of men and 5% of women develop symptomatic stone by the age of 70. Rate of nephrolithiasis increases with : Age Men White

4
Etiology : Calcium stones 80% ( Ca ox > Ca ph ) Uric acid Struvite (Mg,Ammonium-Phosphate ) Cystine One patient may have more than one type (eg : Ca & uric acid )
 Uric acid Struvite (Mg,Ammonium-Phosphate ) Cystine One patient may have more than one type (eg : Ca & uric acid )")
5
An oxalate stone

6
A calcium phosphate stone

7
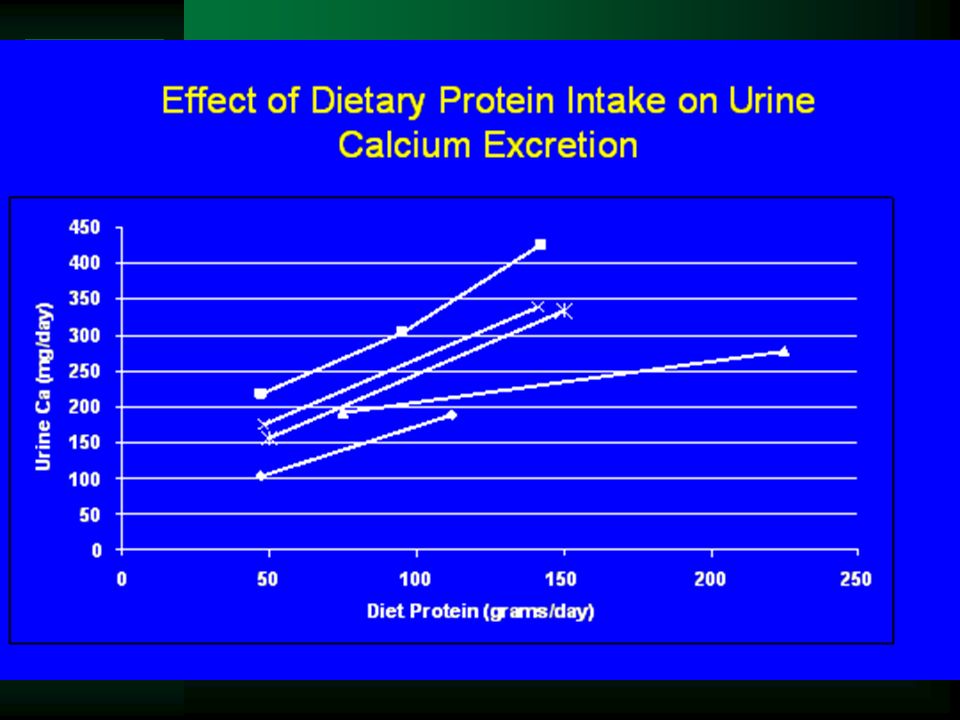
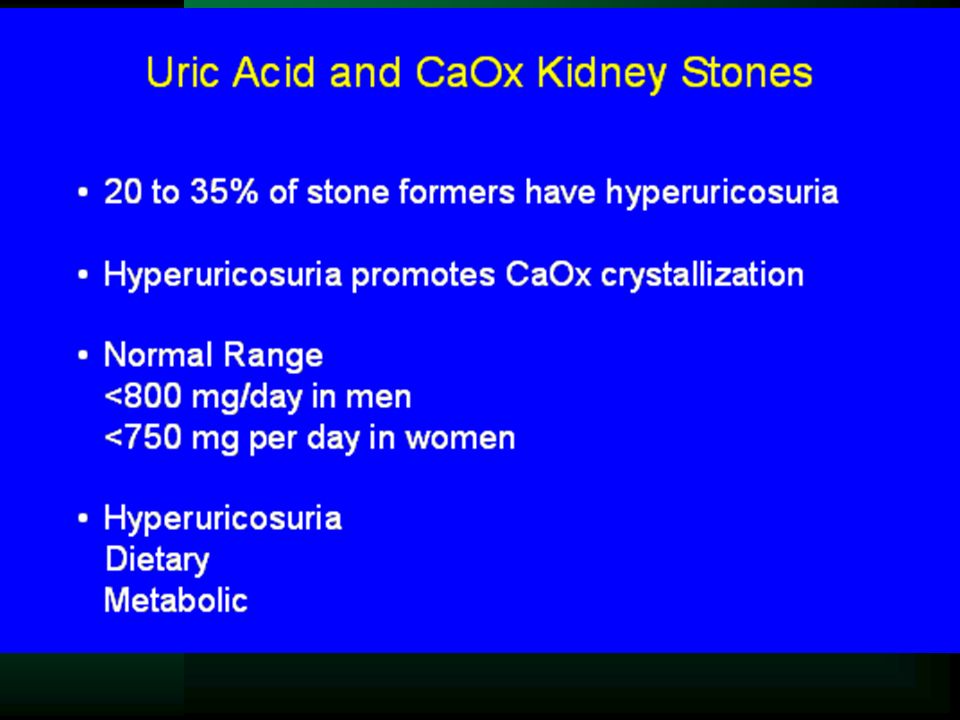
Risk factors : 1. Hypercalciuria 2. Hyperuricosuria ( uric acid- ca ox stones ) 3. Hypocitraturia 4. High protein intake ( animal > vegetable ) 5. Low water intake 6. High salt diet ( prior stone ) 7. Prior calcium nephrolithiasis
 5. Low water intake 6. High salt diet ( prior stone ) 7. Prior calcium nephrolithiasis.")
8
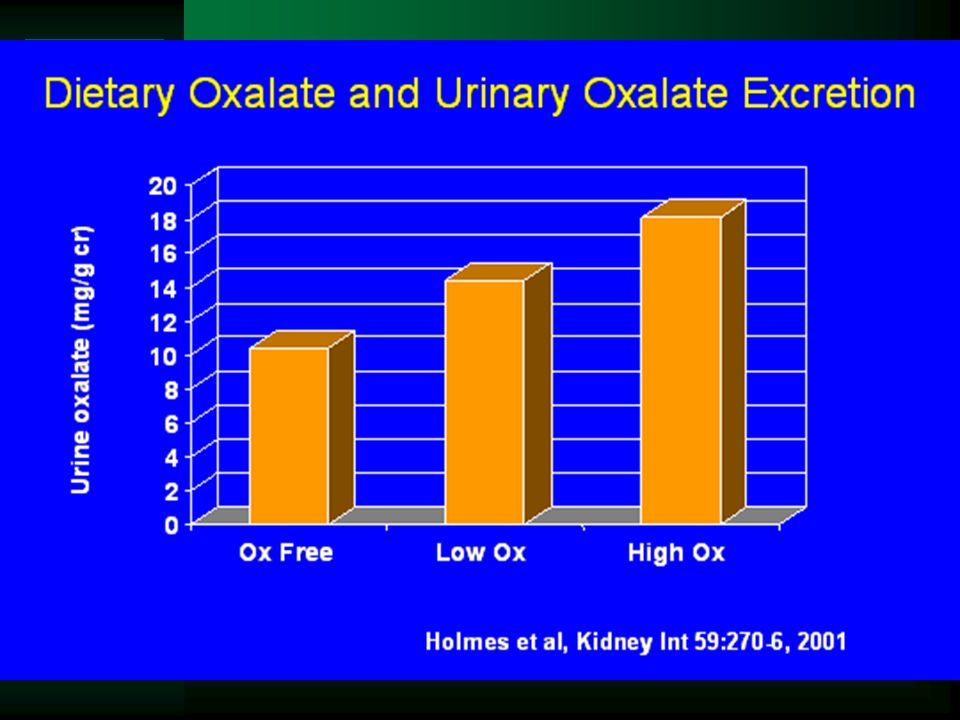
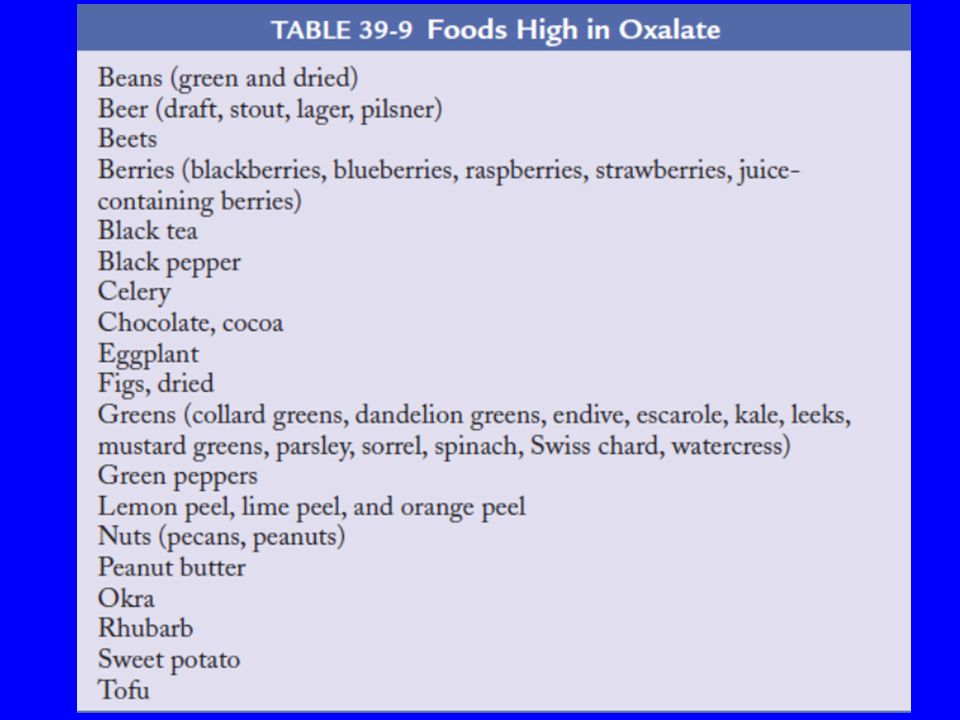
Risk factors : cont … 8. Family history 9. Enteric oxalate absorption 10. Urinary tract infection (spinal cord injury) 11. Medications : (indinavir, sulfadiazine, trimterene) 12. Hypertension (hypercalciuria ) 13. Marathon runners 14. Type of fluid taken
 11. Medications : (indinavir, sulfadiazine, trimterene) 12. Hypertension (hypercalciuria ) 13. Marathon runners 14. Type of fluid taken.")
9
Risk factors : cont … 15. Gout 16. Chronic diarrheal state ( acidosis, urine volume, acid urine ) 17. Cystinuria 18. Vitamine intake ( C or D ) controversial. 19. Primary hyperparathyroidism 20. Medullary sponge kidney 21. Type one distal RTA
 17. Cystinuria 18. Vitamine intake ( C or D ) controversial. 19. Primary hyperparathyroidism 20. Medullary sponge kidney 21. Type one distal RTA.")
10
Pathophysiology

11
There are two major factors that promote uric acid precipitation: a high concentration of uric acid; and an acid urine pH which drives the reaction toward uric acid formation, H(+) + Urate(-) Uric acid Relatively soluble insoluble
 + Urate(-) Uric acid Relatively soluble insoluble")
12
at a urine pH of 7.0 (a setting in which 95 percent of uric acid is present as the more soluble urate anion) at a urine pH of 5.0 (a setting in which most of the uric acid is the insoluble intact acid)
 at a urine pH of 5.0 (a setting in which most of the uric acid is the insoluble intact acid)")
13
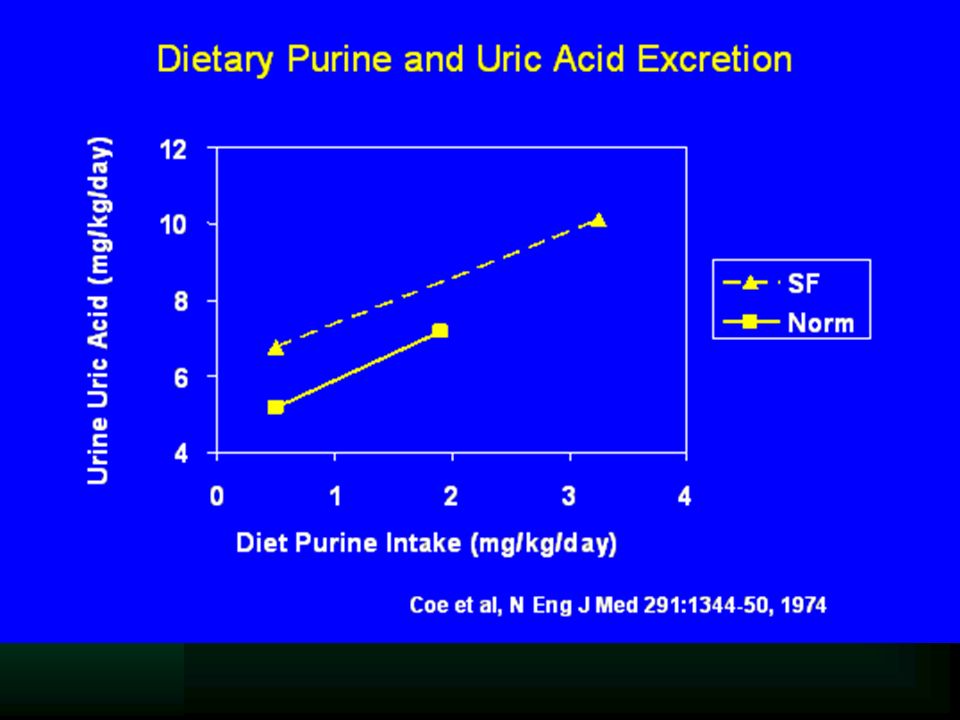
the incidence of stone formation varies with the rate of uric acid excretion, ranging from 10 to 20 percent when urinary uric acid excretion is normal (upper limit of normal equals 800 mg [4.8 mmol] in men and 750 mg [4.5 mmol] in women) to as high as 40 to 50 percent when uric acid excretion exceeds 1000 mg/day (6 mmol/day).
![ the incidence of stone formation varies with the rate of uric acid excretion, ranging from 10 to 20 percent when urinary uric acid excretion is normal (upper limit of normal equals 800 mg [4.8 mmol] in men and 750 mg [4.5 mmol] in women) to as high as 40 to 50 percent when uric acid excretion exceeds 1000 mg/day (6 mmol/day).](http://images.slideplayer.com/24/7016862/slides/slide_13.jpg " the incidence of stone formation varies with the rate of uric acid excretion, ranging from 10 to 20 percent when urinary uric acid excretion is normal (upper limit of normal equals 800 mg [4.8 mmol] in men and 750 mg [4.5 mmol] in women) to as high as 40 to 50 percent when uric acid excretion exceeds 1000 mg/day (6 mmol/day).")
15
multivalent metallic cations, such as magnesium. small organic anions, such as citrate. small inorganic anions, such as pyrophosphate. macromolecules, such as osteopontin and Tamm Horsfall protein. There are at least four types of inhibitors in urine:

16
WWW.HDCN.COM/SYMP/02ASN/ASP2/ASP2.HTM
18
Histologic images showing sites of Randall's plaque and its progression

19
1. Ca Oxalate crystals attached to renal papilla

26
Clinical manifestations : Asymptomatic Passing of gravel (uric acid ) or stone Pain Mild to severe Wax & wane ( paroxysm of severe pain lasts 20 – 60 min). Renal pelvic or upper ureter (flank pain or tenderness) lower ureter (ipsilateral testicle or labia )
 lower ureter (ipsilateral testicle or labia ).")
28
Clinical manifestations : cont … Hematuria ( gross or microscopic ) in the majority of patients, the single most discriminate predictor of kid. stone in unilateral flank pain. The absence of hematuria in acute flank pain does not exclude nephrolithiasis Nausea,vomiting, dysuria, urgency, when the stone is entering the bladder or urethra.

29
Diagnosis: Clinical manifestations Family hx Urinalysis – urine culture Stone analysis KUB IVP US CT SCAN ( choice )
")
30
Diagnosis: cont … Urinalysis : PH >7.5 infection PH < 5.5 uric acid sediment: uric acid crystals, acid urine amorphous urate Struvite orCa ph crystals alkaline urine Ca ox crystals PH. Independent cystine crystal :hexagonal, struvite: mg.am.ph amm, ur. PH + UTI (proteus or klebsiella) = only struvite stone
 = only struvite stone.")
31
Uric acid crystals

32
Calcium oxalate crystals

33
Struvite crystal in urine sediment (Mg Ammonium Phosphate, coffin lid) only alkaline urine, pH>7
 only alkaline urine, pH>7")
34
Ca phosphate crystals

35
Cystine crystals

36
Indinavir

37
Diagnosis: cont … KUB : * Detect : radiopaque stones ( Ca, struvite, cystine stones) * Will miss : uric acid stone small stone stone overlying bony structures * Will not detect : obstruction
 * Will miss : uric acid stone small stone stone overlying bony structures * Will not detect : obstruction")
42
IVP : high sensitivity and specificity, procedure of choice but reaction, replaced by non- contrast CT – Scan Non – contrast helical CT scan : Detect both stone and UTO, the gold standard for radiologic diagnosis of stones. Radiolucent stones missed on KUB, usually detected by CT scan. Detect second sign of obs. :1- ureter dilatation 2- collecti- ng system dilatation 3- perinephric stranding. Diagnosis: cont …

45
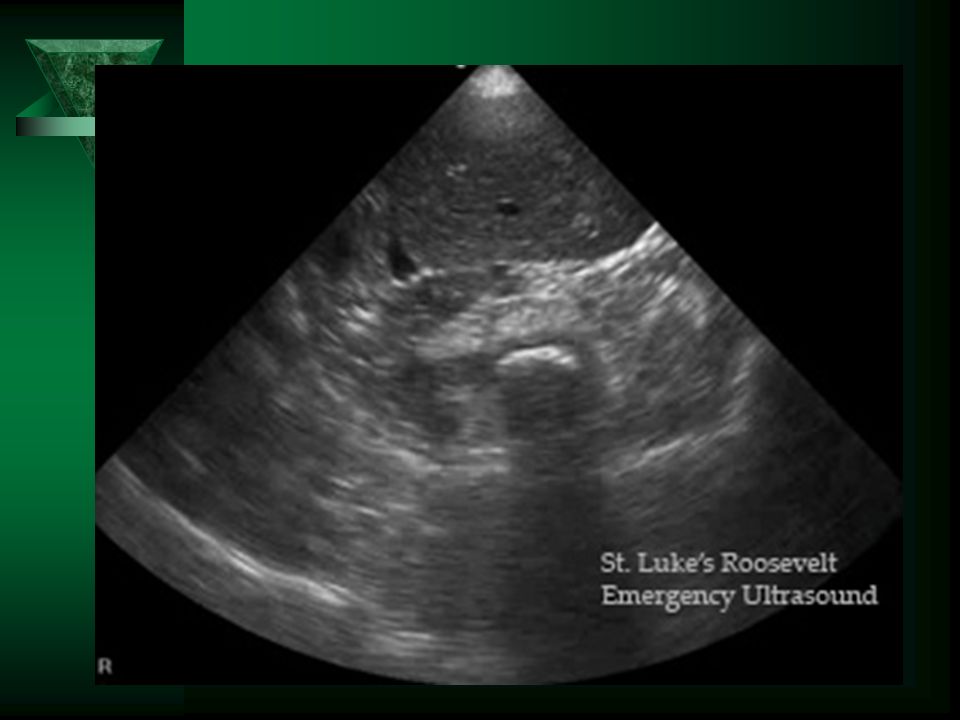
U.S. : 1- Choice for pregnant women. 2-Childbearing age. 3- Very sensitive for UTO. 4-Detect radiolucent stones. 5-May miss small stones and ureteral stones.

47
Diagnosis: cont … Recommendations : 1-Dx of nephrolithiasis : actual onset of atraumatic flank pain without abdominal tenderness and with hematuria. 2- non contrast helical CT scan due to higher sensitivity and specificity than IVP and US, suggest the initial diagnostic study of choice in most cases, and is faster than IVP and slightly more expensive ($ 600 vs $ 400 ). If helical CT is not available, IVP or US are appropriate.
. If helical CT is not available, IVP or US are appropriate..")
48
Evaluation of a pt. with established nephrolithiasis Ca stones : risk factors of ca ox same as ca ph, except : 1-hyperoxaluria and hyperuricosuria for ca ox. 2-urine PH > 5.3, type 1 RTA for ca ph. Calcium stone formation is most often idiopathic but in other disorders : Primary hyperparathyroidism Medullary sponge kidney Distal RTA

49
Evaluation of a pt. with established nephrolithiasis con... Uric acid stones : occurs in: 1- persistent acid urine 2- overproduction of uric acid in gout 3- chronic diarrheal states Struvite stones : only in chronic UTI due to urease producing organisms such as proteus and klebsiella. patients have Mg. Amm. Ph. crystal in urine. Stone may grow over a period of weeks or months, if not adequately treated develop a staghorn calculus.

50
Evaluation of a pt. with established nephrolithiasis cont... Cystine stones : in pts. With cystinuria due to insolubility of cystine in the urine. Diag. :1- F.Hx. 2- hexagonal crystals on urinalysis in 25% of pts. 3- measurement of urinary cystine excretion. Risk factors : fluid intake, animal protein, (hypercalciuria, hyperuricosuria, hypocitraturia), salt diet, Ca intake, foods with oxalate?, Vitamin D.
, salt diet, Ca intake, foods with oxalate , Vitamin D..")
51
Evaluation of a pt. with established nephrolithiasis cont... Medications : Indinavir, Sulfadiazine, Triamterene. Evaluation : 1- complete: * multiple stones at first presentation * active stone disease ( recurrent stone,enlargement of old stone, passage of gravels ) 2- limited :after first stone 3- targeted :first stone if : F Hx +ve, male, middle age,chronic diarrheal state and /or malabsorption pathologic skeletal Fx.,osteoporosis, UTO and/or gout, stone composed of : cystine, uric acid, Ca ph, or struvite
 2- limited :after first stone 3- targeted :first stone if : F Hx +ve, male, middle age,chronic diarrheal state and /or malabsorption pathologic skeletal Fx.,osteoporosis, UTO and/or gout, stone composed of : cystine, uric acid, Ca ph, or struvite.")
52
Evaluation of a pt. with established nephrolithiasis cont... Radiologic evaluation IVP : site & degree of obstruction US : presence of ureteral dilatation without stone : recent passage of stone. Mg Am Ph & cystine stones are opaque but less dense than Ca stones. Ca ph stone in the presence of nephrocalcinosis : RTA Bilateral calcification at C M J : medullary sponge kidney ( Ca ox or Ca ph stone ) IVP the only method of established diagnosis of MSK. Staghorn calculi favors struvite stones.
 IVP the only method of established diagnosis of MSK. Staghorn calculi favors struvite stones..")
53
Evaluation of a pt. with established nephrolithiasis cont... Radiologic evaluation MSK is 12% -20% of Ca stone formers MSK is 20% - 30% of women and those < the age of 20. MSK is associated with Calciuria, uricosuria, citraturia, urine volume. Diagnosis and medical treatment same as other stones. Radiologic monitoring of stone : usually with US or KUB. initially at one year, if – ve every two or four yrs.

54
Metabolic evaluation Blood : uric acid, Ca, bicarbonate. low bicarb : type 1 RTA. Ca measured on 2 or 3 occasions,if high NL (10.2- 11), or urine Ca is high : intact PTH should measured, since Primary HP is often associated with inttermi. or mildly elevated plasma Ca. PHP suspected in women, since PHP is more common in women, whereas 80% of formers of idiopathic stones are men.
, or urine Ca is high : intact PTH should measured, since Primary HP is often associated with inttermi. or mildly elevated plasma Ca. PHP suspected in women, since PHP is more common in women, whereas 80% of formers of idiopathic stones are men..")
55
Metabolic evaluation Twenty four hours urine collection: urine volume, PH,Ca, uric acid, citrate, oxalate, Na, Creatinine calculated. Two or three separate collections to obtain all of these informations. Uric acid in alkaline or plain solution, Ca and Ox. in HCl or nitric acid solution,Citrate in acidified solution ( needs 2or 3 sample and two or three 24 hr. urine collctions). Timing of collection : Pt. on his or her normal diet ( not in hospital ). Two or three months after stone event or any interventionas ( ex : ESWL ).
. Timing of collection : Pt. on his or her normal diet ( not in hospital ). Two or three months after stone event or any interventionas ( ex : ESWL )..")
56
Management of renal & ureteral stones Surgical Medical Surgical : 10% -20% require surgical management. Stones < 5 mm pass spontaneously. Stones > 8-10 mm pass unlikely.

57
Management of renal & ureteral stones Indication of stone removal : Pain Obstruction Infected struvite stone Large stone : > 2cm or staghorn stone Cystine stone

58
Management of renal & ureteral stones Three surgical techniques : Percutaneous nephrolithotomy Rigid & flexible ureterorenoscopy Shock wave lithotripsy proximal & renal stones SWL middle & distal ureter ureterorenoscopy ESWL ; treatment of choice in 85% of pts.

59
Management of renal & ureteral stones cont … Medical therapy : Medical therapy doesn ’ t dissolve preexisting Ca stones thus the passage of such stones can occur and does not represent a treatment failure. Acute therapy : Conservative : pain control, hydration, until stone passage. Average time for stone passage : Stone <= 2 mm : 8 days Stones 2- 4 mm : 12 days Stones >= 4 mm : 22 days

60
Management of renal & ureteral stones cont … 1. Pain control: NSAID – Narcotics - Desmopressin NSAID are as effective as opiates, but more pain relief at 10 min ( 100 mg rectal indomethacin vs. 5-10 mg IV morphine ). Or ; iv ketorolac ( 60 mg ) more pain relief vs.( 50 mg) iv meperidin NSAIDs : 1- decreased ureteral smooth muscle tone 2- discourages opiate – seeking patients 3- may induce ARF 4- should be stop 3 days before SWL(because of bleeding ). Intranasal Desmopressin : effective for renal colic. Hospitalization : who can not tolerate oral intake or have very severe pain.
. Or ; iv ketorolac ( 60 mg ) more pain relief vs.( 50 mg) iv meperidin NSAIDs : 1- decreased ureteral smooth muscle tone 2- discourages opiate – seeking patients 3- may induce ARF 4- should be stop 3 days before SWL(because of bleeding ). Intranasal Desmopressin : effective for renal colic. Hospitalization : who can not tolerate oral intake or have very severe pain..")
61
Management of renal & ureteral stones cont … 2. Straining urine and bring any stone that passes. 3. Urology consultation : * urosepsis * ARF * failure to pass the stone after 2- 4 weeks * stone > 5 mm * uncontrolled pain

62
Management of renal & ureteral stones cont … Chronic prevention of recurrent stones : 1- reactants 2- inhibitors Monitoring of response : 1)One or two 24 hours urine at 6-8 wk after therapy. 2)Repeat values at yearly,then q 2-4 years 3)Periodic U.S. at 1 year, then q 2-4 years
Repeat values at yearly,then q 2-4 years 3)Periodic U.S. at 1 year, then q 2-4 years.")
63
Management of renal & ureteral stones cont … Dietary modification : High fluid intake > 2 L /d, also at night Reduced animal protein intake ( sulfuric acid) (adverse changes in urine Ca, uric acid & citrate ) 1 g / kg /d. Limit Na intake : low Na diet (80-100 meq/d ), Ca & Na reabsorption in proximal tubule Ca excretion.
, Ca & Na reabsorption in proximal tubule Ca excretion..")
64
Management of renal & ureteral stones (cont … ) Calcium intake : Limiting Ca intake not recommended. A low Ca diet may have a second deleterious effect in idiopathic hypercalciuria ; wasting of Ca from the bone and the kidney, results in diminished bone density.

65
Management of renal & ureteral stones cont … Drug therapy : Indications :Active stone disease : Formation of new stones Enlargement of old stones Passage of gravels (Despite initial drug therapy over a six months period ).
.")
66
Management of renal & ureteral stones cont … Initial drug therapy : Thizides for hypercalciuria Potassium citrate or allopurinol for hyperuricosuria Potassium citrate for hypocitraturia Potassium citrate for type one RTA

67
Management of renal & ureteral stones cont … Idiopathic hypercalciuria (not PHP or sarcoidosis ) Normal Ca diet ( Ca intake risk stone ) Low animal protein Low salt diet Thiazide diuretics (chlorthalidone or HCTZ ) urine Ca as much as 150 mg/d. 90% in incidence of new stones, dose 12.5- 25mg/d. bone mineral density, hip fractures.

68
Management of renal & ureteral stones cont … Idiopathic hypercalciuria : cont … Avoid hypokalemia urine citrate excretion Amiloride ( K- sparing diuretic ) 5-10 mg /d. Ca reabsorption in CCT Ca excretion. K HCO3 or K citrate ( 60-80 meq /d ) not Na ; Plasma alkali Ca reabsorption Ca excretion. Plasma alkali urine excretion of citrate. Na causes volum expansion Na & Ca excretion. Neutral phosphate (orthophosphate) : Ca excretion & crystalization inhibitors excretion ( pyrophosphate ).
 not Na ; Plasma alkali Ca reabsorption Ca excretion. Plasma alkali urine excretion of citrate. Na causes volum expansion Na & Ca excretion. Neutral phosphate (orthophosphate) : Ca excretion & crystalization inhibitors excretion ( pyrophosphate )..")
69
Management of renal & ureteral stones cont … Hyperuricosuria : if diet is ineffective : Allopurinol 100- 300 mg/d,80% in new stone formation. Alkali therapy by K citrate, 60- 80 meq /d, urine PH > 6 insoluble uric acid to soluble urate salt.

70
Management of renal & ureteral stones cont … Hypocitraturia : K citrate or KHCO3 30-80 meq/d,alkakizing the plasma citrate excretion, in contrast, KCl does not increase citrate excretion in Nl K,because it is a non-alkalizing salt. Orange juice ( K citrate,Ca ox,Ascorbic acid ): citrate excretion, Ca excretion not lower, Oxalate excretion modestly increased ( ascorbic acid ) Lemon juice ( citrate ): (intolerant to citrate ) 4 ounce /d + urine citrate tap water = 2 L/d (lemonade) urine Ca urine Ox didn ’ t alter
: citrate excretion, Ca excretion not lower, Oxalate excretion modestly increased ( ascorbic acid ) Lemon juice ( citrate ): (intolerant to citrate ) 4 ounce /d + urine citrate tap water = 2 L/d (lemonade) urine Ca urine Ox didn ’ t alter.")
71
Management of renal & ureteral stones cont … Enteric hyperoxaluria : Fluid intake Potassium citrate Oral Ca Co3 ( 1- 4 gm daily) Fat – oxalate diet Cholestyramine (binds both Bile acid & Ox )
 Fat – oxalate diet Cholestyramine (binds both Bile acid & Ox )")
72
Management of renal & ureteral stones cont … No metabolic abnormality : Have more Ca & less citrate in the urine than normals, but neither is clearly abnormal. Have a lower urine volume. Treatment : Thiazide even in normocalcemic urine. K citrate remains to be determined. Neutral phosphate 2 g m /d. Ca Ph stones : have persistently urine PH, Treatment : K citrate.

73
Management of renal & ureteral stones cont … Cyctine : High water intake Urine Ph > 7-7.4 K citrate 3-4 meq/kg Low intake of Na 50 meq/d ( cystin excretion ) Penicillamine, tiopronin, captopril
 Penicillamine, tiopronin, captopril")
Similar presentations









 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")


 is well- documented common occurrences in the general population nephrolithiasis (kidney calculi.>")

 RENAL DISEASE: RENAL STONES AND UT OBSTRUCTION Pathophysiology of Disease: Chapter 16 (401-404) Jack DeRuiter,>")






 Triple phosphate237 (26.4%) Phosphate119 (13.4%) Uric.>")




