Download presentation
Presentation is loading. Please wait.

1
Nursing Care of Clients with Gallbladder, Liver and Pancreatic Disorders Chapter 27

2
Liver, Gallbladder and Pancreas

3
Gallbladder Disorders Cholelithiasis- Formation of stones Cholecystitis-Inflammation of the gallbladder Patho&risk- age, hx, gender, OC –gallstones form due to abnormal bile composition biliary statis inflammation of gallbladder

4
Gallbladder Disorders Cholelithiasis asymptomatic epigastric fullness after fatty meal biliary colic jaundice Acute cholecystitis RUQ pain - back a/n/v fever with chills

5
Gallbladder Disorders 4 Treatment –laparoscopic cholecystectomy 4 Nursing Diagnoses –Pain –Imbalanced Nutrition –Risk for Infection

6
Liver

7
Hepatitis

9
Liver Disorders 4 Hepatitis –inflammation of the liver due to virus, ETOH, drugs, toxins, may be acute or chronic 4 Viral Hepatitis 4 Hepatitis A - infectious hepatitis –fecal-oral route –benign, self-limiting

10
Liver Disorders 4 Hepatitis B –transmission - infected blood and body fluids at risk - healthcare workers, drug users, multiple sexual partners, hemodialysis clients 4 Hepatitis C –transmission - infected blood and body fluids –manifestations - mild, non-specific –world wide cause of chronic hepatitis

11
Liver Disorders 4 Disease pattern –Onset –Transmission –Carrier –Prevent –Treatment

12
Hepatitis Course of acute viral hepatitis follows three phases: Preicteric- abruptly before jaundice Icteric- after 5-10 days of exposure Convalescent- well being improves, energy increases, jaundice resolves. See book.

13
Liver Disorders 4 Nursing Care –teaching handwashing blood and body fluid precautions vaccines for persons at high risk

14
Advanced Cirrhosis

15
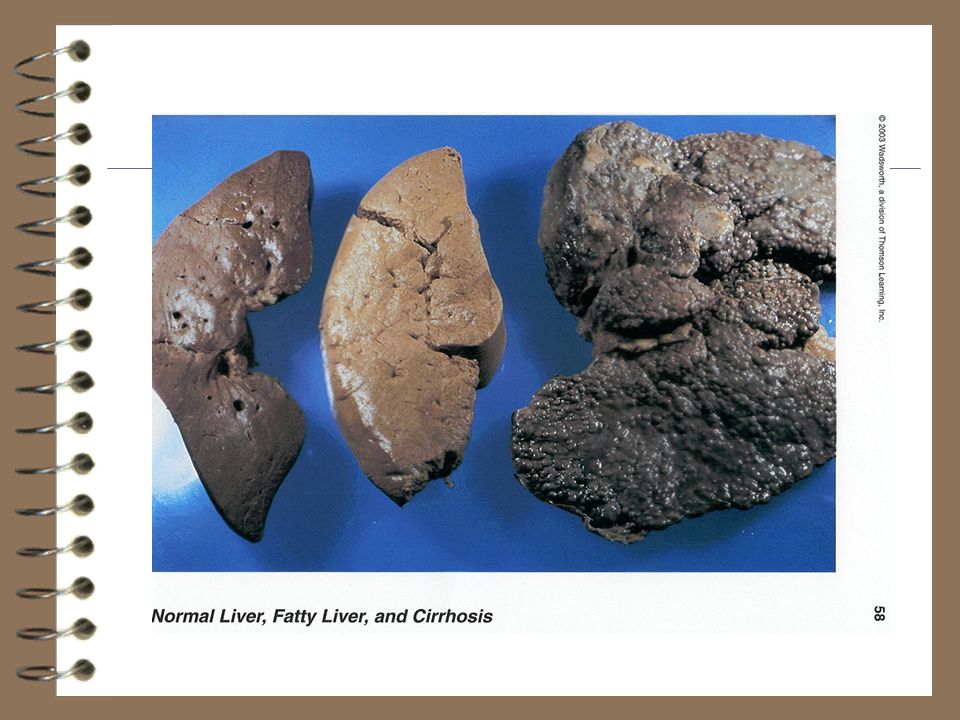
Liver Disorders 4 Cirrhosis –end state of chronic liver disease, progressive and irreversible alcoholic cirrhosis, biliary, or secondary to hepatitis –Manifestations liver enlg. Tender, wt loss, weakness, anorexia ascites, jaundice, edema, anemia,

16
Cirrhosis of the Liver Functional liver tissue is gradually destroyed and replaced with fibrous scar tissue, thus metobolic functions of the liver are lost. The scar tissue forms constrictive bands in the liver and disrupts blood and bile flow within the liver. Impaired blood flow through the liver increases pressure in the portal venous system, thus leading to many problems including esophageal varices. Discussion see book.

17
Cirrhosis of the Liver As the liver is destroyed it’s ability to metabolize proteins is impaired!!! Ammonia and toxic wastes accumulate in the blood, these substances affect the CNS!!! Hepatic Encephalopathy is the result of accumulated ammonia and toxic wastes(protein). CM are altered levels of consciousness, cognition and motor function. Asterixis or liver flap is an early CM of hepatic encephalopathy. This is a muscle tremor that causes involuntary jerking movements that make it difficult to keep the extremities still
. CM are altered levels of consciousness, cognition and motor function. Asterixis or liver flap is an early CM of hepatic encephalopathy. This is a muscle tremor that causes involuntary jerking movements that make it difficult to keep the extremities still.")
18
Liver Disorders 4 Complications –portal hypertension –splenomegaly –ascites –esophageal varices –hepatic encephalopathy –hepatorenal syndrome

19
Hepatitis Nursing Care- Supportive care. Prevent transmission of disease!! Teaching needs- If at risk, need vaccine!!!!! Complications- Cirrhosis!

20
Pancreatitis 4 Pancreatitis –inflammation of pancreas characterized by release of pancreatic enzymes into pancreatic tissue itself leading to hemorrhage and necrosis 4 Risk factors –alcoholism, gallstones

21
Pancreatitis 4 Manifestations –abrupt onset of severe epigastric/abdominal pain relieved by leaning forward, sitting up initiated by fatty meal or alcohol intake –n/v –abd. distention and rigidity, decreased b.s. –fever, 24 hours later jaundice

22
Pancreatitis

23
4 Diagnostic tests –labs - amylase and lipase –Ultra sound, ERCP, C-T scan, needle bx 4 Treatment –NPO,hydration, pain control and antibiotics

24
Pancreatitis Can be acute or chronic Acute- middle life from gallstones and alcoholism which are the primary risk factors Chronic- Alcoholism is the primary risk factor. Pancreatic duct obstruction by a gallstone or spasm of the sphincter of oddi can obstruct the outflow of pancreatic enzymes then auto digestion begins. See text

25
Pancreatic Cancer 4 Very lethal 4 Risk factors –smoking, chemical or environmental toxins 4 Manifestations –non-specific, a/n, wt. loss, dull epigastric pain 4 Treatment –surgery - Whipple, radiation and chemotherapy

26
NCLEX A client diagnosed with cholelithiasis requests medication for pain relief. Which of the following medications is the provider most likely to prescribe? A. Acetaminophen (Tylenol) D. ibuprofen B. Meperidine (Demerol)(Motrin) C. Morphine Sulfate
 D. ibuprofen B. Meperidine (Demerol)(Motrin) C. Morphine Sulfate.")
27
NCLEX A client who was diagnosed with hepatitis A state he was told by the nursing assistant that his disease could be transmitted only through blood contact. The appropriate action by the nurse would be to: A. Provide the correct information to the client and nursing assistant. B. Take no further action because the information is correct. C. Remove all precautions because hepatitis A cannot be transmitted D. Place a sign on the client’s door stating “blood precautions.”

28
NCLEX A client is diagnosed with hepatitis B. Which of the following information, if obtained during the admission assessment would indicate a risk factor? A. She ate in a dirty restaurant 2 weeks ago B. She uses barrier protection during sex C. She is an intravenous drug user D. She has never received a blood transfusion

29
NCLEX The nurse is caring for a client with acute pancreatitis. Which nursing assessment should receive the highest priority? A. Assess intake and output B. Assess cardiovascular status and fluid volume status C. Assess bowel sounds and fecal output D. Assess mental status

30
NCLEX A client with cirrhosis is scheduled for discharge. The nurse recognized the need for further teaching if the client states A. I will use a soft toothbrush for oral hygiene B. I will maintain a low-protein diet C. I will report increased difficulty breathing to my provider D. I will limit alcohol intake to two servings per day

31
NCLEX A 45 –year old client with liver disease is prescribed lactulose (Chronulac) 30 ML every 6 hours. Recognizing the action of this medication in the treatment of liver disease, the nurse would expect to assess which positive response to the medication? A. Increased urine output B. Reduced serum ammonia levels C. Reduced steatorrhea D. Increased serum potassium levels

32
NCLEX A patient tells the nurse that his bowel movements are weird in that they look soapy and smell really bad. The nurse realizes that this client might be experiencing: A. A. an obstructed gallbladder B. B. turner’s sign C. C.cullen’s sign D. D. steatorrhea

33
Ammonia Levels and liver failure Ammonia levels are elevated because of inability of the liver to metabolize protein products. The medication Lactulose increases the absorption of ammonia from the bowel, thus reducing blood ammonia levels. What do we see clinically in a patient who’s blood ammonia levels are too high from liver cirrhosis? What is Asterixix? What type of diet should the patient with cirrhosis of the liver and hepatic encephalopathy be prescribed?

34
Pancreatitis Acute- The pancreas is damaged or its duct to the duodenum is blocked, allowing pancreatic enzymes to accumulate within the pancreas. Pancreatic duct obstruction by a gallstone or spasm of the sphincter of Oddi which is associated with alcohol use can obstruct the outflow of pancreatic enzymes. This creates autodigestion. Steatorrhea- Fatty stool. Alcoholism is the primary risk factor for chronic pancreatitis in the US. Labs of importance: Serum amylase and lipase will be elevated during pancreatitis.

Similar presentations










 that progresses to cirrhosis Replacement of liver tissue.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")







