Download presentation
Presentation is loading. Please wait.

1
Organ donation Peter Bishop Clinical lead for organ donation

2
Number of deceased donors and transplants in the UK 1 April 1999 - 31 March 2009 - patients on the active transplant lists at each year

3
Number of deceased donors and transplants in the UK 1000+ patients die on transplant waiting list each year1000+ patients die on transplant waiting list each year Access to waiting lists is cappedAccess to waiting lists is capped Live related liver transplantsLive related liver transplants 50% mortality rate for CF patients awaiting transplants50% mortality rate for CF patients awaiting transplants 1 April 1999 - 31 March 2009 - patients on the active transplant lists at 31 March

4
Donors pmp

5
Organ Donors in Spain Numbers & Annual Rate (p.m.p) 50% increase in 5 years 550 687 778 832 865 960 1037 1032 1155 1250 1334 1345 1335 1411
 50% increase in 5 years")
6
Organ Donation Taskforce Terms of reference To identify barriers to donation and transplantation and recommend solutions within existing operational and legal frameworks in England Target – 50% increase in donation over 5 years Elisabeth Buggins CBE

7
A UK Model for Donation NHSBT Department of Health Acute Hospital Trusts More donors National ODO Effective co-ordination and retrieval Education, training and audit Public engagement Funding Resolution of ethical and legal issues Performance Management Training Public recognition Clinical leads Embedded co-ordinators Donation committees

8
Key recomendations 1.A UK-wide Organ Donation Organisation should be established 2.The establishment of the Organ Donation Organisation should be the responsibility of NHS Blood and Transplant. 3.Urgent attention is required to resolve outstanding legal, ethical and professional issues in order to ensure that all clinicians are supported and are able to work within a clear and unambiguous framework of good practice. Additionally, an independent UK-wide Donation Ethics Group should be established. 4.All parts of the NHS must embrace organ donation as a usual, not an unusual event. Local policies, constructed around national guidelines, should be put in place. Discussions about donation should be part of all end-of-life care when appropriate. Each Trust should have an identified clinical donation champion and a Trust donation committee to help achieve this. 5.Minimum notification criteria for potential organ donors should be introduced on a UK-wide basis. These criteria should be reviewed after 12 months in the light of evidence of their effect, and the comparative impact of more detailed criteria should also be assessed. 6.Donation activity in all Trusts should be monitored. Rates of potential donor identification, referral, approach to the family and consent to donation should be reported. The Trust donation committee should report to the Trust Board through the clinical governance process and the medical director, and the reports should be part of the assessment of Trusts through the relevant healthcare regulator. Benchmark data from other Trusts should be made available for comparison. 7.BSD testing should be carried out in all patients where BSD is a likely diagnosis, even if organ donation is an unlikely outcome. 1.Financial disincentives to Trusts facilitating donation should be removed through the development and introduction of appropriate reimbursement 2.The current network of DTCs should be expanded and strengthened through central employment by a UK-wide Organ Donation Organisation. Additional co-ordinators, embedded within critical care areas, should be employed to ensure a comprehensive, highly skilled, specialised and robust service. There should be a close and defined collaboration between DTCs, clinical staff and Trust donation champions. Electronic on-line donor registration and organ offering systems should be developed. 3.A UK-wide network of dedicated organ retrieval teams should be established to ensure timely, high-quality organ removal from all heartbeating and nonheartbeating donors. The Organ Donation Organisation should be responsible for commissioning the retrieval teams and for audit and performance management 4.All clinical staff likely to be involved in the treatment of potential organ donors should receive mandatory training in the principles of donation. There should also be regular update training 5.Appropriate ways should be identified of personally and publicly recognising individual organ donors, where desired. These approaches may include national memorials, local initiatives and personal follow-up to donor families 6.There is an urgent requirement to identify and implement the most effective methods through which organ donation and the ‘gift of life’ can be promoted to the general public, and specifically to the BME population. Research should be commissioned through Department of Health research and development funding. 7.The Department of Health and the Ministry of Justice should develop formal guidelines for coroners concerning organ donation

9
Donation committee Non clinical Chair Mr Gerald Coteman Clinical lead for organ donation Intensive care clinical and nursing Emergency Physician Paediatricians Bereavement Chapliancy PALS

10
Princess Alexandra ITU Deaths

11
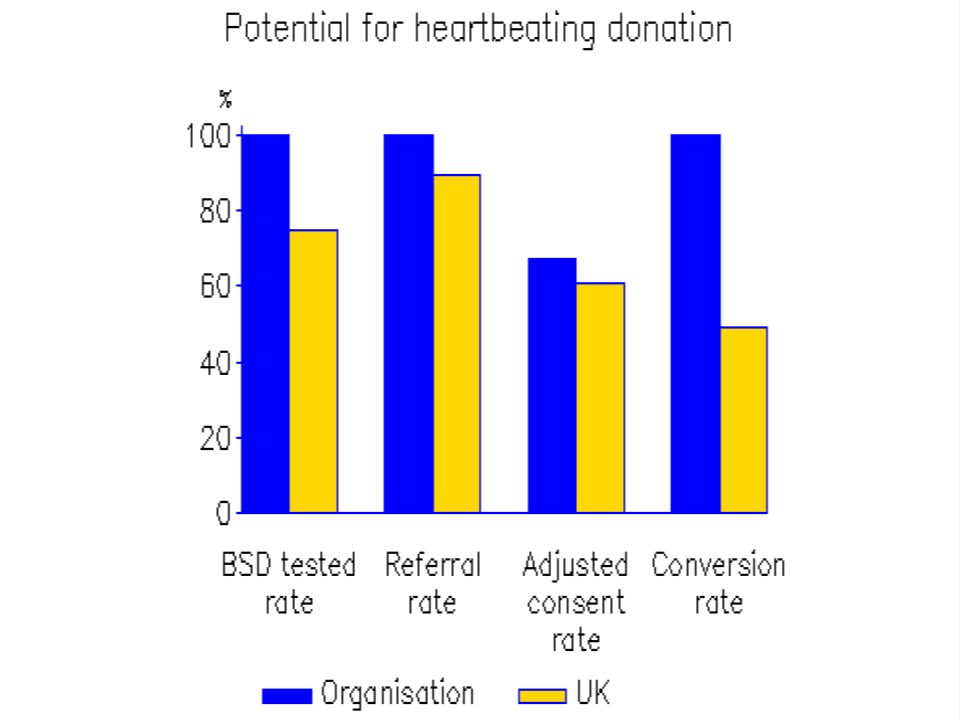
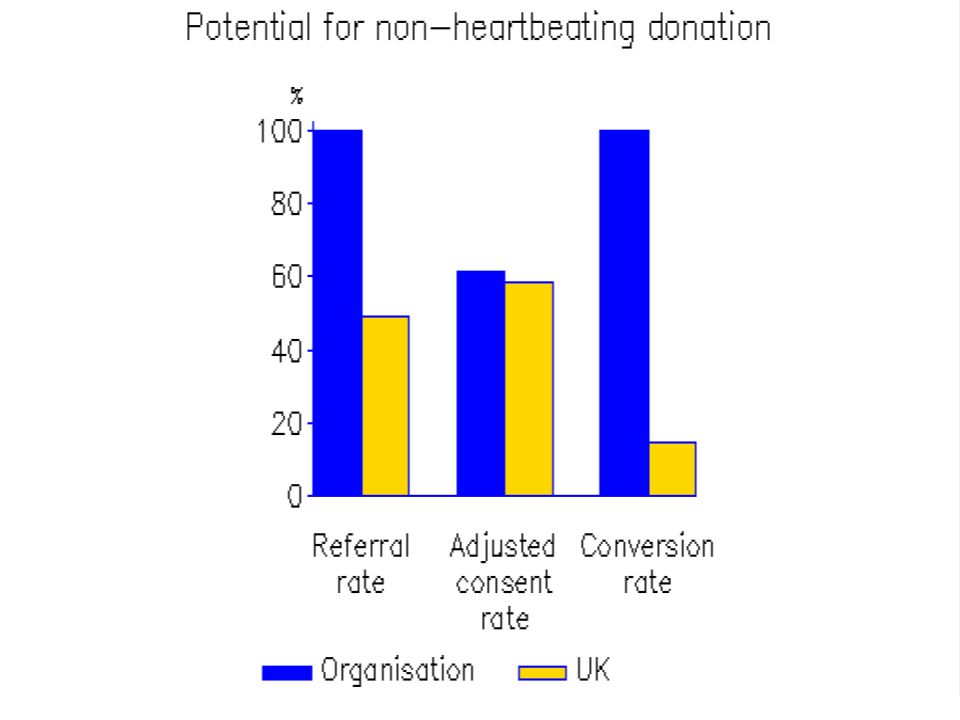
ITU Donor Potential and Organ Donors

14
Financial disincentives NHSBT fixed rate tariff £2086 per donor NHSBT finance 1 PA to support the work of the CLOD £2000pa to support the donation committee Critical care capacity

15
Future activity Embedded donor coordinator Local awareness Donor register Non heart beating programme End of life policy Tissue donation

Similar presentations






 Act 2013 Making it work 13/10/2014.>")


? Federally designated, not-for-profit organ, tissue, and eye procurement.>")



 Act 2013 Making it work 2/12/2014.>")





