Download presentation
Presentation is loading. Please wait.

1
Systemic Lupus Erythematosus

2
Introduction Autoimmune disease Multi system involvement Organs damage – Autoantibodies – Immune complexes

3
Epidemiology All genders, ages, and ethnic groups Women of childbearing years (90%) Female/ men: 9/1 * Iran: 9/1 Prevalence – 10 to 400 per 100,000 (United States) – 40 per 100,000 (Iran) – Highest in black women – Lowest is in white men
 Female/ men: 9/1 * Iran: 9/1 Prevalence – 10 to 400 per 100,000 (United States) – 40 per 100,000 (Iran) – Highest in black women – Lowest is in white men")
4
PATHOGENESIS OF SLE 1- Genetic bases 2- Environmental factors 3- Autoantibodies 4- B-cell abnormalities 5- T-cell abnormalities 6- Immunoregulation inability

5
Susceptibility Abnormal immune response Auto Abs & ICs Inflammation Damage Pathogenesis ?

6
Pathogenesis and Etiology

7
Pathogenesis Abnormal immune responses (1) Activation of innate immunity – Dendritic cells, monocyte/macrophages (2) Lowered thresholds and abnormal activation activation in adaptive immunity cells – T and B lymphocytes
 Activation of innate immunity – Dendritic cells, monocyte/macrophages (2) Lowered thresholds and abnormal activation activation in adaptive immunity cells – T and B lymphocytes")
8
Pathogenesis (3) Ineffective regulatory – CD4+ and CD8+ T cells (4) Reduced clearance – Immune complexes – Apoptotic cells
 Ineffective regulatory – CD4+ and CD8+ T cells (4) Reduced clearance – Immune complexes – Apoptotic cells")
9
Pathogenesis Immune cell activation Proinflammatory cytokines – IFNs – Tumor necrosis factor – Interleukin (IL)-17 – B cell–maturation/survival cytokines B lymphocyte stimulator (BLyS/BAFF) – IL-10
-17 – B cell–maturation/survival cytokines B lymphocyte stimulator (BLyS/BAFF) – IL-10")
10
Pathogenesis Immune cell activation Lupus T and natural killer (NK) cells fail to produce – IL-2 – Transforming growth factor (TGFβ)
 cells fail to produce – IL-2 – Transforming growth factor (TGFβ)")
11
Clinical Manifestations

12
Systemic (95%) – Fatigue – Malaise – Fever – Anorexia – Weight loss
 – Fatigue – Malaise – Fever – Anorexia – Weight loss")
13
Musculoskeletal (95%) Arthralgias/myalgias Intermittent polyarthritis – Hands, wrists, and knees Joint deformities (hands and feet) – Only 10% – Erosions on joint x-rays are rare
 Arthralgias/myalgias Intermittent polyarthritis – Hands, wrists, and knees Joint deformities (hands and feet) – Only 10% – Erosions on joint x-rays are rare")
14
Musculoskeletal (95%) Ischemic necrosis of bone (15%) Myositis (5%) Muscle weakness – Glucocorticoid therapies (commonly) – Antimalarial therapies (rarely)
 Ischemic necrosis of bone (15%) Myositis (5%) Muscle weakness – Glucocorticoid therapies (commonly) – Antimalarial therapies (rarely)")
16
Cutaneous Manifestations (80%) Acute – Localized – Generalized
 Acute – Localized – Generalized")
17
Butterfly rash (discoid type)
")
18
Cutaneous Manifestations (80%) Oral ulcer (40%) Erythema on soft and hard palate Buccal mucosa Without pain Malar rash (50%) Nasal ulcer lower nasal septum Bilateral Active disease
 Oral ulcer (40%) Erythema on soft and hard palate Buccal mucosa Without pain Malar rash (50%) Nasal ulcer lower nasal septum Bilateral Active disease")
19
Cutaneous Manifestations (80%) Subacute cutaneous LE (SCLE) Annular Papulosqumous (psoriasiform)
 Subacute cutaneous LE (SCLE) Annular Papulosqumous (psoriasiform)")
20
Cutaneous Manifestations (80%) Chronic – DLE (20%) Localized Generalized – Lupus panniculitis (profundus) – Mucosal LE – Tumid lupus
 Chronic – DLE (20%) Localized Generalized – Lupus panniculitis (profundus) – Mucosal LE – Tumid lupus")
21
Cutaneous Manifestations (80%) Vasculitis (20%) – Palpable purpura – Urticarial vasculitis – Polyarteritis nodosa–like – Livedo reticularisa
 Vasculitis (20%) – Palpable purpura – Urticarial vasculitis – Polyarteritis nodosa–like – Livedo reticularisa")
22
Renal Manifestations (50%) Nephritis – Most serious manifestation – Asymptomatic (most lupus patients) Urinalysis should be ordered in any person suspected of having SLE
 Nephritis – Most serious manifestation – Asymptomatic (most lupus patients) Urinalysis should be ordered in any person suspected of having SLE")
23
Renal Manifestations Nephritis – Proteinuria 500 mg/24 h, cellular casts (30–50%) – Nephrotic syndrome (25%) End-stage renal disease (5–10%)
 – Nephrotic syndrome (25%) End-stage renal disease (5–10%)")
24
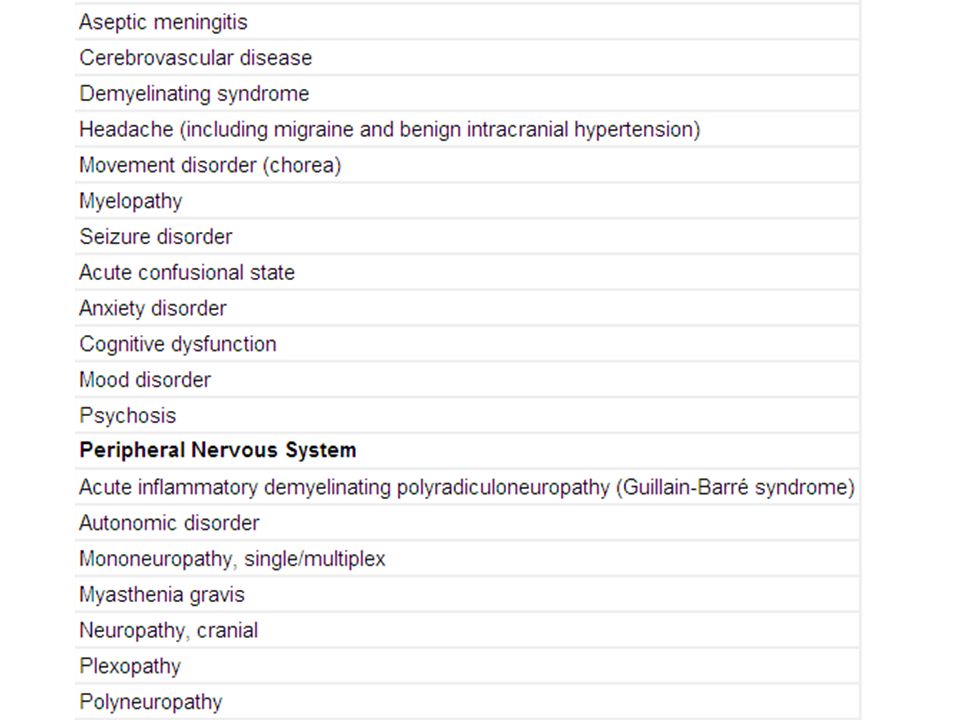
Nervous System Manifestations (60%) Central nervous system (CNS) Peripheral nervous system Cognitive dysfunction (most common)(50%) – Difficulties with memory and reasoning Headaches Psychosis Glucocorticoid-induced psychosis Myelopathy Infection
 Central nervous system (CNS) Peripheral nervous system Cognitive dysfunction (most common)(50%) – Difficulties with memory and reasoning Headaches Psychosis Glucocorticoid-induced psychosis Myelopathy Infection")
27
Cardiopulmonary (60%) Pleurisy, pericarditis, effusions (30–50%) Myocarditis, endocarditis (10%) Coronary artery disease (10%)
 Pleurisy, pericarditis, effusions (30–50%) Myocarditis, endocarditis (10%) Coronary artery disease (10%)")
28
Cardiopulmonary (60%) Lupus pneumonitis (10%) Interstitial fibrosis (5%) Shrinking lung syndrome (<5%) Pulmonary hypertension, ARDS, hemorrhage (<5%)
 Lupus pneumonitis (10%) Interstitial fibrosis (5%) Shrinking lung syndrome (<5%) Pulmonary hypertension, ARDS, hemorrhage (<5%)")
29
Gastrointestinal (40%) Nonspecific (30%) – Nausea – Mild pain – Diarrhea Abnormal liver enzymes (40%) Vasculitis (5%) Thrombosis (15%)
 Nonspecific (30%) – Nausea – Mild pain – Diarrhea Abnormal liver enzymes (40%) Vasculitis (5%) Thrombosis (15%)")
30
Ocular (15%) Sicca syndrome (15%) Conjunctivitis, episcleritis (10%) Vasculitis (5%)
 Sicca syndrome (15%) Conjunctivitis, episcleritis (10%) Vasculitis (5%)")
31
Clinical Manifestations Thrombosis (15%) – Venous (10%) – Arterial (%5)
 – Venous (10%) – Arterial (%5)")
32
Hematologic (85%) Anemia (chronic disease) (70%) Leukopenia (<4000/L) (65%) Lymphopenia (<1500/L) (50%) Thrombocytopenia (100,000/L) (15%) Lymphadenopathy (15%) Splenomegaly (15%) Hemolytic anemia (10%)
 Anemia (chronic disease) (70%) Leukopenia (<4000/L) (65%) Lymphopenia (<1500/L) (50%) Thrombocytopenia (100,000/L) (15%) Lymphadenopathy (15%) Splenomegaly (15%) Hemolytic anemia (10%)")
33
SLE in IRAN: 2280 patients (1976-2009) Musculoskeletal: 83.2% Cutaneous: 81% Renal: 65.4% Neuropsychiatric: 23.4% Pulmonary: 21.5% Cardiac: 17.2% Hematologic: 66.4% Renal involvement more than some european countries
 Musculoskeletal: 83.2% Cutaneous: 81% Renal: 65.4% Neuropsychiatric: 23.4% Pulmonary: 21.5% Cardiac: 17.2% Hematologic: 66.4% Renal involvement more than some european countries")
34
Laboratory Tests Aims – Establish or rule out the diagnosis – Follow the course of disease Flare or organ damage – Identify adverse effects of therapies

35
Laboratory Tests Autoantibodies ANA (>95%) High-titer IgG antibodies to double-stranded DNA (dsDNA) Antibodies to Sm (specific) Anti phospholipid antibody Anti-Ro – Neonatal lupus – Sicca syndrome – SCLE. Declining levels of C3 or C4 complement

36
Immunofluorescent staining of ANAs 1. Homogenous (diffuse) deoxy RNA protein, histone (SLE, DIL, RA ) 2. Rim (peripheral) dsDNA, histone characteristic of SLE
 deoxy RNA protein, histone (SLE, DIL, RA ) 2. Rim (peripheral) dsDNA, histone characteristic of SLE.")
37
Urine sediment Hematuria: RBC > 5 Dysmorphic (fragmented, abnormal sizes and shapes) Pyuria: WBC > 5 RBC, WBC, mixed cast NEPHRITIC Granular, fatty cast PROTEINURIC Broad, waxy cast CRF
 Pyuria: WBC > 5 RBC, WBC, mixed cast NEPHRITIC Granular, fatty cast PROTEINURIC Broad, waxy cast CRF")
38
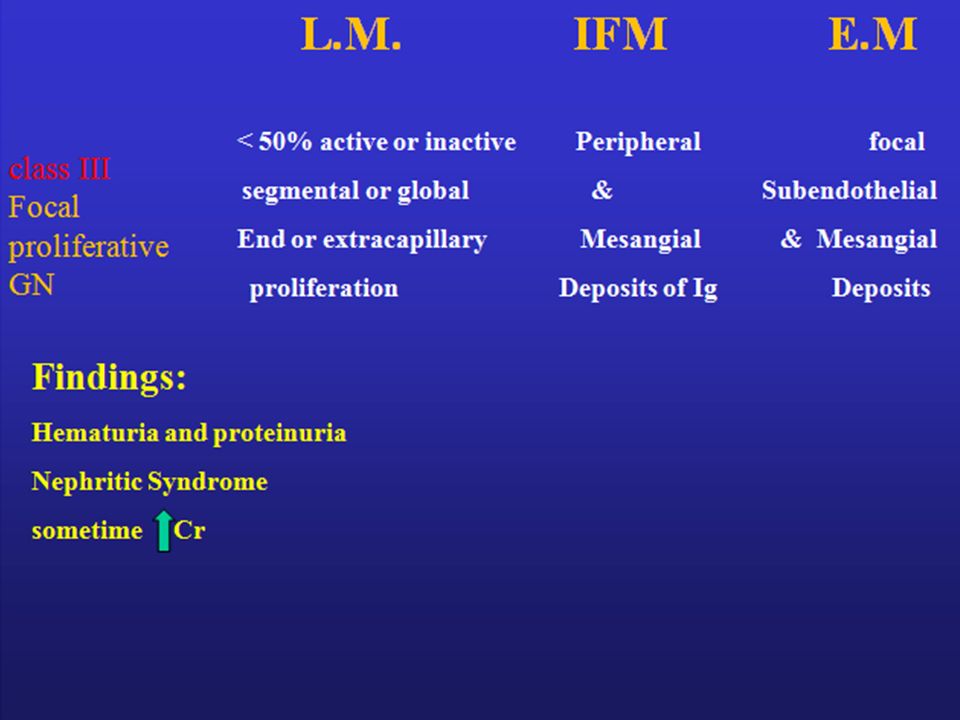
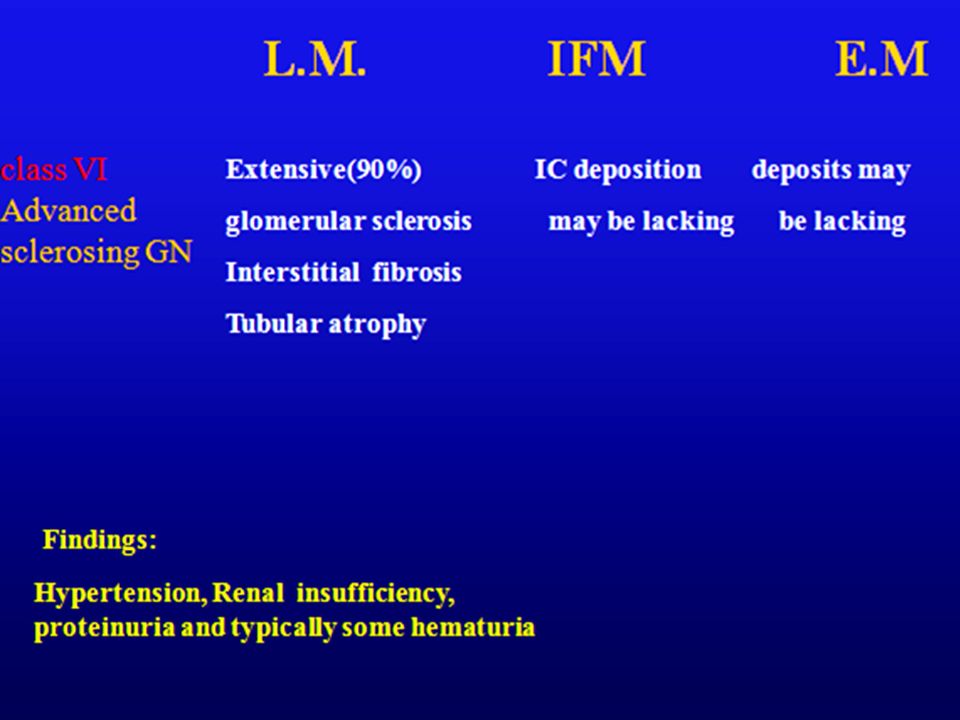
WHO Classification of Nephritis Class I Normal Class II Mesangial GN Class III Focal Segmental GN Class IV Diffuse Proliferative GN Class V Diffuse Membranous GN Class VI Glomerulosclerosis

40
Class II Mesangial proliferative GN

43
Class IV Diffuse proliferative GN Normal glomerulus

45
Membranous GN

47
Laboratory Tests Skin biopsy Deposition of Ig at the dermal-epidermal junction (DEJ) – Clinically unaffected skin
 – Clinically unaffected skin")
48
Laboratory Tests Standard Tests for diagnosis – Auto antibodies Screening tests – Complete blood count – Platelet count – Urinalysis may detect abnormalities

49
Diagnosis Diagnosis ACR Criteria for Systemic Lupus Erythematosus 1.Malar rash 2.Discoid rash 3.Photosensitivity 4.Oral ulcers 5.Arthritis – Nonerosive arthritis of two or more peripheral joints 6.Serositis – Pleuritis or pericarditis documented by ECG or rub or evidence of effusion

50
Diagnosis Diagnosis ACR Criteria for Systemic Lupus Erythematosus (cont.) 7. Renal disorder Proteinuria > 0.5 g/d or 3+ Or cellular casts 8. Neurologic disorder – Seizures or psychosis without other causes 9. Hematologic disorder – Hemolytic anemia or leukopenia (<4000/L) or – Lymphopenia (<1500/L) or – Thrombocytopenia (<100,000/L)
 or – Lymphopenia (<1500/L) or – Thrombocytopenia (<100,000/L).")
51
Diagnosis Diagnosis ACR Criteria for Systemic Lupus Erythematosus (cont.) >/= 4 criteria, Specificity and sensitivity are 95% and 75%, respectively 10. Immunologic disorder – Anti-dsDNA, anti-Sm, and/or anti-phospholipid 11. Antinuclear antibodies – An abnormal titer of ANA – Absence of drugs known to induce ANAs

53
Treatment

55
Major organ involvement Nephritis Proliferative or membranous nephritis Hematologic Severe thrombocytopenia (< 20 × 103/μL) TTP–like syndrome, AA, sever hemolytic Lupus pneumonitis or alveolar hemorrhage Cardiac Myocarditis, pericarditis (impending tamponade) Abdominal vasculitis Nervous system Transverse myelitis, Cerebritis Vasculitis, neuropathy Psychosis resistance to GC
 TTP–like syndrome, AA, sever hemolytic Lupus pneumonitis or alveolar hemorrhage Cardiac Myocarditis, pericarditis (impending tamponade) Abdominal vasculitis Nervous system Transverse myelitis, Cerebritis Vasculitis, neuropathy Psychosis resistance to GC")
56
NSAIDs Side effects – Aseptic meningitis – Transaminitis – Decreased renal function – Vasculitis of skin – Myocardial infarction (esp cox2 I) Drugs Both GI events and symptoms Allergic Reactions Dermatitis Dizziness Acute Renal Failure Edema Hypertension
 Drugs Both GI events and symptoms Allergic Reactions Dermatitis Dizziness Acute Renal Failure Edema Hypertension")
57
Drugs Topical glucocorticoids – Atrophy of skin – Contact dermatitis – Folliculitis – Hypopigmentation, infection Topical sunscreens – Contact dermatitis

58
Drugs Hydroxychloroquine 200–400 mg qd Retinal Damage Agranulocytosis Aplastic Anemia Ataxia Cardiomyopathy Dizziness Myopathy Ototoxicity Peripheral Neuropathy Pigmentation Of Skin Seizures Thrombocytopenia Quinacrine Diffuse yellow skin coloration

59
Antimalarial agents* Reduce the frequency of disease flares (nephritis) Contribute to the maintenance of remission Prolong the onset of disease Reduce the risk of complications *Nature, 2010
 Contribute to the maintenance of remission Prolong the onset of disease Reduce the risk of complications *Nature, 2010")
60
Antimalarial agents* Immunomodulatory effects – Protect against thrombotic events – Improve glucose and lipid profiles – Prevent renal damage – Reduced cardiovascular risk Increased rate of survival lower risk of major infections *Nature, 2010

61
Drugs Methotrexate Dermatitis, arthritis 10–25 mg once a week Anemia bone marrow suppression leukopenia Thrombocytopenia Hepatotoxicity Nephrotoxicity Infections Neurotoxicity Pulmonary fibrosis Pneumonitis Severe dermatitis Seizures

62
Drugs Prednisolone – 0.5–1 mg/kg per day (severe SLE) – 0.07–0.3 mg/kg per day (milder disease) Methylprednisolone sodium – 1 g IV qd x 3 days (severe disease)
 – 0.07–0.3 mg/kg per day (milder disease) Methylprednisolone sodium – 1 g IV qd x 3 days (severe disease)")
63
Drugs Side effects of steroids Infection, VZV infection, hypertension Hyperglycemia, hypokalemia, acne Allergic reactions, anxiety Aseptic necrosis of bone Cushingoid changes, CHF, fragile skin, insomnia Menstrual irregularities, mood swings Osteoporosis Psychosis

64
Drugs Cyclophosphamide – 7–25 mg/kg q month x 6 Infection Bone marrow suppression Hemorrhagic cystitis (less with IV) Carcinoma of the bladder, alopecia, nausea, diarrhea, malaise Malignancy Ovarian and testicular failure
 Carcinoma of the bladder, alopecia, nausea, diarrhea, malaise Malignancy Ovarian and testicular failure")
65
Drugs Mycophenolate mofetil – 2–3 g/d PO Infection leukopenia lymphoproliferative disorders Malignancy Alopecia Cough, diarrhea, fever, GI symptoms, headache Hypertension, hypercholesterolemia, hypokalemia Insomnia, peripheral edema, transaminitis, tremor Rash

66
Drugs Azathioprine – 2–3 mg/kg per day PO Infection Bone marrow suppression Pancreatitis Hepatotoxicity Malignancy Alopecia, fever, flulike illness, GI symptoms

67
Drugs Rituximab – 1 g q 2 wks x 2 Infection Infusion reactions Headache Arrythmias Allergic responses

68
Preventive Therapies Vaccinations – Influenza and pneumococcal vaccines Prevent osteoporosis Control of hypertension Prevention strategies for atherosclerosis Suppressing recurrent urinary tract infections Monitoring and treatment – Dyslipidemias – Hyperglycemia – Obesity

69
Patient Outcomes, Prognosis, and Survival Survival – 95% at 5 years – 90% at 10 years – 78% at 20 years The leading causes of death – First decade of disease Systemic disease activity Renal failure Infections – Thromboembolic events (later)
")
70
Patient Outcomes, Prognosis, and Survival Poor prognosis High serum creatinine levels (>1.4 mg/dL) Hypertension Nephrotic syndrome (24-h urine protein excretion >2.6 g) Anemia (hemoglobin < 12.4 g/dL) Hypoalbuminemia Hypocomplementemia Apl Male sex Ethnicity (African American, Hispanic)
 Hypertension Nephrotic syndrome (24-h urine protein excretion >2.6 g) Anemia (hemoglobin < 12.4 g/dL) Hypoalbuminemia Hypocomplementemia Apl Male sex Ethnicity (African American, Hispanic)")
71
Pregnancy and Lupus Fertility rates for men and women with SLE are probably normal Rate of fetal loss is increased – Two- to threefold High disease activity Antiphospholipid antibodies Active nephritis

72
Pregnancy and Lupus Glucocorticoids (category A) Cyclosporine, Tacrolimus, Rituximab (category C) Azathioprine, Hydroxychloroquine and Mycophenolate mofetil (category D) Methotrexate is (catrgory X)
 Cyclosporine, Tacrolimus, Rituximab (category C) Azathioprine, Hydroxychloroquine and Mycophenolate mofetil (category D) Methotrexate is (catrgory X)")
73
Pregnancy and Lupus Adverse effects of prenatal glucocorticoid exposure (primarily betamethasone) – Low birth weight – Abnormalities in the CNS – Predilection toward adult metabolic syndrome
 – Low birth weight – Abnormalities in the CNS – Predilection toward adult metabolic syndrome")
74
Pregnancy and Lupus Women with SLE usually tolerate pregnancy without disease flares Severe flares (small proportion) – Poor maternal outcomes – Active nephritis – Irreversible organ damage Kidneys Brain Hear t
 – Poor maternal outcomes – Active nephritis – Irreversible organ damage Kidneys Brain Hear t")
75
Drug induced SLE A syndrome of positive ANA – Fever – Malaise – Arthritis or intense arthralgias/myalgias – Serositis – Rash

76
SLE INDUCING DRUGS Hydralazine Procainamide Isoniazid Hydantoins Chlorpromazine Statins Penicillamine Minocycline TNF-α inhibitors Interferon-α Methyldopa

77
Drug induced SLE Rare – kidneys or Brain – Association with anti-dsDNA Antibodies to histones (commonly) Resolves – Several Weeks after discontinuation drug
 Resolves – Several Weeks after discontinuation drug")
78
IN THE NAME OF GOD THE END

Similar presentations









>")
. Definition Epidemiology Pathophysiology Clinical features Classification and diagnosis Treatment Prognosis Lupus related syndromes.>")
 is a chronic inflammatory connective tissue.>")

>")












>")