Download presentation
Presentation is loading. Please wait.

1
BY: Diana Blum RN MSN Metro Community College
OR Experience BY: Diana Blum RN MSN Metro Community College

2
Statistics 2009 Total number of inpatient procedures
performed: 48.0 million Cardiac catheterizations: 1.1 million Coronary artery bypass graft: 415,000

3
Preoperative Begins with the scheduling of procedure
Ends at time of transfer to surgical suite Places emphasis on safety and client education The client’s readiness is critical to the outcome Includes education and intervention to reduce anxiety and complications, and to promote cooperation Communication and collaboration with the surgical team is essential to reach desired outcome

4
Procedures Categorized by: Reason for procedure
Urgency of the procedure Degree of risk Anatomic location GUIDELINES ON P.587

5
Types of Surgery Cosmetic Palliative Reconstructive Elective Urgent
Emergent Curative Exploratory Diagnostic

6
Surgical Areas Preoperative holding area Quiet, calm transition
Equipment includes: 02, EKG machine, BP cuff, code cart RN verifies that all relevant tests and documentation are completed prior to surgery Abnormals reported to MD Confirm NPO status

7
ASSESSMENT Preoperative health evaluation
30 days before surgery, must be documented, clears pt for surgery Pre op history and physical exam Done by anesthesia provider ASA classification, done with any type of sedation (pg 589)
")
8
Risk Factors Elderly Obesity Diabetes Heart conditions Renal failure

9
Assessment History Physical Psychosocial Laboratory Radiographic
Age, drug/ETOH use, meds, alternative meds, medical hx, surgery hx, anesthesia experiences, blood donations, allergies, family hx, type of surgery planned, education recv’d about perioperative period, support system Physical important to obtain baseline assessment, complete vitals, report abnormal findings to doctor Psychosocial Looks at anxiety level, coping ability, and support system Anxiety and fear may influence the amount and type of anesthesia and affect ability to learn, cope, and cooperate Laboratory Provides a baseline for the client Helps predict potential complications Radiographic Provides baseline and looks at size & shape of heart and lungs Diagnostics EKG- used as baseline. Looks for old MI, or other complications that could postpone surgery

11
Question Which diuretic can cause problems in surgery? A. lasix
B. hydrochlorothiazide C. valium D. benadryl

12
Lasix and hydrochlorothiazide may cause excessive respiratory depression resulting from an associated electrolyte imbalance

13
Nursing Diagnosis Disturbed sleep pattern r/t anxiety
Ineffective coping r/t impending surgery Anticipatory grieving r/t effects of surgery Disturbed body image r/t anticipated changes Powerlessness r/t health care environment, loss of independence

14
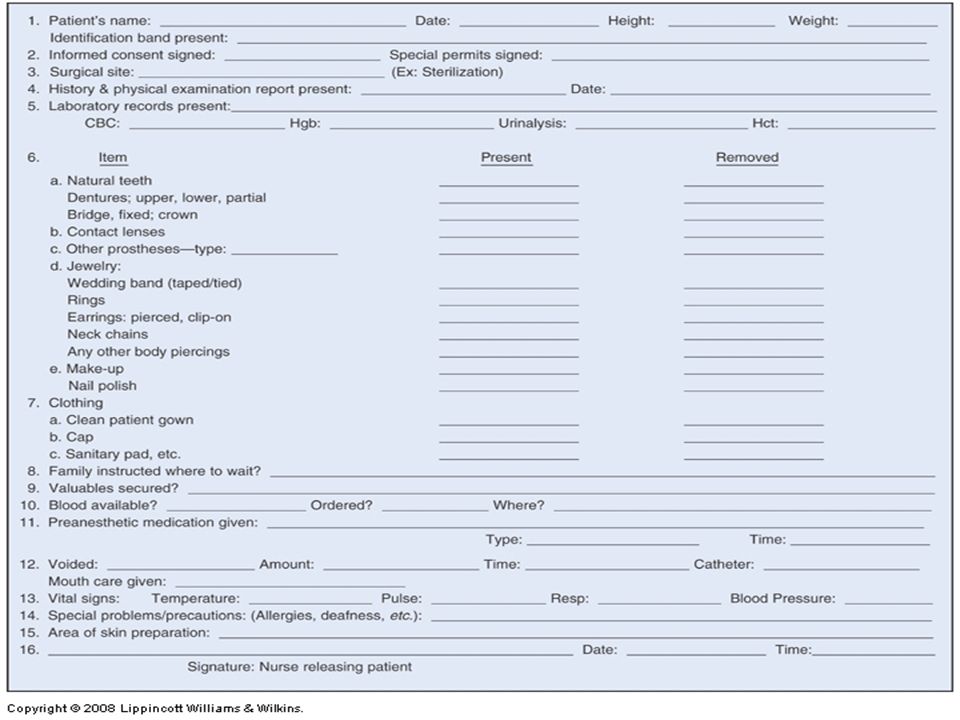
Education Doctor should explain purpose and expected results of surgery Consent needs to be obtained prior to surgery. (if pt signs with an ‘X’ 2 witnesses must sign. Client should ask questions if they don’t understand a term or procedure NPO requirements needs to be explained Preoperative preparations need to be explained (colon prep, or skin prep) Client should understand post op exercises and techniques prior to surgery—I.S., etc.
 Client should understand post op exercises and techniques prior to surgery—I.S., etc.")
15
Informed Consent must be done prior to surgery
Procedure, risks and benefits need to be explained to the patient by the SURGEON The patient must be competent to understand information Consent for blood Consent for anesthesia is separate

16
Legal Responsibilities
DNR DNI Must be clearly documented

17
Surgical Prep Bowel prep Skin prep-shower, hair removal (clippers)
(see pg 610) Preoperative meds Antibiotic
 Preoperative meds. Antibiotic.")
18
Tubes, drains, vascular access
Pt must be educated prior to surgery Reduces fear Tubes Foley- monitors renal function NG-used for abd surgery to decompress the stomach Drains Removes fluid for surgical site. CT, JP, Hemovac, Orthopat Vascular access For anesthesia For drugs and fluids

19
Respiratory education
Incentive spirometry Encourages clients to take deep breaths every 1-2 hours after surgery Usually 10x’s per hour or with each commercial break from a TV show Deep breathing Sit upright, feet firm on ground, gentle breath through mouth, exhale gently Expansion breathing Comfortable upright position, knees slightly bent, place hands on each side just above waist Splinting use pillow or towel and place over surgical site, take 3 deep breaths and clear then cough to loosen secretions See chart 18-4 for more thorough instruction

20
DVT risk Obese >40 yrs old Have cancer
Immobile or decreased mobility Leg fracture or trauma History of DVT, PE, Varicose veins, or edema Use oral contraceptives Smoke Decreased cardiac output Get them antiembolism stockings

21
Anxiety reduction Distraction Promote rest Guided imagery

22
Gerontological Considerations
Go over instructions slower Have family present Co-existing disease increases risk Positioning

23
Intra op

24
Nursing diagnosis Risk for infection Impaired skin integrity
Altered body temperature Anxiety Injury related to positioning and other hazards

25
Members Surgeon heads surgical team Makes decisions related to surgical procedure May need assistant Surgical assistant (other doctor, surgical tech, resident, intern) May hold retractors, suction wound, cut tissue, suture, and dress wounds depending on scope of practice and under supervision of physician Anesthesia Anesthesiologist or Certified Registered Nurse Anesthestist Maintains airway Monitoring circulation/respiratory status Replace blood/fluid loss
 May hold retractors, suction wound, cut tissue, suture, and dress wounds depending on scope of practice and under supervision of physician. Anesthesia. Anesthesiologist or Certified Registered Nurse Anesthestist. Maintains airway. Monitoring circulation/respiratory status. Replace blood/fluid loss.")
26
OR nurses Holding area nurse Primary role is Circulating Nurse
Duties performed outside of sterile field Scrub Nurse Passes instruments, sponges in the sterile field Perform surgical scrub Very specialized role, most education is during orientation, not in nursing school.

27
Surgical Areas Operating Room Restricted area
Trend towards less invasive procedures (less scarring, quicker recovery, decreased length of hospitalization

28
Basic Guidelines for Surgical Asepsis
All materials in contact with the wound and within the sterile field must be sterile. Gowns are sterile in the front from chest to the level of the sterile field, and sleeves from 2 inches above the elbow to the cuff. Only the top of a draped table is considered sterile. Items are dispensed by strategically to maintain sterility. Movements of the surgical team are from sterile to sterile and from unsterile to sterile only.

29
Movement around the sterile field must not cause contamination of the field. At least a 1-foot distance from the sterile field must be maintained. Whenever a sterile barrier is breached, the area is considered contaminated. Every sterile field is constantly maintained and monitored. Items of doubtful sterility are considered unsterile. Sterile fields are prepared as close as possible to time of use.

31
Question true or false. To maintain surgical asepsis, the nurse knows that the sides and top of a draped table is considered sterile.

32
Answer False. Rationale: Sterile drapes are used to create a sterile field. Only the top surface of a draped table is considered sterile. During draping of a table or patient, the sterile drape is held well above the surface to be covered and is positioned from front to back.

33
Infection Anyone with open wound, cold, or any infection should not participate in surgery Jewelry should be minimal Hands of surgical staff are usually cultured every 3-6 months to determine possible nosocomial (hospital acquired) infections
 infections.")
35
Attire

36
Time out procedure Nurse asks pt to confirm procedure and is verified with consent form Patient verifies the right site and surgeon 2 patient identifiers Site mark “Time out” Name, procedure, site, document See pg. 612

37
Anesthesia

38
Anesthesia Def: induced state of partial or total loss of sensation, occurring with or without loss of consciousness. Purpose: block nerve impulse transmission, suppress reflexes, promote muscle relaxation, and sometimes achieve controlled level of unconsciousness Choice depends on: type and duration of procedure, area of body, safety issues, emergency, pain management after surgery, last meal or liquids or drugs

39
Types General—see slides Local- Novocaine for example Hypnosis
Cryothermia Acupuncture TABLE ON PAGES

40
General Definition: reversible loss of consciousness induced by inhibiting neuronal impulses in several areas of the central nervous system Depress CNS Results in analgesia (pain relief), amnesia (memory loss), and unconsciousness with loss of muscle tone and reflexes Used in head, neck, upper torso and abd surgeries
, amnesia (memory loss), and unconsciousness with loss of muscle tone and reflexes. Used in head, neck, upper torso and abd surgeries.")
41
Stages of general 1:sedation administered
Induction and LOC, decreased sensation Warmth, dizziness, noises exaggerated 2: excitement/delirium LOC and relaxation, regular breathing Pupils dilate, HR increases, may need to restrain pt Do not touch pt 3: operative anesthesia Muscle relaxation, depressed vitals Unconscious, maintained for hours 4:danger = Medullary Depression Depressed vs, respiratory failure Too much anesthesia, cyanosis Emergence: recovery from anesthesia

42
Types of general Inhalation: most controllable Fast acting
Passes through vaporizer Depresses CNS Ex: Nitrous Oxide

43
Induce and maintain anesthesia Anesthetics Opiods
IV: rapid and pleasant Induce and maintain anesthesia Anesthetics Opiods Etomidate Fentanyl Valium Morphine Versed Diprivan Reversal agent for opoids=Narcan (0.2mg) Reversal agent for Benzos = Romazicon(0.2mg)
 Reversal agent for Benzos = Romazicon(0.2mg)")
44
Muscle relaxants Affect skeletal muscle Administered before intubation
Assess with nerve stimulator Succinylcholine, Tracrium, Vecronium Reversal agent= Neostigmine (0.5-2mg

45
Balanced: minimal disturbance to function, used with elderly and high risk
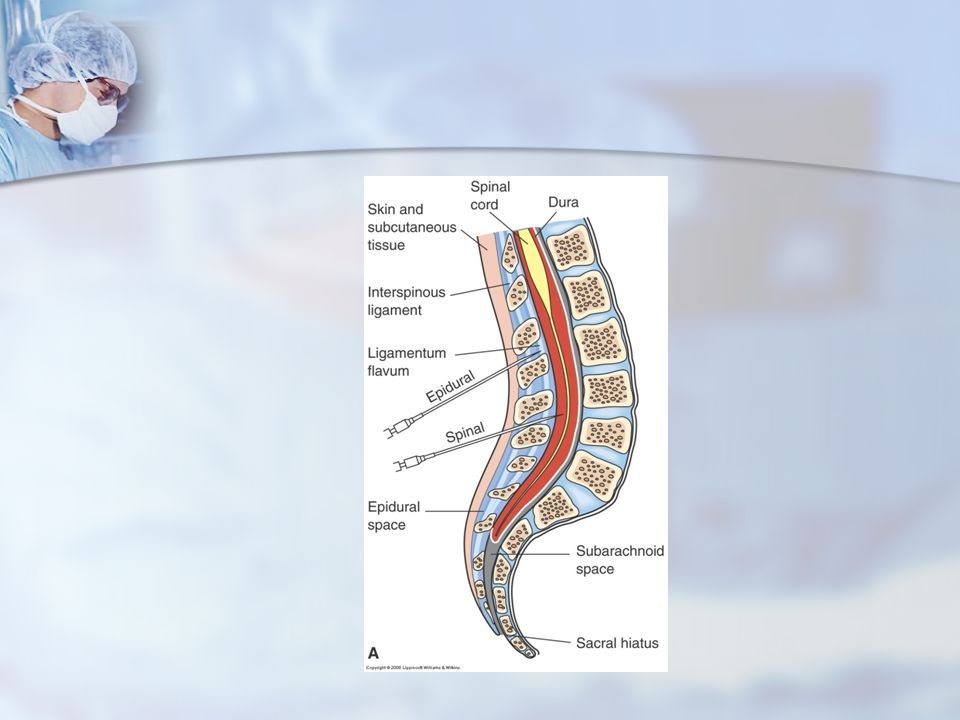
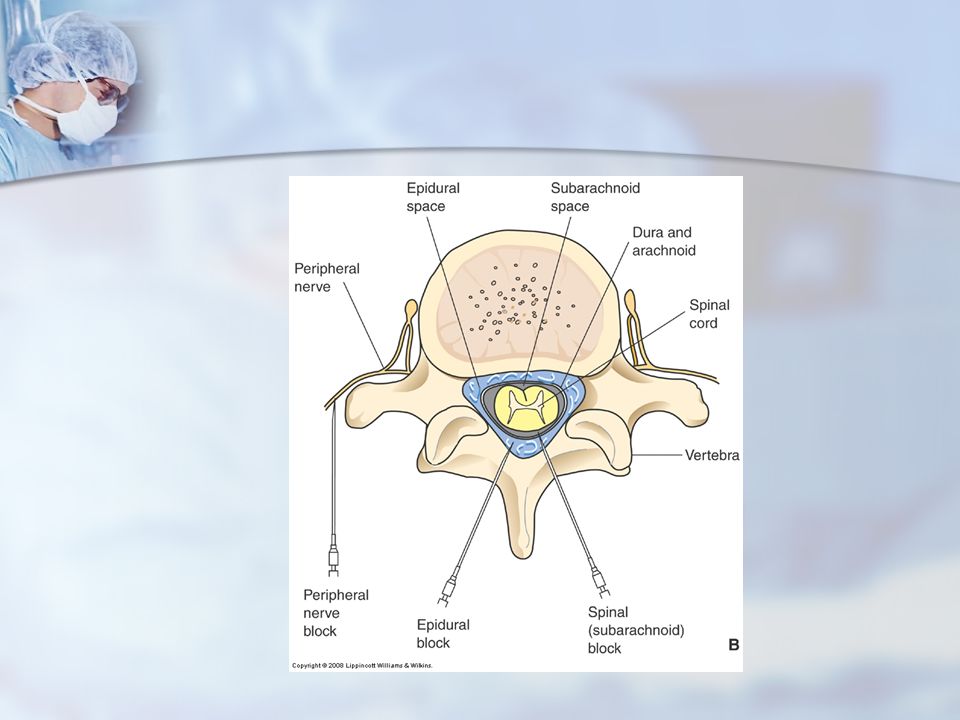
Regional (Spinal, Epidural, Peripheral nerve block)~ gag and cough stay intact block transmission of sensory impulses Does not depress respirations Local injection of med
~ gag and cough stay intact. block transmission of sensory impulses. Does not depress respirations. Local injection of med.")
46
Types of Regional Anesthesia
Spinal Local anesthetic injected into subarachoid space, directly into CSF “Blocks” at level of spinal cord (sensory and motor) Epidural Local anesthetic into epidural space Peripheral nerve block Anesthesia of a certain area No systemic effect
 Epidural. Local anesthetic into epidural space. Peripheral nerve block. Anesthesia of a certain area. No systemic effect.")
47
Complications of Regional
HA Hypotension Meningitis Hematoma at site Nerve damage

48
Intraoperative Complications
Nausea and vomiting Anaphylaxis Hypoxia and respiratory complications Hypothermia Dysrhymias Malignant hyperthermia Disseminated intravascular coagulation (DIC)
")
49
Malignant Hyperthermia
Life threatening Predisposition is genetic

50
causes increased calcium and potassium levels in skeletal muscles
Immediate reaction or several hours later s/s: tachycardia, dysrhythmias, muscle rigidity (jaw, face), hypotension, tachypnea, mottling, cyanosis, myoglobournia (muscle proteins in urine), *increase in CO2 and decrease sat Care: stop agent, intubate, give dantrium to reverse, check ABG, cooling techniques, monitor core temp, EKGs, insert foley, hydrate, ICU for at least 24 hours Chart 26-3
, hypotension, tachypnea, mottling, cyanosis, myoglobournia (muscle proteins in urine), *increase in CO2 and decrease sat. Care: stop agent, intubate, give dantrium to reverse, check ABG, cooling techniques, monitor core temp, EKGs, insert foley, hydrate, ICU for at least 24 hours. Chart")
51
Manifestations Hypoxia Hyperthermia****THIS IS A LATE SIGN****
Dysrhythmias Hypotension Early signs: contracture of jaw Sinus tach Increase in expiratory CO *Pg. 630 *

52
Complications continued
Overdose: can occur if metabolism and drug elimination are slower (ht, wt, and allergies are vital to know before administration) Unrecognized hypoventilation: failure to exchange gases can lead to cardiac arrest, permanent brain damage, and death. Vital to use end tidal carbon dioxide monitor to confirm the exchange
 Unrecognized hypoventilation: failure to exchange gases can lead to cardiac arrest, permanent brain damage, and death. Vital to use end tidal carbon dioxide monitor to confirm the exchange.")
53
Intubation complication
Broken or chipped teeth Swollen lip Vocal cord trauma

54
Question Malignant hyperthermia usually manifests within what time frame after induction of anesthesia? 5 minutes 10–20 minutes 30 minutes 45 minutes

55
Answer 10–20 minutes Rationale: Malignant hyperthermia usually manifests about 10 to 20 minutes after induction of anesthesia. It can also occur during the first 24 hours after surgery.

56
Local Numbing agent is used Mentally alert
Complications: potential cardiac depression, toxic reaction, edema, blurred vision, inflammation, etc. see

57
Types of local Topical Infiltration: directly into wound or lesion
Blocks: Field: injections around work site (lidocaine, novocaine) Nerve: injection into or around nerve in involved area-used for chronic pain relief Spinal: injection of agent into CSF in the subarachnoid space-absorbed rapidly Epidural: placed in epidural space-may affect breathing
 Nerve: injection into or around nerve in involved area-used for chronic pain relief. Spinal: injection of agent into CSF in the subarachnoid space-absorbed rapidly. Epidural: placed in epidural space-may affect breathing.")
60
Moderate (Conscious) Sedation
Minimally depressed LOC Pt able to maintain airway Pt responds to physical and verbal stimuli

61
Moderate (Conscious) Sedation
As a nurse, what do you need to have available at the bedside? What medications might be given? What monitoring/assessments? What types of procedures?

62
Potential Adverse Effects of Surgery and Anesthesia
Allergic reactions or drug toxicity Cardiac dysrhythmias Over sedation or Under sedation Trauma: laryngeal, oral, nerve, and skin, including burns Hypotension Thrombosis See Chart 19-1

63
Gerontologic Considerations
Elderly patients are at increased risk for complications because of: Pre-existing conditions. Aging heart and pulmonary systems. Decreased homeostatic mechanisms. Changes in responses to drugs because of changes such as decreased renal function, etc.

64
Nursing diagnosis Risk for injury r/t positioning
Impaired skin integrity r/t surgical incision Risk for infection

65
Important to remember Always know client’s wishes about life sustaining measures because they apply in the OR as well However some facilities/doctors require that the surgical client that is DNR on unit is full code in OR. Always know the allergies and reactions Always know current lab values because they could postpone surgery Know the client’ s baseline vitals to monitor for complications Patient identification Correct informed consent Verification of records of health history and exam Safety measures such as grounding of equipment, restraints, and not leaving a sedated patient Verification and accessibility of blood

66
Positioning Accommodates access Surgical view
Maintain skin integrity (pressure ulcers) Injury to nerves may happen Prevent injury Complications: Compromised respiratory status, pressure ulcers, injury to nerves
 Injury to nerves may happen. Prevent injury. Complications: Compromised respiratory status, pressure ulcers, injury to nerves.")
67
Surgical positions Supine Trendelenburg Prone Lateral Jackknife
lithotomy

68
Bariatrics Deals with causes, prevention, and treatment of obesity First line: diet, exercise, behavior therapy, & antiobesity drugs BUT HAS ONLY SHORT TERM SUCCESS IN MANY CASES

69
Antiobesity drugs: Orlistat (approved Feb ’07) - reduces absorption of fat by inhibiting pancreatic lipase Metformin Byetta (delays gastric emptying)
")
70
Bariatric Surgery Roux en Y: most commonly performed
- least likely to result in nutritional deficiencies - small bowel is divided & arranged into a “y” and attached to the small stomach pouch - pt feels fullness rapidly after eating

71
Post op Starts at the completion of surgery and transfer to PACU or ICU Stabilize VS, maintain airway Prepare pt for discharge To work here in-depth knowledge of the following areas needed: pharm, pain management, and procedures, good assessment skills, decision maker in critical situations

72
Assessment Cardio Telemetry, ekgs, vitals, pulses, homans, Neuro
LOC, motor response, orientation, arousal Fluid and electrolyte I/O, hydration, IVF, acid base Renal Output, urine retention is common if no foley Gi N/V, peristalsis, monitor for ileus, NG tube output if indicated Skin Monitor wound, drainage, drains, dressings, Vitals are vital Usually q15” x4, q30” x4, q1hr x4, q2hr x4, then q4hr Respiratory status Airway management, lung sounds, muscle use, snoring, stridor (high pitched crowing) Monitor PAIN
 Monitor PAIN.")
73
Early infection can be indicated on increase in band cells of the WBC differential (left shift)
Get culture Notify MD Monitor ABGs and CMP

75
Aldrete Post Anesthesia Recovery Score (PARS)
Numerical scoring system to eval PACU patients Based on activity, Respirations, Circulation, Consciousness, O2 Sats Ranges from 0 to 10, 10 is the best Score when arrives in PACU, every 30 min until 8 or higher is achieved Score also done at discharge

76
Nursing diagnosis

77
Impaired Gas Exchange Open airway
Breathing pattern improved over baseline Adequate O2 saturation Provide supplemental oxygen Artificial airway if patient is minimally responsive Cough deep breath, IS

78
Risk for Imbalanced Fluid Volume
Adequate hemostasis Normal fluid and electrolyte balance Monitor hourly for postop bleeding Mark drainage on dressing, monitor for enlargement Monitor for possible drainage beneath patient Monitor for internal bleeding Monitor for signs of dehydration, fluid overload

79
Risk for Decreased Cardiac Output
Rhythm, cardiac output BP, heart rate consistent with baseline Monitor for sinus tachycardia/bradycardia, identify and treat cause Monitor for hypotension; IV fluids, patient positioning Monitor for hypertension, identify and treat cause

80
Risk for Imbalanced Body Temperature: Hypothermia
Normal core temperature Monitor for core temperature <36°C (96.8°F), shivering, patient report of feeling cold Risk factors: patient history, length of surgery, cold solutions Blankets, clothing, ambient temp Treat with active warming, meds
, shivering, patient report of feeling cold. Risk factors: patient history, length of surgery, cold solutions. Blankets, clothing, ambient temp. Treat with active warming, meds.")
81
Pain Physiological and psychological effects
Delayed ambulation, diminished functioning Monitor for pain management and respiratory depression PCA, PCEA: monitor for pain relief, untoward effects Monitor sensory level of the epidural

82
Anxiety Can increase morbidity and mortality, length of stay
Affects VS, depresses immune system, delays healing Implicated in heart problems, postop pain Individualized care plan based on patient preferences Frequent reassurance about condition and progress Maintain a calm, quiet, restful environment

83
Drains see chart 27-6 Hemovac JP Penrose

84
Chest tube

85
Types of wound healing

86
Post-Op Complications
Evisceration Dehiscence SSI Atelectasis Pneumonia ileus Urinary retention DVT

87
Dehiscence Partial or complete separation of wound layers
Wound is open Prevention?

88
Evisceration Complete separation of wound layers
Protrusion of internal organs Usually occurs 5-10 days post-op Prevention?

89
Surgical Site Infections (SSI)
Aseptic technique Most infections are caused by exogenous organisms Surgical wound classification (pg. 636) Risks: Obesity, smokers, malnourishment
 Risks: Obesity, smokers, malnourishment.")
90
Dehiscence Evisceration Complications on chart 27-4

91
Atelectasis and Pneumonia
Collapse of alveoli Mucus accumulates Leads to fever and hypoxia Incidence of post op pneumonia 15% High fowlers IS, CDB Ambulate

92
Gastrointestinal N/V Flatus Bowel sounds
Ileus-hypoactive bowel, delay in peristalsis

93
Urinary Retention Foley cath Must void within 6-8hrs
Anesthesia causes relaxation, retention May have swelling from certain procedures

94
DVT LWM- Heparin or lovonox SCD TEDS Ambulation Leg exercises

Similar presentations