Download presentation
Presentation is loading. Please wait.

1
Cardiogenic shock Kasia Hryniewicz, M.D. Minneapolis Heart Institute, Abbott Northwestern Hospital, Minneapolis, MN Greater Twin Cities Area Chapter of AACN Fall Symposium November 8, 2013

2
Definition Cardiogenic shock (CS) is a clinical condition of inadequate tissue perfusion due to cardiac dysfunction.
 is a clinical condition of inadequate tissue perfusion due to cardiac dysfunction.")
3
Definition cont persistent hypotension (systolic blood pressure <80 to 90 mmHg or mean arterial pressure 30 mmHg lower than baseline) severe reduction in cardiac index (<1.8 L/ min per m2 without support or <2.0 to 2.2 L/ min per m2 with support) adequate or elevated filling pressures
 severe reduction in cardiac index (<1.8 L/ min per m2 without support or <2.0 to 2.2 L/ min per m2 with support) adequate or elevated filling pressures")
4
Etiology Cardiogenic shock Acute Chronic - End stage cardiomyopathy, inotrope dependent

5
Etiology – Acute CS 1.Acute myocardial infarction –Large infarct, reinfarction –Mechanical complications MR, VSD, free wall rupture –Right ventricular infarction 2. Non-infarct related - acute myocarditis - acute MR – chordal rupture/endcarditis - acute AI – dissection, endocarditis - stress induced cardiomyopathy - myocardial contusion

6
Incidence- SHOCK registry 1190 pts- overall incidence – 5% The majority of patients have a STEMI, but CS occurs in 2.5% (NSTEMI) LV failure79% Severe MR7% VSD4% Isolated RV infarct 2% Tamponade1.4% Other7%
 LV failure79% Severe MR7% VSD4% Isolated RV infarct 2% Tamponade1.4% Other7%")
7
Shock - pathophysiology Hochman J:Circulation 107:2998, 2003

8
Risk factors Older age Anterior MI Hypertension diabetes mellitus multivessel coronary artery disease Prior MI or diagnosis of heart failure STEMI Left bundle branch block on the electrocardiogram (ECG)
")
9
Risk factors continue In the GUSTO-I and GUSTO-III trials of fibrinolytic therapy in acute STEMI -Age -systolic blood pressure -heart rate -Killip class were major predictors of CS accounting for over 95 percent of the predictive information.

10
Killip acute HF class Class 1Absence of rales over the lung fields and absence of S3. Class 2Rales over 50% or less of the lung fields or the presence of an S3. Class 3Rales over more than 50% of the lung fields. Class 4Cardiogenic shock

11
Symptoms severe systemic hypotension signs of systemic hypoperfusion (eg, cool extremities, oliguria, and/or alteration in mental status) respiratory distress due to pulmonary congestion. Not all patients present with this syndrome. In particular, most patients develop shock after presentation.

12
Onset Based on GUSTO trials Shock was present on admission in 0.8 % at hospital presentation and an additional 5.3 % developed shock after admission, either as a sudden event or as a gradual fall in blood pressure. Approximately 50 percent of patients who developed shock after admission did so within the first 24 hours after the infarct. In SHOCK trial: the median time from MI to onset of cardiogenic shock was 5.5 hours and 75 % of patients developed shock within 24 hours.

13
Onset cont Shock developed significantly later among patients with a NSTEMI (median 76 to 94 hours versus 9.6 hours for those with STEMI).
.")
14
Pre-shock COMMIT trial randomization to early beta blockade was associated with a 30% higher occurrence of CS in patients: -> 70 years of age -SBP < 120 mm Hg -HR >110 beats per minute -Killip Class > 1 Commit trial.

15
Diagnosis is key! H&P ECG Echo (TTE/TEE) S-G catheter Coronary angiogram
 S-G catheter Coronary angiogram")
16
Treatment

18
Shock trial Inclusion criterion: shock due to LV failure complicating myocardial infarction 302 pts randomly assigned to emergency revascularization (n=152) or initial medical stabilization (n=150).
 or initial medical stabilization (n=150).")
19
Shock trial IABP was performed in 86 percent of the patients in both groups. The primary end point mortality from all causes at 30 days. Secondary end point six-month survival

20
Shock trial results - No difference in mortality at 30 days (46.7% vs 56%, p=0.11) - Significant decrease in all cause mortality at 6 months (50.3% vs. 63.1% p=0.027).
..")
21
Shock trial – what have we learned? 1. Average LV ejection fraction (EF) is only moderately severely depressed (30%), with a wide range of EFs and LV sizes noted. 2. SVR on vasopressors is not elevated 3. A clinically evident systemic inflammatory response syndrome is often present in patients with CS. 4. Most survivors have NYHA class I status.
 is only moderately severely depressed (30%), with a wide range of EFs and LV sizes noted. 2. SVR on vasopressors is not elevated 3. A clinically evident systemic inflammatory response syndrome is often present in patients with CS. 4. Most survivors have NYHA class I status..")
22
Predictors of outcome Coronary anatomy - Higher mortality in pts with a LM SVG lesion than in those with LCX, LAD or RCA (79 and 70 % vs 37and 42%). RCA culprit lesions were associated with the best prognosis Echocardiographic predictors - (LVEF) and severity of mitral regurgitation (MR). LVEF <28 percent survival at one year was 24% vs 56% Moderate or severe MR survival at one year was 31 % vs 58% However, there was benefit of early revascularization at all levels of LVEF and MR grade. Symptom onset to reperfusion time - mortality only 6.2 percent in patients reperfused within two hours of symptom onset
 and severity of mitral regurgitation (MR). LVEF <28 percent survival at one year was 24% vs 56% Moderate or severe MR survival at one year was 31 % vs 58% However, there was benefit of early revascularization at all levels of LVEF and MR grade. Symptom onset to reperfusion time - mortality only 6.2 percent in patients reperfused within two hours of symptom onset.")
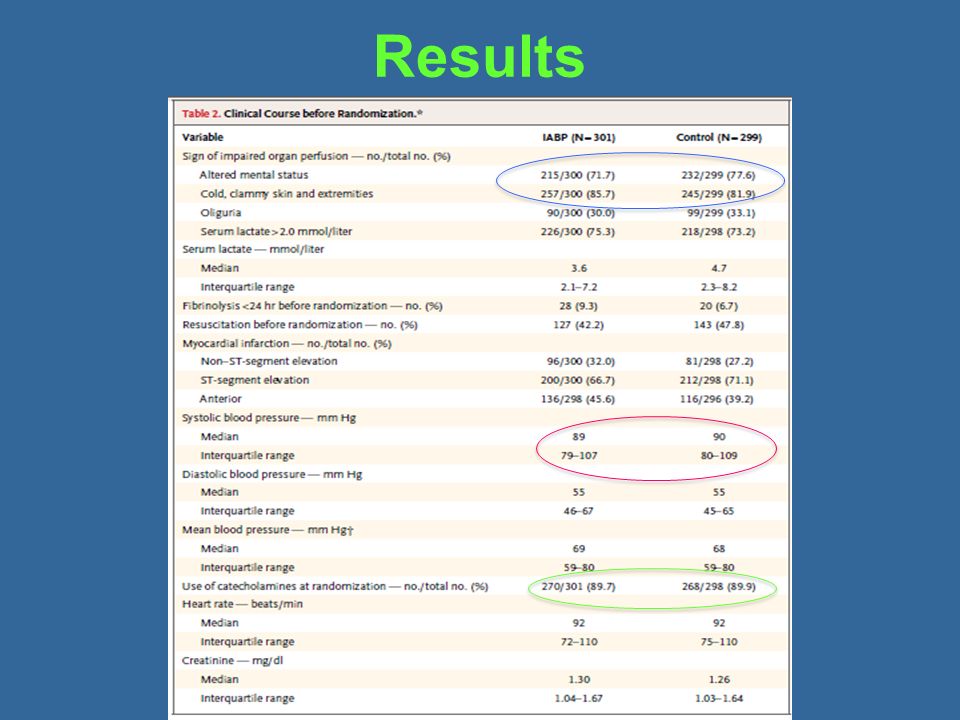
24
Methods Randomized, prospective, open-label, multicenter trial 600 patients with CS complicating acute myocardial infarction, randomly assigned to - IABP, (301 pts) or - no IABP (299 pts) plus early revascularization The primary end point 30-day all-cause mortality. Safety assessments - major bleeding, peripheral ischemic complications, sepsis, and stroke.

25
Results

27
At 30 days – 119 patients in the IABP group (39.7%) and 123 patients in the control group (41.3%) had died (P = 0.69). - At 6 months – no difference in mortality.

28
Conclusions… The use of IABP did not significantly reduce 30-day or 6 month mortality in patients with cardiogenic shock complicating acute MI for whom an early revascularization strategy was planned.

29
Conclusions… The IABP-SHOCK II trial could have affirmed contemporary clinical practice and guidelines,“ "Instead, it revealed surprising results.... We must now move forward with the understanding that a cardiovascular condition with 40% mortality at 30 days remains unacceptable

30
CS-Management General measures -ventilation support to correct hypoxemia and, in part, acidosis -Optimize intravascular volume -Sodium bicarbonate only for severe metabolic acidosis (arterial pH less than 7.10 to 7.15) -Aspirin -Intravenous heparin -insertion of pulmonary artery catheter
 -Aspirin -Intravenous heparin -insertion of pulmonary artery catheter")
31
Management cont Pharmacologic support -Vasopressors and inotropes (norepinephrine, vasopressin, dopamine, neosinephrine, dobutamine, milrinone) Mechanical support -IABP??? -Full mechanical support (ECMO?)
.")
32
Which pressor is best?

33
Results 1679 pts, 858 dopamine and 821 norepinephrine. Primary outcome – rate of death at 28 days Secondary endpoint – number of days without need for organ support and occurrence of adverse events.

34
Results 1. No difference in primary outcome (52.5% vs 48.5%) 2. Less AE in norepinephrine group (24.1% vs 12.4%, p<0.001) 3. In CS subgroup analysis Dopamine was associated with significantly higher mortality comparing with norepinephrine.
 3. In CS subgroup analysis Dopamine was associated with significantly higher mortality comparing with norepinephrine..")
35
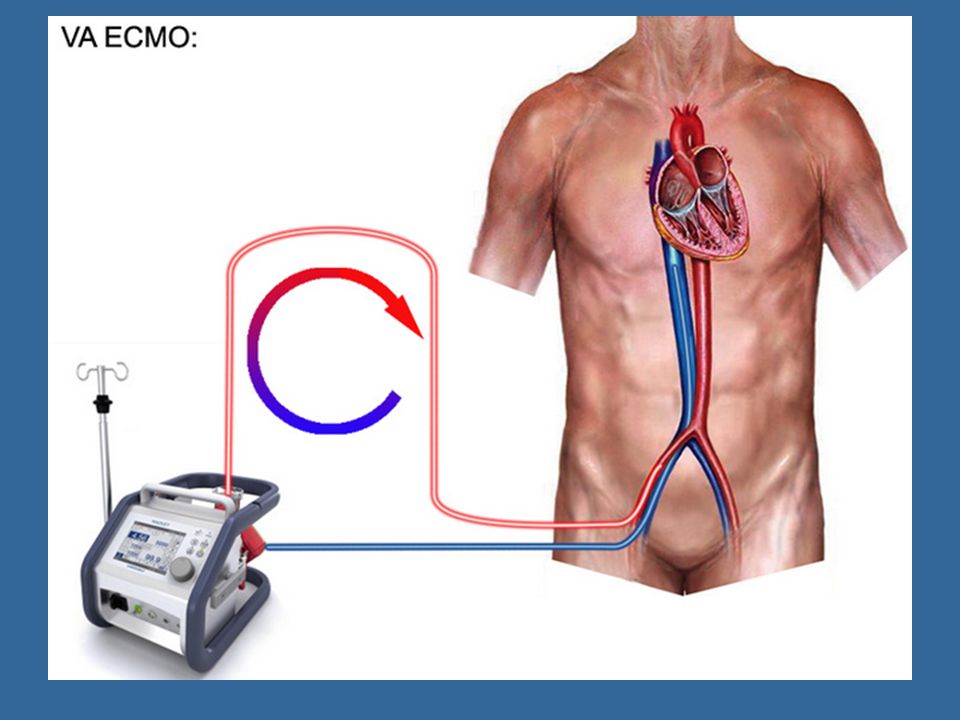
What about mechanical support?

36
ExtraCorporeal Membrane Oxygenation VV (veno-venous) respiratory failure VA (veno-arterial) full hemodynamic support for refractory cardiogenic shock Relatively easy placement Temporary stabilization, bridge to recovery/permanent VAD Requires anticoagulation
 respiratory failure VA (veno-arterial) full hemodynamic support for refractory cardiogenic shock Relatively easy placement Temporary stabilization, bridge to recovery/permanent VAD Requires anticoagulation")
38
ECMO at ANWH 46 pts between 2012-2013 Percutanously placed in the cath lab Survival to discharge 70% Major complications – bleeding Patients managed by HF cardiologists/RNs/perfusionists in CT ICU

39
Approach to a pt with CS Acute MI Mechanical complications Surgery H&P, ECG, echo (TEE) Cath lab Revascularization IABP?/MCS (ECMO)? Severely depressed EF, STE PCI MCS (ECMO?)
.")
40
Thank you!

Similar presentations



















>")






