Download presentation
Presentation is loading. Please wait.

1
PALLIATIVE SEDATION Myth, Mercy or Euphemism?
Nova Scotia Hospice Palliative Care Association Annual Conference 2011 PALLIATIVE SEDATION Myth, Mercy or Euphemism? Dr Nigel Sykes St Christopher's Hospice London

2
A Confusion of Terms Terms: Palliative sedation Terminal sedation
Early terminal sedation Palliative sedation therapy Primary sedation Secondary sedation Proportionate sedation Controlled sedation for intractable distress in the dying Sudden sedation Continuous deep sedation

3
This yields 4,782,969 possible definitions of Palliative Sedation…
A Manifold Definition of Palliative Sedation (Adapted from Jones, 2011) Palliative Sedation is the use of sedatives that is either continuous or intermittent; deep or mild; the primary or secondary pharmacological effect; proportionate or disproportionate to ‘refractory symptoms’ ; which include or do not include ‘existential distress’; in a patient who is or is not imminently dying; at the request or not of the patient; who intends or does not intend to be unconscious until death; with the doctor also intending this or not; withholding or not withholding nutrition and hydration; with or without an advance refusal; such that this protocol does or does not actually hasten death; and is intended or is not intended to do so by the patient; and is intended or is not intended to do so by the patient This yields 4,782,969 possible definitions of Palliative Sedation…
 Palliative Sedation is the use of sedatives that is either continuous or intermittent; deep or mild; the primary or secondary pharmacological effect; proportionate or disproportionate to ‘refractory symptoms’ ; which include or do not include ‘existential distress’; in a patient who is or is not imminently dying; at the request or not of the patient; who intends or does not intend to be unconscious until death; with the doctor also intending this or not; withholding or not withholding nutrition and hydration; with or without an advance refusal; such that this protocol does or does not actually hasten death; and is intended or is not intended to do so by the patient; and is intended or is not intended to do so by the patient. This yields 4,782,969 possible definitions of Palliative Sedation…")
4
Is the likely clinical effect of this Definition…
Palliative Sedation is the use of sedatives that is intermittent; mild; proportionate to ‘refractory symptoms’ ; in a patient who is imminently dying; not withholding nutrition and hydration

5
…the same as the likely clinical effect of this Definition?
Palliative Sedation is the use of sedatives that is continuous, deep, disproportionate to ‘refractory symptoms’ ; in a patient who is not imminently dying but is intended to be unconscious until death; withholding nutrition and hydration A Euphemism for Euthanasia?

6
A Confusion of Purposes
Sedation can mean: The giving of sedatives for specific symptom control, e.g. Seizures Delirium in the absence of correctable factors A treatment for insomnia The attempt to make a patient unaware of a intractable symptom by reducing their conscious level An expert survey achieved only 40% agreement with a single definition of sedation (Chater, 1998) Chater S et al. Pall Med, 1998; 12: The definition was the intention of deliberately inducing and maintaining deep sleep, but not deliberately causing death for intractable symptoms or profound anguish in patients perceived to be close to death. (Autgors from Ottawa)
 Chater S et al. Pall Med, 1998; 12: The definition was the intention of deliberately inducing and maintaining deep sleep, but not deliberately causing death for intractable symptoms or profound anguish in patients perceived to be close to death. (Autgors from Ottawa)")
7
What is an intractable symptom?
An "intractable" symptom is one: that does not respond to available treatment or for which the treatment is unacceptable to the patient because of: insufficiently rapid action or excessive side effects (Cherny and Portenoy, 1994) Sedation is used significantly more often by doctors who predict that a symptom will be intractable than by those who actually try all the treatments (Morita, 2004) Cherny NI, Portenoy RK. Sedation in the management of refractory symptoms: guidelines for evaluation and treatment. J Pall Care, 1994; 10(2): Frequency of intractable symptoms controversial: this paper estimates 16-52%. Morita T. Differences in physician-reported practice in palliative sedation therapy. Supp Care cancer, 2004; 12:
 Sedation is used significantly more often by doctors who predict that a symptom will be intractable than by those who actually try all the treatments (Morita, 2004) Cherny NI, Portenoy RK. Sedation in the management of refractory symptoms: guidelines for evaluation and treatment. J Pall Care, 1994; 10(2): Frequency of intractable symptoms controversial: this paper estimates 16-52%. Morita T. Differences in physician-reported practice in palliative sedation therapy. Supp Care cancer, 2004; 12:")
8
Reasons for sedation Multicentre study of 387 terminally ill patients
Haemorrhage % Distress % Pain % Nausea and vomiting 2.3% Breathlessness % Delirium % (Fainsinger et al., 2000)
")
9
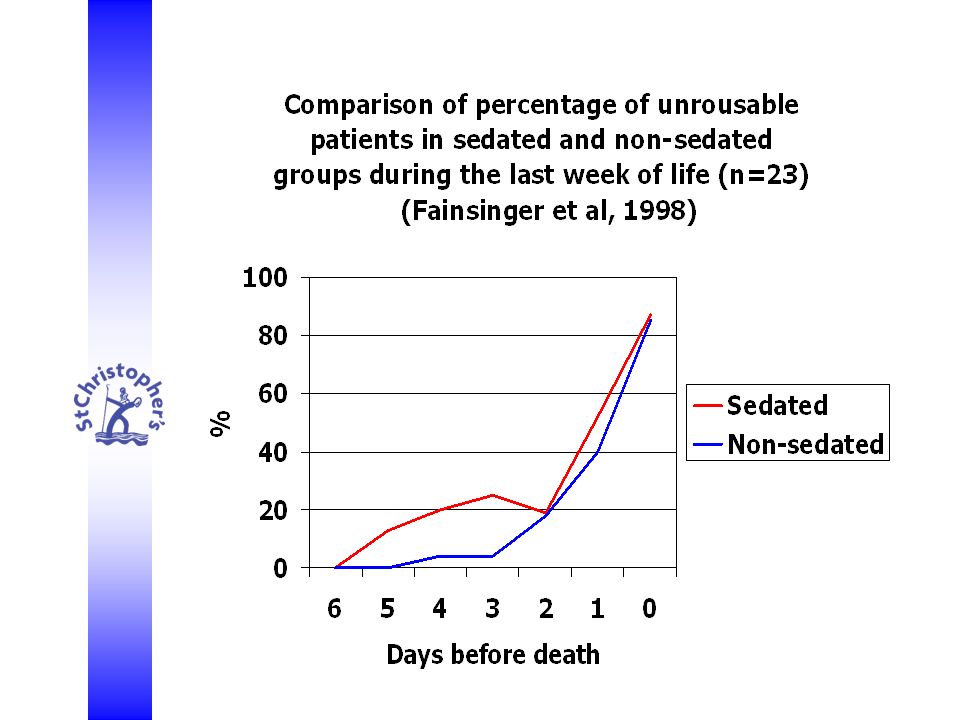
How often is sedation used in Palliative Care?
Reports of the proportion of patients who require sedation in the closing days of life vary widely: 1% (Fainsinger, 1998) 88% (Turner et al., 1996) This situation is not getting any better: Prospective study of the use of all depths and lengths of sedation in eight palliative care units showed a rate of 7.5% (Claessens et al, 2011) Retrospective study from one palliative care unit of the use specifically of continuous deep sedation showed a rate of 43% (Rietjens et al., 2008) Turner K, Chye R, Aggarwal G, Philip J, Skeels A and Lickiss J.N. Dignity in dying: A preliminary study of patients in the last three days of life. J Pall Care, 1996; 12(2): 7-13. Fainsinger RL. Use of sedation by a hospital palliative care support team. J Pall Care, 1998; 14(1):
 88% (Turner et al., 1996) This situation is not getting any better: Prospective study of the use of all depths and lengths of sedation in eight palliative care units showed a rate of 7.5% (Claessens et al, 2011) Retrospective study from one palliative care unit of the use specifically of continuous deep sedation showed a rate of 43% (Rietjens et al., 2008) Turner K, Chye R, Aggarwal G, Philip J, Skeels A and Lickiss J.N. Dignity in dying: A preliminary study of patients in the last three days of life. J Pall Care, 1996; 12(2): Fainsinger RL. Use of sedation by a hospital palliative care support team. J Pall Care, 1998; 14(1):")
10
Sedation in Palliative Care
The use of sedative drugs has always been a part of Palliative Care at the end of life: For mental distress (but only as an adjunct to the giving of properly attentive time) (Saunders, 1960) For anxiety or agitated confusion (Saunders, 1965) Opiates should not be used as sedatives (Saunders, 1958) “It should hardly ever be necessary to use the very heavy sedation that completely smothers the patient’s personality, although many who see these patients only occasionally do not believe that it is possible to avoid this” (Saunders, 1967) p.102 in Clark. CS Selected Writings
 (Saunders, 1960) For anxiety or agitated confusion (Saunders, 1965) Opiates should not be used as sedatives (Saunders, 1958) It should hardly ever be necessary to use the very heavy sedation that completely smothers the patient’s personality, although many who see these patients only occasionally do not believe that it is possible to avoid this (Saunders, 1967) p.102 in Clark. CS Selected Writings.")
11
Sedatives can do both these things
“Very heavy sedation that completely smothers the patient’s personality” The crux of ethical and clinical concern seems to be whether sedative use: Obliterates the patient’s personality and destroys the possibility of further emotional and spiritual development Kills the patient Sedatives can do both these things

12
Sedation for intractable symptoms
The paramount moral obligation is to relieve suffering “A doctor who leaves a patient to suffer intolerably is morally more reprehensible than the doctor who performs euthanasia” Twycross, 1996 Mercy Twycross RG. Euthanasia: going Dutch? J Roy Soc Med, 1996; 89:

13
Principle of Double Effect (The Get-out Clause)
A harmful effect of treatment, even resulting in death, is permissible providing that it: was not intended and arises as a side effect of a beneficial action and the harmful effect was not the means of achieving the beneficial effect But if we need to invoke the Principle of Double Effect does this suggest we are routinely shortening patients’ lives by sedation? Truth or Myth?

14
Classification of end of life care sedation (Broeckaert, 2000)
Mild Intermittent Acute Deep Continuous Non-acute

15
Classification of end of life care sedation (Morita, Tsuneto and Shima, 2001)
Mild Intermittent Primary Pain No organ failure Deep Continuous Secondary Psychological distress Organ failure Morita T, Tsuneto S, Shima Y. Proposed definition for sedation. Lancet 2001; 338:

16
How is depth of sedation assessed?
Glasgow Coma Scale (Teasdale and Jennett, 1974) Communication Capacity Scale (Morita et al., 2001) Consciousness Scale for Palliative Care (Goncalves et al.,2008) Physicians’ unsubstantiated report Assessment of the deepest sedation requires infliction of pain: Supra-orbital pressure (GCS) Pain (unspecified method) or change in position (CCS) Trapezius pinch (CSPC) How willing are palliative care staff to carry out these assessments routinely?
 Communication Capacity Scale (Morita et al., 2001) Consciousness Scale for Palliative Care. (Goncalves et al.,2008) Physicians’ unsubstantiated report. Assessment of the deepest sedation requires infliction of pain: Supra-orbital pressure (GCS) Pain (unspecified method) or change in position (CCS) Trapezius pinch (CSPC) How willing are palliative care staff to carry out these assessments routinely")
17
Depth of Sedation It has been suggested that the depth of sedation tends to increase as death approaches 45% of patients originally given ‘mild’ sedation had ‘deep continuous’ sedation by two days before death (Claessens et al., 2011) But this is based on only 9 patients and it is not clear how the sedative doses changed in the interim How different is this from the natural trajectory of dying? 50% of Palliative Care not receiving sedatives are unable to manage complex communication five days before death (Morita et al., 2003)
 But this is based on only 9 patients and it is not clear how the sedative doses changed in the interim. How different is this from the natural trajectory of dying 50% of Palliative Care not receiving sedatives are unable to manage complex communication five days before death (Morita et al., 2003)")
19
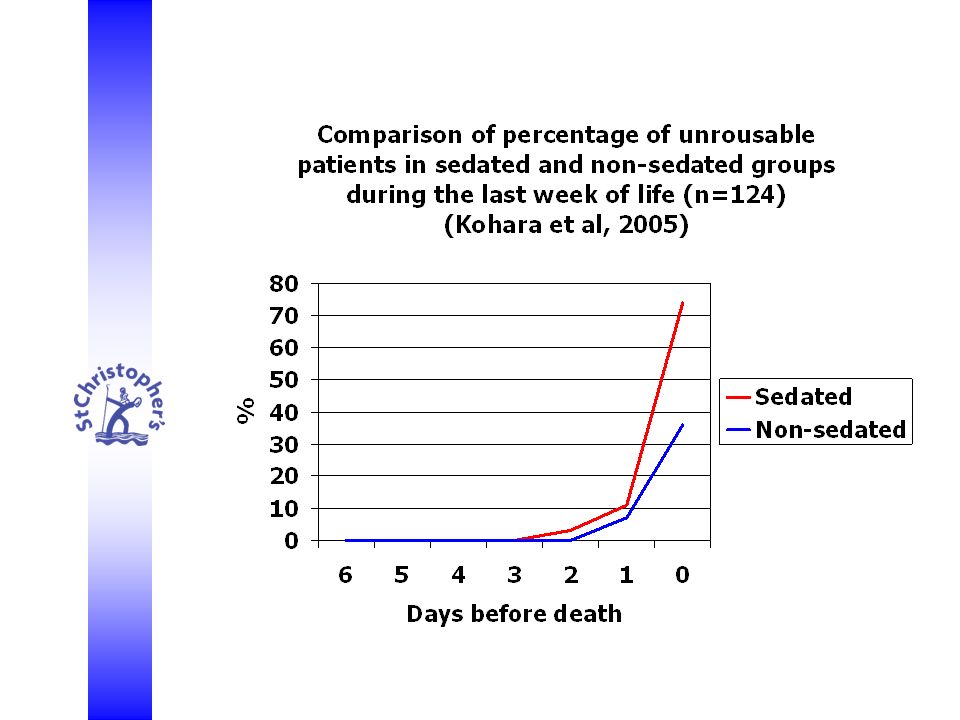
Kohara H, Ueoka H, Takeyama H, Murakami T, Morita T
Kohara H, Ueoka H, Takeyama H, Murakami T, Morita T. Sedation for terminally ill patients with cancer with uncontrollable physical distress. J Pall Med, 2005; 8(1):
:")
22
What is in the Name? The root of the word sedation is the Latin sedatio meaning ‘soothing’ or ‘allaying’ The clinical purpose of sedative drugs in palliation is the reduction of irritability or agitation, i.e. the relief of distress Sleep is not the intention but may occur either: if a high enough sedative dose is required to relieve the distress or If a tired, ill patient is enabled to be comfortable and relaxed Soporare = to render sleepy

23
Continuousness Sedation is a response to a symptom
Continuous symptoms need continuous relief See use of regular morphine in chronic pain for details 30% of patients receiving sedatives do so only on an ‘as required’ basis Median 2.5mg midazolam on a median of 2 occasions (Dunn et al., 2008) Liverpool Care Pathway Guidance suggests use of a continuous subcutaneous infusion if two or more ‘as required’ doses of sedative have been given in 24h (NCPC, 2006) So ‘as required’ rapidly becomes ‘continuous’ Continuous sedative administration is neither rare nor necessarily sinister
 Liverpool Care Pathway Guidance suggests use of a continuous subcutaneous infusion if two or more ‘as required’ doses of sedative have been given in 24h (NCPC, 2006) So ‘as required’ rapidly becomes ‘continuous’ Continuous sedative administration is neither rare nor necessarily sinister.")
24
Proportionality There is a growing consensus that the essence of sedative use in Palliative Care is proportionality Morita, Tsuneto and Shima, 2002 De Graeff and Dean, 2007 Brockaert and Claessens, 2009 Cherny and Radbruch, 2009 Hasselaar, Verhagen and Vissers, 2009 Quill et al., 2009 But not everywhere. The Dutch National Guideline on Palliative Sedation speaks of proportionality but assumes: The aim is to reduce consciousness The patient should be within 2 weeks of dying Administration of fluids should be stopped A doctor should be present at initiation of sedation (KNMG 2005/2009)
")
25
Proportionate Responses are key to Palliative Care Practice
The mode of use of sedatives is analogous to that of other symptom control measures, such as opioids for pain: A low initial dose is titrated higher against the response until distress is relieved, i.e. the dose used is proportional to severity of distress Relief of distress is the end-point, not a particular level of consciousness

26
What is a Proportionate Dose of Sedative?
Midazolam is the most commonly used sedative in Palliative Care (Sykes and Thorns, 2003a) Mean midazolam doses reported range from 22 to 70mg/24h (Mercadante et al., 2009) But individually as high as 240mg/24h In our study of 238 patients: Overall mean midazolam dose was 25.7 mg/24 h Mean midazolam dose for patients receiving sedation throughout the last week of life was 54.5 mg/24 h (Sykes and Thorns, 2003b)
 Mean midazolam doses reported range from 22 to 70mg/24h (Mercadante et al., 2009) But individually as high as 240mg/24h. In our study of 238 patients: Overall mean midazolam dose was 25.7 mg/24 h. Mean midazolam dose for patients receiving sedation throughout the last week of life. was 54.5 mg/24 h (Sykes and Thorns, 2003b)")
27
Effect of Sedation on Palliative Care patients’ Survival
Study With sedation Without sedation Stone, 1997 (UK) 18.6 days 19.1 days Ventafridda, 1990 (Italy) 25 days 23 days Chiu, 2001 (Taiwan) 28.5 days 24.7 days Sykes, 2003b 38.6 days 14.2 days Kohara, 2005 (Japan) 28.9 days 39.5 days
 18.6 days days. Ventafridda, 1990 (Italy) 25 days. 23 days. Chiu, (Taiwan) 28.5 days days. Sykes, 2003b days days. Kohara, (Japan) 28.9 days days.")
28
Duration of Sedation Mean duration of sedation estimated to be 2.5 days (range ) Based on ten studies, totalling 1,900 patients (Porta Sales, 2001 updated) Suggests that sedation is generally a response to symptoms associated with the onset of dying Additional confirmation from: Chiu TY, Hu WY, Lue BH, Cheng SY, Chen CY. Sedation for refractory symptoms of terminal cancer patients in Taiwan. J Pain Symptom Management, 2001: 21: 70/251 (27.9%) terminal cancer patients required sedation (57% of them for delirium, 23% for dyspnoea, 10% for pain). Survival of sedated patients was 28.5 days, non-sedated 24.7 days (p=0.43).
 Suggests that sedation is generally a response to symptoms associated with the onset of dying. Additional confirmation from: Chiu TY, Hu WY, Lue BH, Cheng SY, Chen CY. Sedation for refractory symptoms of terminal cancer patients in Taiwan. J Pain Symptom Management, 2001: 21: /251 (27.9%) terminal cancer patients required sedation (57% of them for delirium, 23% for dyspnoea, 10% for pain). Survival of sedated patients was 28.5 days, non-sedated 24.7 days (p=0.43).")
29
Midazolam use at St Christopher’s
In a random recent month: 55 patients died 51 (93%) had at least one dose 35 (64%) had a continuous s.c. infusion 14 (40%) of infusions started within 48h of death 14 (40%) of infusions started 3 to 7 days before death All had either already stopped eating or ate until 3 to 5 days before death 7 (20%) infusions lasted between one week and one month Of these patients five continued to eat until 3 to 5 days before death The other two had gastrostomy feeding Was our sedation rate 93% or zero?
 had at least one dose. 35 (64%) had a continuous s.c. infusion. 14 (40%) of infusions started within 48h of death. 14 (40%) of infusions started 3 to 7 days before death. All had either already stopped eating or ate until 3 to 5 days before death. 7 (20%) infusions lasted between one week and one month. Of these patients five continued to eat until 3 to 5 days before death. The other two had gastrostomy feeding. Was our sedation rate 93% or zero")
30
58 year old man with astrocytoma
Case History 1 58 year old man with astrocytoma General condition noted to be deteriorating Developed an acute onset of violent agitation and paranoia Midazolam 20mg given i.m. stat followed by 55mg/24h by s.c. infusion Died 55 hours later

31
Case History 2 70 year old woman with lung cancer and a previous history of schizophrenia Admitted because of general deterioration Developed delusions and progressive agitation unresponsive to haloperidol doses up to 12mg per day Over 24h she received 125 mg levomepromazine and 60 mg midazolam by s.c. infusion, but also another 60 mg midazolam and 200 mg levomepromazine in s.c stat doses for continuing agitation At the end of this period her breathing was noted to be noisy. 200 mg phenobarbital was given s.c. and the patient died 6 h later.

32
And yet some will ask: Is sedation used to cover up potentially remediable delirium? 73% of delirium in palliative care is irreversible Life expectancy of patients with irreversible delirium is under 17 days (Leonard et al., 2008) What about provision of hydration and nutrition? This is a separate decision, but the great majority of patients who receive sedatives already have minimal oral intake What about sedation for existential distress? Does not correlate with physical deterioration
 What about provision of hydration and nutrition This is a separate decision, but the great majority of patients who receive sedatives already have minimal oral intake. What about sedation for existential distress Does not correlate with physical deterioration.")
33
Use of sedatives in existential or psychological distress
Hard to tell if such distress is really intractable Level of distress can be variable and idiosyncratic Standard treatments have low morbidity Intractability can only be decided by a multiprofessional clinical team skilled in psychological care who know both patient and family and have made repeated assessments Team access to psychiatry, chaplaincy and ethics is required (Cherny and Radbruch, 2009) Some sedative use may be helpful, as may respite sedation to provide periods of ‘time out’ But the induction of sleep for extended periods should be a truly exceptional occurrence
 Some sedative use may be helpful, as may respite sedation to provide periods of ‘time out’ But the induction of sleep for extended periods should be a truly exceptional occurrence.")
34
Conclusions ‘Sedation’ continues to mean different things to different people In specialist palliative care units use of sedatives in the last days of life is not associated with shortened survival overall Most use of sedatives is for the management of restlessness and confusion occurring as part of the process of dying Impaired consciousness is common at the end of life with or without sedatives The aim of sedative use is to relieve distress, not to induce sleep The key to ethical use of sedatives is proportionality, whatever the indication

35
If Palliative Sedation is approached properly…
It will be an act of Mercy for our patients whose distress cannot be relieved by other means It will be a Myth that it shortens patients’ lives And so It will not be a Euphemism for Euthanasia

Similar presentations









; MA.>")










