Download presentation
Presentation is loading. Please wait.

2
2011 and Beyond-Quo Vadis James P. Borgstede, M.D., FACR President-Elect ABR of the futureABR of the future ABMS of the futureABMS of the future Integration of ABR within healthcare and healthcare regulatory bodiesIntegration of ABR within healthcare and healthcare regulatory bodies

3
Thanks Gary Becker and ABR staffGary Becker and ABR staff David LaszakovitsDavid Laszakovits Jennifer BosmaJennifer Bosma

5
The ABR of the Future Increased demands to demonstrate relevance of certificationIncreased demands to demonstrate relevance of certification Increasing expectations of accountability to our diplomatesIncreasing expectations of accountability to our diplomates –ABR has established advisory committees Increased demands from a more robust American Board of Medical Specialties (ABMS)Increased demands from a more robust American Board of Medical Specialties (ABMS)
Increased demands from a more robust American Board of Medical Specialties (ABMS)")
6
ABMS of the Future More robustMore robust More legislatively activeMore legislatively active Continuous MOC rather than 10 year cyclesContinuous MOC rather than 10 year cycles Involvement and promotion of institutional MOCInvolvement and promotion of institutional MOC Significant presence of primary care boards in ABMS governanceSignificant presence of primary care boards in ABMS governance Competition from rogue organizations for statureCompetition from rogue organizations for stature

7
Integration of the ABR within healthcare and healthcare regulatory bodies

8
Movement away from concerns for access Movement away from payment for service and toward payment for quality Quality = value X price/ time How does this transformation from payment for service to payment for quality occur? Potentially thru Accountable Care Organizations (ACO)? An integration of traditional specialty societal economic efforts, e.g. ACR, with future expectations on ABMS member boards, e.g. ABR, as objective verifiers of quality. Healthcare continues to increase as percentage of GDP and all payers are looking for ways to save money Movement toward improvement in quality, decreasing costs, improving delivery
. An integration of traditional specialty societal economic efforts, e.g. ACR, with future expectations on ABMS member boards, e.g. ABR, as objective verifiers of quality. Healthcare continues to increase as percentage of GDP and all payers are looking for ways to save money Movement toward improvement in quality, decreasing costs, improving delivery.")
9
Socioeconomic Truisms Primary Care is KingPrimary Care is King Quality is the coin of the realm (to some)Quality is the coin of the realm (to some) However, quality is a shill to some payers and some in the government.However, quality is a shill to some payers and some in the government. Shill-definition: Somebody (payer) who promotes somebody else (quality) or makes a sales pitch (financial incentive to physicians) for something (better care) for reasons of self-interest (payer saves money).Shill-definition: Somebody (payer) who promotes somebody else (quality) or makes a sales pitch (financial incentive to physicians) for something (better care) for reasons of self-interest (payer saves money). –Encarta Dictionary North America There is a fusion of medical economics, quality, safety, and reimbursement which may or may not improve patient care.There is a fusion of medical economics, quality, safety, and reimbursement which may or may not improve patient care.
 who promotes somebody else (quality) or makes a sales pitch (financial incentive to physicians) for something (better care) for reasons of self-interest (payer saves money).Shill-definition: Somebody (payer) who promotes somebody else (quality) or makes a sales pitch (financial incentive to physicians) for something (better care) for reasons of self-interest (payer saves money). –Encarta Dictionary North America There is a fusion of medical economics, quality, safety, and reimbursement which may or may not improve patient care.There is a fusion of medical economics, quality, safety, and reimbursement which may or may not improve patient care..")
10
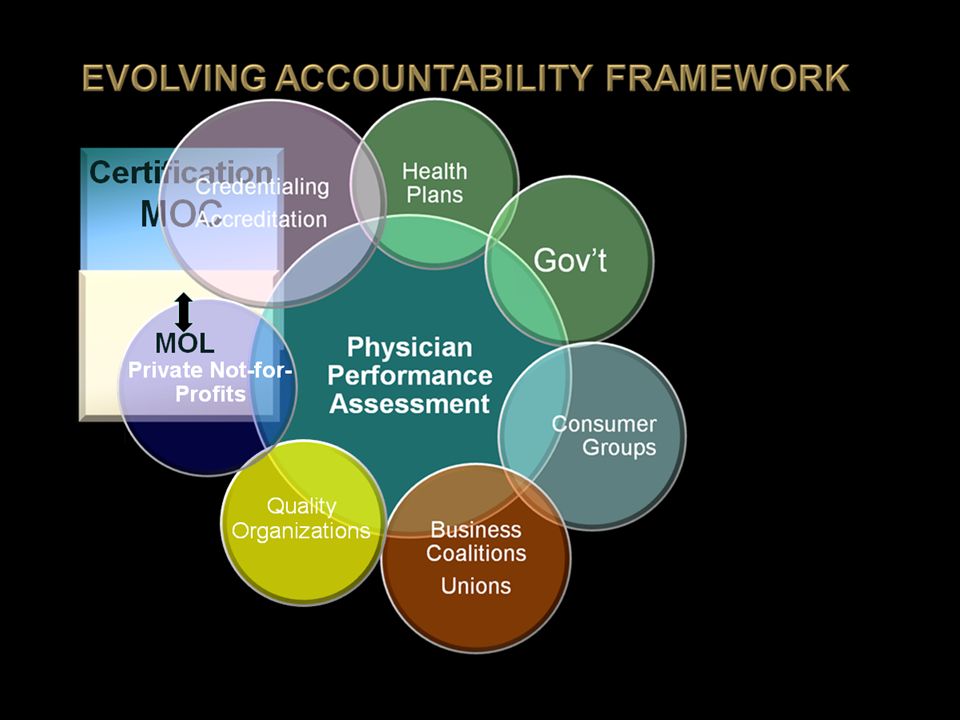
Certification MOC State Medical Licensure Physician Performance Assessment Health Plans Gov’t Consumer Groups Business Coalitions Unions Credentialing Accreditation Quality Organizations Private Not-for- Profits

11
Certification MOC Physician Performance Assessment Health Plans Gov’t Consumer Groups Business Coalitions Unions Credentialing Accreditation Quality Organizations Private Not-for- Profits MOL

12
An Example

13
Participation in the Center for Medicare and Medicaid Services (CMS) Physician Quality Reporting Initiative (PQRS) The Maintenance of Certification Program (MOCP) operated by an ABMS specialty body for CMS The ABMS Maintenance of Certification (MOC) program requiring practice quality improvement (PQI) These are three separate programs: – –PQRS (CMS $ 1% in 2011) – –If PQRS then opportunity to participate in MOCP (CMS $ 0.5%) – –PQI as part of ABR MOC separate from $$
 Physician Quality Reporting Initiative (PQRS) The Maintenance of Certification Program (MOCP) operated by an ABMS specialty body for CMS The ABMS Maintenance of Certification (MOC) program requiring practice quality improvement (PQI) These are three separate programs: – –PQRS (CMS $ 1% in 2011) – –If PQRS then opportunity to participate in MOCP (CMS $ 0.5%) – –PQI as part of ABR MOC separate from $$")
14
Voluntary program began in 2007Voluntary program began in 2007 Receive bonus payments of 1% (previously 1.5 percent) of their total allowed Medicare charges by satisfactorily submitting quality information for services they furnish in the calendar year.Receive bonus payments of 1% (previously 1.5 percent) of their total allowed Medicare charges by satisfactorily submitting quality information for services they furnish in the calendar year. 17 % of clinicians & 16 % of radiologists that could participate in PQRS reporting did so in 2009.17 % of clinicians & 16 % of radiologists that could participate in PQRS reporting did so in 2009. CMS failed to reimburse the promised 1% in many cases. The Physician Quality Reporting Initiative (PQRS)
.")
15
Physician Consortium on Performance Improvement (PCPI). AMA sponsored.Physician Consortium on Performance Improvement (PCPI). AMA sponsored. –The PCPI is a physician-led measure developer. –They do not implement their measures but make them available for use by any payer or organization that wishes to use them, e.g. CMS primarily. Other payers have also used PCPI measures. –Most of the measures in the current PQRS program were developed through the PCPI. –PCPI is now working with ABMS and specialty boards/societies to develop measures that can be used for PQI projects to meet MOC be used for PQI projects to meet MOC requirements in general and to help meet the requirements in general and to help meet the PQRS MOCP requirements. PQRS MOCP requirements.
. AMA sponsored. –The PCPI is a physician-led measure developer. –They do not implement their measures but make them available for use by any payer or organization that wishes to use them, e.g. CMS primarily. Other payers have also used PCPI measures. –Most of the measures in the current PQRS program were developed through the PCPI. –PCPI is now working with ABMS and specialty boards/societies to develop measures that can be used for PQI projects to meet MOC be used for PQI projects to meet MOC requirements in general and to help meet the requirements in general and to help meet the PQRS MOCP requirements. PQRS MOCP requirements..")
16
The Secretary of HHS will establish a composite of appropriate, risk-based measures of quality that reflect the health outcomes and health status of Medicare beneficiaries.The Secretary of HHS will establish a composite of appropriate, risk-based measures of quality that reflect the health outcomes and health status of Medicare beneficiaries. The Secretary of HHS must seek endorsement of the quality measures by the entity with a contract with the Secretary under section 1890(a) [e.g., the National Quality Forum].The Secretary of HHS must seek endorsement of the quality measures by the entity with a contract with the Secretary under section 1890(a) [e.g., the National Quality Forum]. The Physician Consortium on Performance Improvement (PCPI) seeks to develop the measures that NQF will endorse.The Physician Consortium on Performance Improvement (PCPI) seeks to develop the measures that NQF will endorse.
 [e.g., the National Quality Forum].The Secretary of HHS must seek endorsement of the quality measures by the entity with a contract with the Secretary under section 1890(a) [e.g., the National Quality Forum]. The Physician Consortium on Performance Improvement (PCPI) seeks to develop the measures that NQF will endorse.The Physician Consortium on Performance Improvement (PCPI) seeks to develop the measures that NQF will endorse..")
17
ACA authorizes PQRS payment incentives/adjustments:ACA authorizes PQRS payment incentives/adjustments: 2011: 1% incentive2011: 1% incentive 2012-2014: 0.5% incentive2012-2014: 0.5% incentive 2015: 98.5% payment adjustment of fee schedule (1.5% penalty for not reporting satisfactorily)2015: 98.5% payment adjustment of fee schedule (1.5% penalty for not reporting satisfactorily) 2016 and on: 98% payment adjustment2016 and on: 98% payment adjustment If an individual radiologist billed Medicare $200,000 in one year, the PQRS incentive would give them $2000 for PQRS.If an individual radiologist billed Medicare $200,000 in one year, the PQRS incentive would give them $2000 for PQRS. Assuming CMS reimburses!Assuming CMS reimburses! Incentive Payments for Physician Quality Reporting System (PQRS)
.")
18
Reporting Measures

19
Reporting Mechanisms Claims based-used in past but may change to make participation more “facile”.Claims based-used in past but may change to make participation more “facile”. CMS is moving toward a data registry based participation.CMS is moving toward a data registry based participation. –Radiology needs eligible registries –Establishing an eligible registry is challenging. ACR is developing registries in radiology.

20
What about MOCP?

21
Section 3002 of the Affordable Care Act (ACA) requires an option for a physician to provide CMS with data on quality measures through a Maintenance of Certification Program (MOCP) operated by an ABMS specialty body. The statute authorizes an additional incentive of 0.5 percent for 2011 – 2014, when requirements are met. Beyond 2014, participation in MOCP and successful completion of a MOCP practice assessment may be incorporated into the “composite of measures” of quality furnished under the physician fee schedule value-based payment modifier. An individual billing Medicare $200,000 in one year would receive an additional $2000 for participation. Individuals will not participate for a total of $2000 + $1000 The significance is not the incentive but instead allowed participation

22
MOCP Mechanics ABMS board e.g. ABR has applied for approval from CMS as the “submitter of data” for ABR diplomates to fulfill both part 4 of MOC for ABR recertification and qualification for MOCP reimbursement under the ACA.ABMS board e.g. ABR has applied for approval from CMS as the “submitter of data” for ABR diplomates to fulfill both part 4 of MOC for ABR recertification and qualification for MOCP reimbursement under the ACA. If approval is finalized, ABR MOC participants would then be eligible for the additional 0.5% incentive IF:If approval is finalized, ABR MOC participants would then be eligible for the additional 0.5% incentive IF: –They have met the PQRS requirements –They have “successfully completed a qualified MOC Program practice assessment for 2011” This is the only pathway by which the MOC PQRS incentive may be obtained. This is the only pathway by which the MOC PQRS incentive may be obtained. ABMS could establish the umbrella program for all ABMS boards to qualify for both MOC part 4 fulfillment and MOCP reimbursement under the ACAABMS could establish the umbrella program for all ABMS boards to qualify for both MOC part 4 fulfillment and MOCP reimbursement under the ACA

24
“To serve patients, the public, and the medical profession...” “...by certifying that its diplomates have acquired, demonstrated, and maintained a requisite standard of knowledge, skill, and understanding...”

Similar presentations


 Demonstration Jody Blatt Senior Research Analyst Project Officer, MAPCP Demonstration Medicare Demonstrations.>")


 Update David Laszakovits, M.B.A.>")









 and Physician Privileging>")
 Source: Centers for Medicare and.>")


