Download presentation
Presentation is loading. Please wait.

1
Pulmonary Embolism in the College Health Population
Vanessa Stoloff, MD University of Pennsylvania Student Health Services

2
This talk is entitled Pulmonary Embolism in the College Population
This talk is entitled Pulmonary Embolism in the College Population. I initially chose to talk about PE because it still is astonishing to me how relatively common this diagnosis can be – in a population where I never thought it would fall so high up on my differential list. I then realized that it would almost be impossible to talk about PE without talking about DVT. So I will define venous thromboembolism (VTE) as it is a blanket term for both – and branch out a bit and discuss each.
 as it is a blanket term for both – and branch out a bit and discuss each.")
3
Introduction What is venous thromboembolism?
Venous thromboembolism (VTE) refers to a blood clot occurring inside a blood vessel VTE is a relatively common diagnosis Each year two million cases of deep vein thrombosis (DVT) are diagnosed in the United States Another 600,000 patients are diagnosed with pulmonary embolism (PE) yearly DVT and PE can result in significant morbidity and mortality PE is a difficult diagnosis that may be missed because of non-specific clinical presentation However, early diagnosis is fundamental since early treatment is highly effective Along with clinical suspicion comes the importance of using validated algorithms + objective testing
 refers to a blood clot occurring inside a blood vessel. VTE is a relatively common diagnosis. Each year two million cases of deep vein thrombosis (DVT) are diagnosed in the United States. Another 600,000 patients are diagnosed with pulmonary embolism (PE) yearly. DVT and PE can result in significant morbidity and mortality. PE is a difficult diagnosis that may be missed because of non-specific clinical presentation. However, early diagnosis is fundamental since early treatment is highly effective. Along with clinical suspicion comes the importance of using validated algorithms + objective testing.")
4
Venous Thromboembolism - VTE
Types of VTE: Deep Vein Thrombosis – DVT Superficial Vein Thrombosis (SVT) Pulmonary Embolism PE
 Pulmonary Embolism PE.")
5
Venous Thromboembolism - VTE
Pathogenesis Virchow’s Triad – 3 primary influences that predispose to thrombus formation: Alterations in blood flow (ie. stasis) Alterations in the constituents of the blood (ie, inherited or acquired hypercoagulable state) Vascular endothelial damage Compression, immobility, ↑blood viscosity → stasis Clot formation develops (and if endothelial damage) → activation of platelets and coagulation cascade RBCs and fibrin accumulate and clot increases with ↑ risk of dislodgement First described by Rudolf Virchow more than a century ago… venous stasis increased activation of clotting factors and vessel wall damage remain the fundamental basis for our understanding of thrombosis.
 Alterations in the constituents of the blood (ie, inherited or acquired hypercoagulable state) Vascular endothelial damage. Compression, immobility, ↑blood viscosity → stasis. Clot formation develops (and if endothelial damage) → activation of platelets and coagulation cascade. RBCs and fibrin accumulate and clot increases with ↑ risk of dislodgement. First described by Rudolf Virchow more than a century ago… venous stasis. increased activation of clotting factors. and vessel wall damage. remain the fundamental basis for our understanding of thrombosis.")
6
Venous ThromboembolisM
Thrombogenesis - the process by which blood forms clots Hemostasis – cessation of bleeding Primary hemostasis Platelets immediately form a plug at the site of injury Secondary hemostasis (occurs simultaneously) Coagulation factors respond in a complex cascade to form fibrin strands Coagulation (thrombogenesis) is the process by which blood forms clots. It is an important part of hemostasis, the cessation of blood loss from a damaged vessel, wherein a damaged blood vessel wall is covered by a platelet and fibrin-containing clot to stop bleeding and begin repair of the damaged vessel. Disorders of coagulation can lead to an increased risk of bleeding (hemorrhage) or obstructive clotting (thrombosis). intricate multi-factorial process Platelets immediately form a plug at the site of injury; this is called primary hemostasis. Secondary hemostasis occurs simultaneously: Proteins in the blood plasma, called coagulation factors or clotting factors, respond in a complex cascade to form fibrin strands, which strengthen the platelet plug.
 Coagulation factors respond in a complex cascade to form fibrin strands. Coagulation (thrombogenesis) is the process by which blood forms clots. It is an important part of hemostasis, the cessation of blood loss from a damaged vessel, wherein a damaged blood vessel wall is covered by a platelet and fibrin-containing clot to stop bleeding and begin repair of the damaged vessel. Disorders of coagulation can lead to an increased risk of bleeding (hemorrhage) or obstructive clotting (thrombosis). intricate multi-factorial process. Platelets immediately form a plug at the site of injury; this is called primary hemostasis. Secondary hemostasis occurs simultaneously: Proteins in the blood plasma, called coagulation factors or clotting factors, respond in a complex cascade to form fibrin strands, which strengthen the platelet plug.")
7
Venous Thromboembolism - VTE
In over 80% of patients with VTE – risk factor for thrombosis can be identified Can often be more than one risk factor More commonly, 3+ risk factors (in one study 56%) Causes of venous thrombosis Inherited (Hereditary) Acquired Venous thromboembolism results from a combination of hereditary and acquired risk factors, also known as thrombophilia or hypercoagulable states.
 Causes of venous thrombosis. Inherited (Hereditary) Acquired. Venous thromboembolism results from a combination of hereditary and acquired risk factors, also known as thrombophilia or hypercoagulable states.")
8
Inherited Thrombophilia
Genetic tendency to venous thromboembolism Most frequent genetic causes Factor V Leiden mutation (most common) Prothrombin gene mutation Protein S deficiency Protein C deficiency Antithrombin deficiency Dysfibrinogenemia clotting or coagulation cascade YouTube video:
 Prothrombin gene mutation. Protein S deficiency. Protein C deficiency. Antithrombin deficiency. Dysfibrinogenemia. clotting or coagulation cascade. YouTube video: v=co6ar6vVp70.")
9
Inherited Thrombophilia
Genetic tendency to venous thromboembolism Most frequent genetic causes Factor V Leiden mutation (most common) Prothrombin gene mutation Protein S deficiency Protein C deficiency Antithrombin III deficiency Dysfibrinogenemia 50-60% of inherited VTE cases
 Prothrombin gene mutation. Protein S deficiency. Protein C deficiency. Antithrombin III deficiency. Dysfibrinogenemia % of inherited VTE cases.")
10
Inherited Thrombophilia
Genetic tendency to venous thromboembolism Most frequent genetic causes Factor V Leiden mutation (most common) Prothrombin gene mutation Protein S deficiency Protein C deficiency Antithrombin III deficiency Dysfibrinogenemia Most of the remaining cases
 Prothrombin gene mutation. Protein S deficiency. Protein C deficiency. Antithrombin III deficiency. Dysfibrinogenemia. Most of the remaining cases.")
11
Inherited Thrombophilia
Most of the remaining cases Once found to have a VTE, and started on treatment, there may be limitations to the testing to see if one might have an inherited thrombophilia.

12
Risk Factors- Other Anatomic Risk Factors Not known to be inherited
Elevated clotting Factors Not yet proven to be genetic – but are supposedly Anatomic Risk Factors - Not known to be inherited - Paget-Schroetter Syndrome (Underlying compressive anomaly at the thoracic outlet) - May-Thurner Syndrome (Compression of left common iliac vein) - Inferior Vena Cava Syndrome (Congenital venous malformations of the IVC) Elevated clotting factors - Not yet proven to be genetic – but are supposedly Associated with increased thrombotic risk Factor VIII, IX, XI, thrombin-activatable fibrinolysis inhibitor (TAFI), Interleukin 8 ABO blood group Non-O blood type Other plasma components
 - May-Thurner Syndrome (Compression of left common iliac vein) - Inferior Vena Cava Syndrome (Congenital venous malformations of the IVC) Elevated clotting factors - Not yet proven to be genetic – but are supposedly. Associated with increased thrombotic risk. Factor VIII, IX, XI, thrombin-activatable fibrinolysis inhibitor (TAFI), Interleukin 8. ABO blood group. Non-O blood type. Other plasma components.")
13
Acquired Thrombophilia
Central venous catheter Chronic liver disease Hyperviscosity Hyperhomocysteinemia Seasonal variation Cardiovascular risk factors Age Air pollution Microalbuminuria Heparin-induced thrombocytopenia Inflammatory bowel disease Trauma Prior thrombotic event Intravenous drug use Pregnancy Medications Immobilization Heart failure Antiphospholipid antibody syndrome Myeloproliferative disorders Renal disease Pretty long list of associations for thrombophilia – some stronger than others. - Trauma (major trauma, minor injuries) - Medications (OCPs, HRT, Tamoxifen, Bevacizumab (Avastin)) - Antiphospholipid antibody syndrome (associated with SLE and rheumatic disease) - Myeloproliferative disorders (PV, essential throbocythemia) - Renal disease (nephrotic syndrome, etc) - Seasonal variation (highest during winter months) - Cardiovascular risk factors (obesity, HTN, DM, smoking, hypercholesterolemia) Other major medical illnesses
 - Medications (OCPs, HRT, Tamoxifen, Bevacizumab (Avastin)) - Antiphospholipid antibody syndrome (associated with SLE and rheumatic disease) - Myeloproliferative disorders (PV, essential throbocythemia) - Renal disease (nephrotic syndrome, etc) - Seasonal variation (highest during winter months) - Cardiovascular risk factors (obesity, HTN, DM, smoking, hypercholesterolemia) Other major medical illnesses.")
14
Acquired Thrombophilia
Many patients have more than one risk factor. Six most prevalent pre-existing medical characteristics: Hospitalization in the past 3 months Surgery in the past 3 months > 48 hours of immobility in past month Malignancy in the past 3 months Infection in the past 3 months Current hospitalization Risk Factors % ≥ 3 53% 1-2 36%+ 11%

15
Acquired Thrombophilia - SHS
Major trauma/ Minor injuries Surgery (orthopedic) Medications (OCPs) Immobilization (prolonged sitting, extended travel) Pregnancy Prior thromboembolic event Intravenous drug use Genetic predisposition Bringing it back to the college health population, we need to remember that our population is at risk!
 Medications (OCPs) Immobilization (prolonged sitting, extended travel) Pregnancy. Prior thromboembolic event. Intravenous drug use. Genetic predisposition. Bringing it back to the college health population, we need to remember that our population is at risk!")
16
CASE # 1

17
Case # 1 - JW JW - 25 yo female – graduate school of Nursing
CC: L sided shoulder pain HPI: Healthy 25 yo female developed L sided shoulder pain x 3 days. Pain progressed down into her L chest. Pain described as a “pulled muscle”. Exacerbation with deep inspiration. Ran 11 miles and felt like she was unable to take a deep breath. While getting ready for her birthday dinner, friend told her she sounded more winded. She realized there was something wrong. Called on call provider after hours. Pain started near her left shoulder and migrated to under her left breast. Pain worse w/ cough, deep inspiration. Pt denied associated fever/chills, no cough. She had a "bad cold" 10 days prior - with clear rhinorrhea. Denies trauma to chest wall. Meds: Yasmin-28 After much discussion, she was sent to Emergency Dept. for further evaluation.

18
Case # 1 - JW ED evaluation
Additional History: No leg pain or swelling. No weakness/numbness. No prolonged immobilization or recent travel. No history of DVT. Pain 8/10. Physical Exam: VS: BP: 151/74 HR: 90 T: 99.0F RR: 16 Gen: 25 yo female tearful and concerned, but in no acute respiratory distress Lungs: CTAB, no wheezes, some discomfort with deep inspiration + Left CVA tenderness LE: pulses 2+, no calf swelling/warmth/ttp

19
Case # 1 - JW ED Evaluation Pulse Ox: 95%-100%
CXR: No active disease seen in the chest, no fractured ribs Labs: CBC, Chem-7 - normal D-dimer: Not done EKG: NSR, no acute ST changes Spiral CT: Bilateral segmental pulmonary emboli, occlusive on the left and non-occlusive on the right. Left anterior basilar pulmonary infarct. Small left pleural effusion with bibasilar atelectasis. Admitted for anticoagulation and pain control Low Wells score

21
Pulmonary Embolism - PE
PE is an obstruction of the pulmonary artery (or one of it’s branches) by material: Thrombus, tumor, air, fat PE can be classified as acute or chronic massive or sub-massive Acute PE is a common and often fatal disease Untreated PE is associated with ~ 30% mortality rate Mortality can be reduced by prompt diagnosis and therapy More than half of all PE are probably undiagnosed In an older study of >42 million deaths over 20 years, 1.5% were diagnosed with PE (now considered an underestimate) Since CT Pulmonary angiogram (CT-PA) incidence has increased from 62.1 to cases per 100,000 Most patients with acute PE have identifiable risk factors at time of presentation
 by material: Thrombus, tumor, air, fat. PE can be classified as. acute or chronic. massive or sub-massive. Acute PE is a common and often fatal disease. Untreated PE is associated with ~ 30% mortality rate. Mortality can be reduced by prompt diagnosis and therapy. More than half of all PE are probably undiagnosed. In an older study of >42 million deaths over 20 years, 1.5% were diagnosed with PE (now considered an underestimate) Since CT Pulmonary angiogram (CT-PA) incidence has increased from 62.1 to cases per 100,000. Most patients with acute PE have identifiable risk factors at time of presentation.")
22
Pulmonary Embolism - Pathophysiology
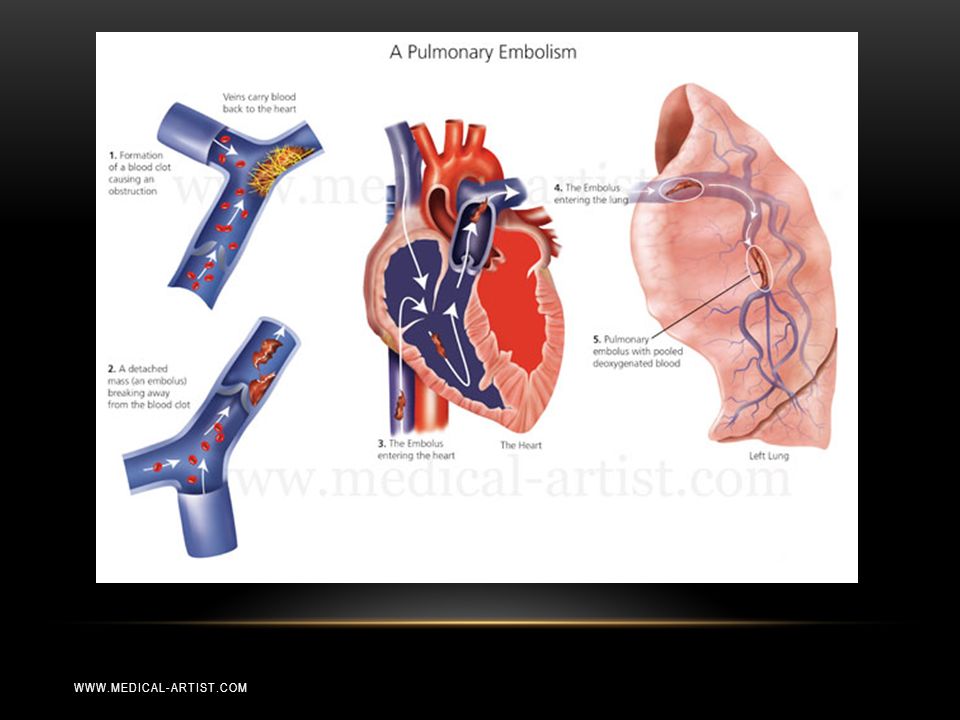
Most PE arise from thrombi in the deep venous system Iliofemoral veins are source of most clinically recognized PE May originate from right heart, or pelvic, renal, or upper extr veins Thrombi travel to lung and may lodge at bifuraction (saddle) Smaller thrombi can continue past main pulmonary artery and lobar branches More likely to produce pleuritic chest pain Can initiate an inflammatory response Lower lobes involved in majority of cases Most PEs are multiple
 Smaller thrombi can continue past main pulmonary artery. and lobar branches. More likely to produce pleuritic chest pain. Can initiate an inflammatory response. Lower lobes involved in majority of cases. Most PEs are multiple.")
23
Pulmonary Embolism – Signs & Symptoms
Most Common Symptoms Dyspnea at rest or with exertion (78%) Pleuritic pain (44%) Cough (34%) > 2-pillow orthopnea (28%) Calf or thigh pain (44%) Calf or thigh swelling (41%) Wheezing (21%) Signs and Symptoms and signs of PE are highly variable and nonspecific
 Pleuritic pain (44%) Cough (34%) > 2-pillow orthopnea (28%) Calf or thigh pain (44%) Calf or thigh swelling (41%) Wheezing (21%) Signs and Symptoms and signs of PE are highly variable and nonspecific.")
24
Pulmonary Embolism – Signs & Symptoms
Most Common Signs Tachypnea (54%) Tachycardia (24%) Rales (18%) Decreased breath sounds (17%) Accentuated pulmonic component of 2nd heart sound (15%) Jugular venous distension (14%)
 Tachycardia (24%) Rales (18%) Decreased breath sounds (17%) Accentuated pulmonic component of 2nd heart sound (15%) Jugular venous distension (14%)")
25
Pulmonary Embolism – Signs & Symptoms
Highly variable and nonspecific Frequency similar among patients with and without PE PE is frequently asymptomatic Clinical impression alone has a sensitivity and specificity of 85% and 51% Not helpful diagnostically

26
Diagnostic testing is necessary before confirming or excluding diagnosis of PE

27
Pulmonary Embolism - PE
Importance of using validated algorithms and various scoring systems Help to determine the a priori clinical probability of PE and DVT Pulmonary Embolism Severity Index (PESI) Simplified PESI Wells Criteria Modified Wells Criteria Pulmonary Embolism Rule-Out Criteria (PERC) Geneva Scoring System - many tools developed to try to help guide in the diagnosis of PE - importance of using validated algorithms and various scoring systems – but they must stem from one’s initial clinical suspicion. For DVT and PE, there are various scoring systems that are used to determine the a priori clinical probability of these diseases a pri·o·ri (ä pr-ôr, -r, pr-ôr, -r) adj. 1. Proceeding from a known or assumed cause to a necessarily related effect; deductive. 2. a. Derived by or designating the process of reasoning without reference to particular facts or experience. b. Knowable without appeal to particular experience. 3. Made before or without examination; not supported by factual study.
 Simplified PESI. Wells Criteria. Modified Wells Criteria. Pulmonary Embolism Rule-Out Criteria (PERC) Geneva Scoring System. - many tools developed to try to help guide in the diagnosis of PE. - importance of using validated algorithms and various scoring systems – but they must stem from one’s initial clinical suspicion. For DVT and PE, there are various scoring systems that are used to determine the a priori clinical probability of these diseases. a pri·o·ri (ä pr-ôr, -r, pr-ôr, -r) adj. 1. Proceeding from a known or assumed cause to a necessarily related effect; deductive. 2. a. Derived by or designating the process of reasoning without reference to particular facts or experience. b. Knowable without appeal to particular experience. 3. Made before or without examination; not supported by factual study.")
28
Pulmonary Embolism Severity Index (PESI)
10 variables + Patient Age = PESI score Male sex (+10 points) Hx of Cancer (+30) Heart failure (+10) Chronic lung disease (+10) Pulse ≥ 110 bpm (+20) Systolic BP < 100 mmHg (+30) Respiratory rate ≥ 30 breaths/min (+20) Temperature < 36 degrees C˚ Altered mental status (+60) Arterial oxygen saturation < 90 (+20) Difficult to apply in a busy clinical setting Risk Class for Mortality Points Class I < 66 Class II 66-85 Class III 86-105 Class IV Class V >125
 Hx of Cancer (+30) Heart failure (+10) Chronic lung disease (+10) Pulse ≥ 110 bpm (+20) Systolic BP < 100 mmHg (+30) Respiratory rate ≥ 30 breaths/min (+20) Temperature < 36 degrees C˚ Altered mental status (+60) Arterial oxygen saturation < 90 (+20) Difficult to apply in a busy clinical setting. Risk Class for Mortality. Points. Class I. < 66. Class II Class III Class IV Class V. >125.")
29
Pulmonary Embolism Severity Index (PESI)
Simplified PESI Assigns one point for each of several variables Age >80 History of cancer Chronic cardiopulmonary disease Hear rate ≥ 110 bpm Systolic BP < 100 mmHg Arterial oxyhemoglobin saturation < 90% Seems to have a prognostic accuracy similar to the original PESI Risk Class for Mortality Points Low risk High risk >1

30
Wells’ criteria for Probability of PE
Wells’ Criteria for Pulmonary Embolism Clinical Signs and Symptoms of DVT +3 PE is #1 diagnosis, or equally likely Heart Rate >100 +1.5 Immobilization at least 3 days or Surgery in the previous 4 weeks Previously, objectively diagnosed PE or DVT? Hemoptysis +1 Malignancy with treatment within 6 months or palliative Patient has none of these Wells criteria has been used extensively – probably the best known

31
Wells’ criteria for Probability of PE
Clinical Probability Assessment Score High > 6.0 Moderate 2.0 to 6.0 Low < 2.0 Modified Clinical Probability Assessment Score PE likely > 4.0 PE unlikely ≤ 4.0

32
Revised Geneva Scoring System For PE
Age > 65 years 1 Previous DVT or PE 3 Surgery (gen anesthia) or fx (lower extremities) within 1 month 2 Active malignant condition Unilateral lower limb pain Hemoptysis Heart rate bpm Heart rate ≥ 95 bpm 5 Pain on LE deep venous palpation and unilateral edema 4 Much like the Wells criteria is the Geneva criteria, which depend on objective measures
 or fx (lower extremities) within 1 month. 2. Active malignant condition. Unilateral lower limb pain. Hemoptysis. Heart rate bpm. Heart rate ≥ 95 bpm. 5. Pain on LE deep venous palpation and unilateral edema. 4. Much like the Wells criteria is the Geneva criteria, which depend on objective measures.")
33
Revised Geneva Scoring System For PE
Clinical Probability Assessment Score High ≥ 11 Intermediate 4 - 10 Low 0 - 3

34
Pulmonary Embolism Rule-out Criteria - PERC
PERC (Pulmonary Embolism Rule-out Criteria) rule can significantly decrease work-up for pulmonary embolism Created for use by Emergency Medicine Clinicians To apply this rule, the clinician must first use clinical gestalt to classify the patient as low risk Eight clinical criteria (+ history, physical and VS) used to help decision making: Age < 50 years Pulse < 100 bpm SaO2 > 94% No unilateral leg swelling No hemoptysis No recent trauma or surgery No prior PE or DVT No hormone use If all criteria are present and pre-test probability is ≤15%, then there is less than a 2% risk that a patient has a PE, no further work-up is needed ge·stalt noun \gə-ˈstält, -ˈshtält, -ˈstȯlt, -ˈshtȯlt\ Definition of GESTALT: a structure, configuration, or pattern of physical, biological, or psychological phenomena so integrated as to constitute a functional unit with properties not derivable by summation of its parts Use of GESTALT. Collection of entities that creates a unified concept Looking at something as a whole.
 rule can significantly decrease work-up for pulmonary embolism. Created for use by Emergency Medicine Clinicians. To apply this rule, the clinician must first use clinical gestalt to classify the patient as low risk. Eight clinical criteria (+ history, physical and VS) used to help decision making: Age < 50 years. Pulse < 100 bpm. SaO2 > 94% No unilateral leg swelling. No hemoptysis. No recent trauma or surgery. No prior PE or DVT. No hormone use. If all criteria are present and pre-test probability is ≤15%, then there is less than a 2% risk that a patient has a PE, no further work-up is needed. ge·stalt noun \gə-ˈstält, -ˈshtält, -ˈstȯlt, -ˈshtȯlt\ Definition of GESTALT: a structure, configuration, or pattern of physical, biological, or psychological. phenomena so integrated as to constitute a functional unit with properties not. derivable by summation of its parts. Use of GESTALT. Collection of entities that creates a unified concept. Looking at something as a whole.")
35
Just an example of one of the many algorithms to be found
36
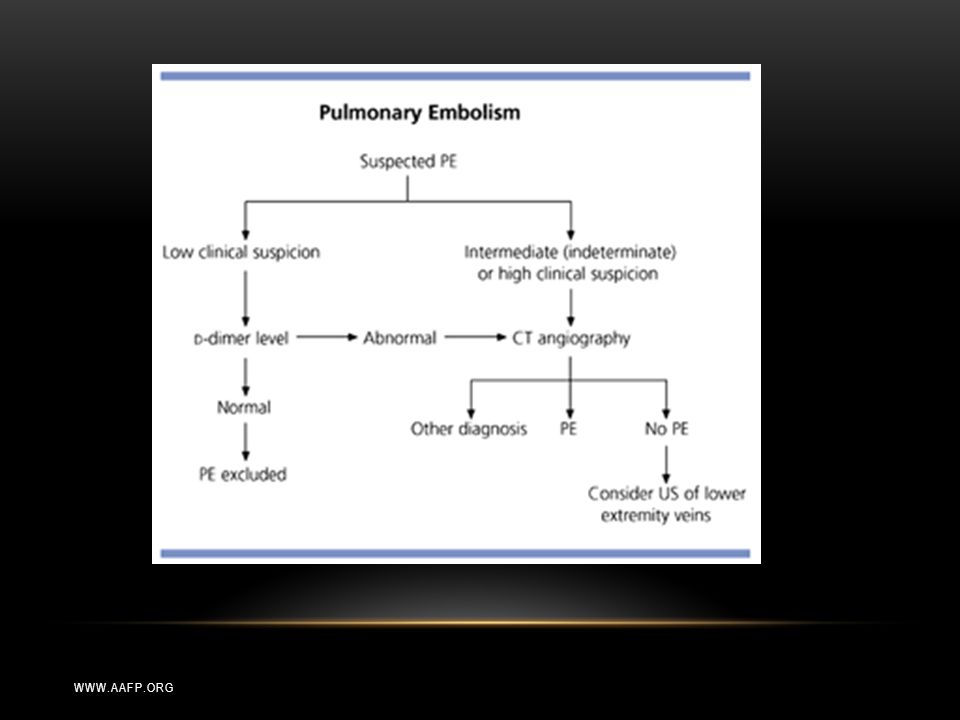
Thankfully some are less complicated.
37
Pulmonary Embolism – OBJECTIVE Testing
Importance of using validated algorithms + objective testing Routine lab findings are usually nonspecific (↑WBCs, ↑ESR, ↑LDH, ↑AST) Arterial blood gas (ABG) (hypoxemia, hypocapnia, resp alk) Pulse oximetry (<95% ↑ risk of complications) Brain natriuretic peptide (BNP) (↑BNP, but insensitive and nonspecific) Troponin I and T (↑ 30-50% with moderate to severe PE) Electrocardiography (Non-specific ST-segment,T-wave changes) Chest radiography importance of using clinical judgement and validated algorithms. Diagnostic testing is necessary before confirming or excluding diagnosis of PE Routine lab findings are usually non-specific. - ABGs are generally NOT done in college health clinics, more used in EDs or other hospital settings Not useful in diagnosis. - Pulse Ox and Troponin – more used for prognosis – associated with adverse outcomes - Many college health centers can perform EKGs, some even have their own radiology, however, these tests, too, are often of low yield. - However - EKGs also can be used for prognosis (Atrial Atrial arrhythmias, RBBB, Inferior Q waves, Precordial T-wave inversion) - CXR can show Atelectasis,Pleural effusion.
 Arterial blood gas (ABG) (hypoxemia, hypocapnia, resp alk) Pulse oximetry (<95% ↑ risk of complications) Brain natriuretic peptide (BNP) (↑BNP, but insensitive and nonspecific) Troponin I and T (↑ 30-50% with moderate to severe PE) Electrocardiography (Non-specific ST-segment,T-wave changes) Chest radiography. importance of using clinical judgement and validated algorithms. Diagnostic testing is necessary before confirming or excluding diagnosis of PE. Routine lab findings are usually non-specific. - ABGs are generally NOT done in college health clinics, more used in EDs or other hospital settings. Not useful in diagnosis. - Pulse Ox and Troponin – more used for prognosis – associated with adverse outcomes. - Many college health centers can perform EKGs, some even have their own radiology, however, these tests, too, are often of low yield. - However - EKGs also can be used for prognosis (Atrial Atrial arrhythmias, RBBB, Inferior Q waves, Precordial T-wave inversion) - CXR can show Atelectasis,Pleural effusion.")
38
Pulmonary Embolism – Testing
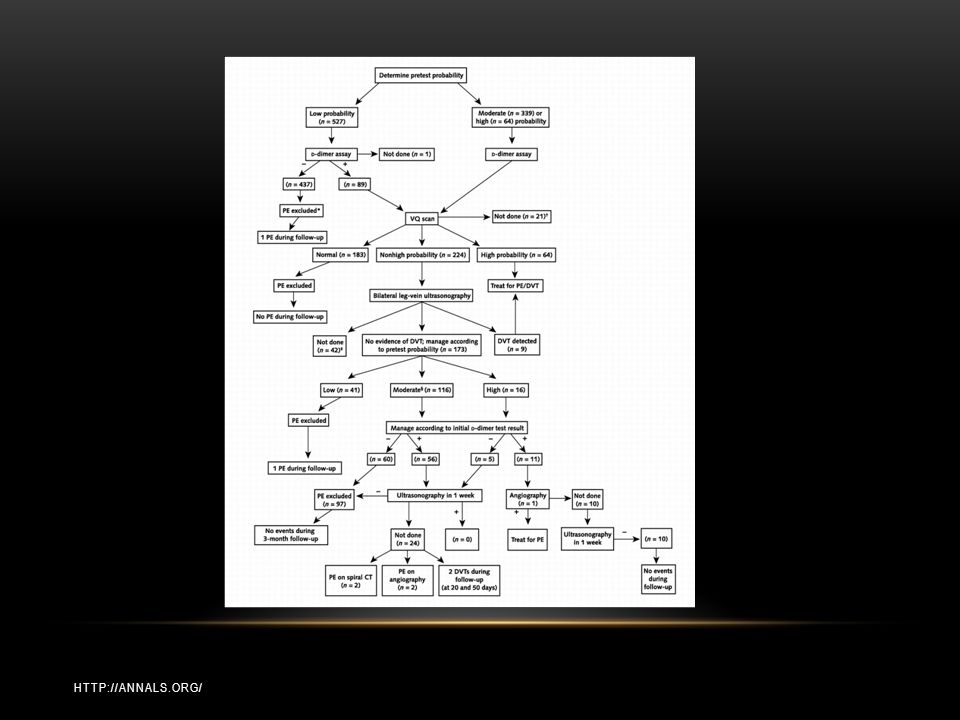
Ventilation/Perfusion (V/Q) Scan Lower extremity ultrasound D-dimer – (measurable degradation product of cross-linked fibrin) Angiography “gold standard” in diagnosis of acute PE Spiral (helical) CT with intravenous contrast – CT Pulmonary Angiography (CT-PA) Ability to detect alternative pulmonary abnormalities MR Angiography (MRA) Echocardiography - V/Q scan determines the vent/perfusion ratio - Ultrasound – flawed in it’s use for PE. Sometimes used with serial exams – if anticoag is withheld. - D-Dimer – we’ll talk more about it’s use - Angiography – still considered the “gold standard” in diagnosis of acute PE Inject contrast into a pulmonary artery branch after percutaneous catheterization (femoral vein) Negative pulmonary angiogram excludes clinically relevant PE Generally safe and well tolerated Mortality < 2%, Morbidity ~5% but…(catheter, contrast rxn, arrhythmia, respiratory insuff) - Spiral (helical) CT with intravenous contrast – CT Pulmonary Angiography (CT-PA) Being used increasingly Ability to detect alternative pulmonary abnormalities (that may otherwise explain patient’s symptoms) - MR Angiography (MRA) Not currently in favor as limited by respiratory and cardiac motion artifact - Echocardiography Only 30-40% of patients with PE will have Echo abnormalities suggestive of PE Increased RV size Decreased RV function Tricuspid regurgitation
 Scan. Lower extremity ultrasound. D-dimer – (measurable degradation product of cross-linked fibrin) Angiography. gold standard in diagnosis of acute PE. Spiral (helical) CT with intravenous contrast – CT Pulmonary Angiography (CT-PA) Ability to detect alternative pulmonary abnormalities. MR Angiography (MRA) Echocardiography. - V/Q scan determines the vent/perfusion ratio. - Ultrasound – flawed in it’s use for PE. Sometimes used with serial exams – if anticoag is withheld. - D-Dimer – we’ll talk more about it’s use. - Angiography – still considered the gold standard in diagnosis of acute PE. Inject contrast into a pulmonary artery branch after percutaneous catheterization (femoral vein) Negative pulmonary angiogram excludes clinically relevant PE. Generally safe and well tolerated. Mortality < 2%, Morbidity ~5% but…(catheter, contrast rxn, arrhythmia, respiratory insuff) - Spiral (helical) CT with intravenous contrast – CT Pulmonary Angiography (CT-PA) Being used increasingly. Ability to detect alternative pulmonary abnormalities (that may otherwise explain patient’s symptoms) - MR Angiography (MRA) Not currently in favor as limited by respiratory and cardiac motion artifact. - Echocardiography. Only 30-40% of patients with PE will have Echo abnormalities suggestive of PE. Increased RV size. Decreased RV function. Tricuspid regurgitation.")
39
CASE # 2

40
Case # 2- MD MD - 21 yo female CC: difficulty breathing while working out HPI: 21 yo female recently in Emergency Dept (2 weeks prior) for “severe allergic reaction” -- diagnosed as urticaria (unknown cause). Treated with prednisone and antihistamines, discharged. No breathing concerns at that time (no wheezing, SOB). She had a “super bad cold” at that time, felt she might have been having some SOB after running. Now her complaint is that her SOB is still present. Now describes her condition as “feeling OK while running – up to a point”. She will develop a burning sensation in her lungs with running -- “not in a good way”. Her parents encouraged her to go to SHS so that she could have “blood work” and a “mono test”. She is already scheduled to see Allergy.
 for severe allergic reaction -- diagnosed as urticaria (unknown cause). Treated with prednisone and antihistamines, discharged. No breathing concerns at that time (no wheezing, SOB). She had a super bad cold at that time, felt she might have been having some SOB after running. Now her complaint is that her SOB is still present. Now describes her condition as feeling OK while running – up to a point . She will develop a burning sensation in her lungs with running -- not in a good way . Her parents encouraged her to go to SHS so that she could have blood work and a mono test . She is already scheduled to see Allergy.")
41
Case # 2- MD PMHx: unremarkable healthy 21 yo female
No history of asthma May have slight seasonal allergies (doesn’t use meds) FHx: non-contributory SHx: non-smoker non-drinker senior - studying business and Chinese Runner - has run in marathons before, training for 10K run next month Meds: OCPs
 FHx: non-contributory. SHx: non-smoker. non-drinker. senior - studying business and Chinese. Runner - has run in marathons before, training for 10K run next month. Meds: OCPs.")
42
Case # 2- MD Physical Exam:
Vital Signs: BP: 121/72 HR: 67 T: 97.8 RR: 14 GEN: well-developed, well-nourished, speaking in full sentences with no effort HEENT: unremarkable Lungs: CTAB, no wheezing, no pleurisy Heart: RRR, no murmurs Ext: WNL, no calf pain or edema, Neg Homans Peak Flows: 450 → 440 → 440 Pox: 95-96%

43
Case # 2- MD Wells Score = 0 Impression:
21 year old otherwise healthy female Dyspnea on exertion Decreased Pulse Ox Oral contraceptives Work up: CXR CBC, TSH, Mono screen (parent’s request) D-Dimer? Rx: Albuterol MDI Disposition: Stable. Since evening appt. was discharged to home. Advised to get CXR in AM. Will contact in AM with results. Trial of bronchodilator. Wells Criteria for PE Score Clinical Signs and Symptoms for DVT 3 PE is most likely diagnosis HR >100 1.5 Immobilization 3 days/Surgery in 4 weeks Previous PE or DVT Hemoptysis 1 Malignancy within 6 mos Patient has none Wells Score = 0
 D-Dimer Rx: Albuterol MDI. Disposition: Stable. Since evening appt. was discharged to home. Advised to get CXR in AM. Will contact in AM with results. Trial of bronchodilator. Wells Criteria for PE. Score. Clinical Signs and Symptoms for DVT. 3. PE is most likely diagnosis. HR > Immobilization 3 days/Surgery in 4 weeks. Previous PE or DVT. Hemoptysis. 1. Malignancy within 6 mos. Patient has none. Wells Score = 0.")
44
Should I request a D-dimer???
PERC Rules actually say we “can” get a D-Dimer – because she is on hormones (OCPs)
")
45
D-Dimer D-dimers are a fibrin degradation product
Elevated if increased plasmin-activated fibrinolysis during thrombosis D-dimer testing is of clinical use when there is a suspicion of DVT or PE If low or moderate probability of DVT, a D-dimer level might be obtained, which excludes a diagnosis if results are normal When individuals are at a high-probability of having DVT, diagnostic imaging is preferred to a D-dimer test D-dimer < 500 ng/ml (<0.50 mcg/ml) is sufficient to exclude PE in patients with a low or moderate pretest probability of PE D-Dimer is a byproduct of thrombosis. If present, there is likelihood of clot.
 is sufficient to exclude PE in patients with a low or moderate pretest probability of PE. D-Dimer is a byproduct of thrombosis. If present, there is likelihood of clot.")
46
- + D-Dimer Clinically useful when there is a suspicion of DVT or PE
Variety of different assays (rapid tests) Good sensitivity and negative predictive value Abnormal in 95% of all patients with PE Hospitalized patients often have elevated levels for multiple reasons ↑ levels require further investigation with diagnostic imaging Poor specificity and positive predictive value Normal in only 40-68% patients without PE Rapid D-dimer assays are available – not at our SHS – which can often limit it’s usefulness in our setting. Other things that can elevate D-Dimer levels: False positive readings can be due to various causes: liver disease, high Rheumatoid factor, inflammation, malignancy, trauma, pregnancy, recent surgery, advanced age, etc.
 Good sensitivity and negative predictive value. Abnormal in 95% of all patients with PE. Hospitalized patients often have elevated levels for multiple reasons. ↑ levels require further investigation with diagnostic imaging. Poor specificity and positive predictive value. Normal in only 40-68% patients without PE. Rapid D-dimer assays are available – not at our SHS – which can often limit it’s usefulness in our setting. Other things that can elevate D-Dimer levels: False positive readings can be due to various causes: liver disease, high Rheumatoid factor, inflammation, malignancy, trauma, pregnancy, recent surgery, advanced age, etc.")
47
Case # 2- MD Results: (seen the next day)
CBC: WBC: 9.6, Hgb/Hct: 13.8/40.6, TSH: 1.94, Mono spot negative – all WNL D-Dimer – 4.38 mcg/ml FEU (<0.50) Now what!?: Unable to reach patient via telephone. Left /secure message: Hi Maria - I just left you a voice message... PLEASE contact me at as soon as you get these results. I am concerned about your D-Dimer level (the one we discussed yesterday at length). It is elevated which increases my suspicion for a possible clot in your lungs. I have already contacted the ED at HUP and they are expecting you. PLEASE head over to HUP ED now at 34th & Spruce. Call me on the way.... Now what!?!
 Now what! : Unable to reach patient via telephone. Left /secure message: Hi Maria - I just left you a voice message... PLEASE contact me at as soon as you get these results. I am concerned about your D-Dimer level (the one we discussed yesterday at length). It is elevated which increases my suspicion for a possible clot in your lungs. I have already contacted the ED at HUP and they are expecting you. PLEASE head over to HUP ED now at 34th & Spruce. Call me on the way.... Now what! !")
48
Case # 2- MD Thankfully, she got my messages and contacted SHS. She was promptly sent to the ED. ED Evaluation: CC: “I was seen yesterday at SHS. I have a low pulse ox and + D-dimer” Exam: VSS, exam WNL Pulse Ox: 95% CXR: No active disease EKG: NSR at 74 bpm CT: Large pulmonary emboli most of both lower lobe pulmonary arteries with the right embolus extending from the upper to the lower lobe and occluding most of the upper lobe and middle lobe pulmonary arteries. Admitted for anticoagulation (given SC dalteparin)
")
49
Case # 2- MD Why did I order the D-Dimer?
“PE, or Not PE?: That is the Question” So, why did I order the D-dimer? This presentation was initially named PE or Not PE: That is the question. Like Hamlet’s soliloquy… But it really is the question. Did I only order it because her because mom wanted her to have a mono test – and since I was drawing blood… Am I psychic? Was it a sixth sense? Or was I just using the force? Isn’t that all part of clinical gestalt after all? I would argue that: A little intuition + a lot of objectivity = proper diagnosis And while I am as much a believer in evidence-based medicine, there is some merit to clinical experience and going a little bit with your gut. There’s also a joke in my office as I tend to have more patients with the diagnosis of PE… is ending up in MY SCHEDULE an independent risk factor for PE? Or is it just that I/m looking for it more now? Whatever it is…. it’s important to have PE on your Differential diagnosis list – even in a young, healthy college population! a little intuition + a lot of objectivity = proper diagnosis

50
CASE #3

51
Case # 3 BS - 28 yo male CC: Heart racing, SOB with movement, a bit dizzy HPI: Healthy 28 yo male s/p recent arthroscopic ACL repair 5 days prior. Complicated post-op course with pneumonitis/pneumonia for which he was admitted for IV antibiotics. Was discharged to home following day. Developed fever and some chest tightness along with SOB 1 day ago. Tmax: yesterday 101.7 Meds: Albuterol MDI, Hydromorphone

52
Case # 3 Physical Exam: Vitals: BP: 153/91 HR: 96 T: 98.9 Pox: 95-96%, HR: Well appearing, NAD Lungs: CTAB L knee in immobilizer Impression: Post-op (Orthopedic procedure), Tachycardic secondary to pain? vs infection? vs PE? Wells criteria: Moderate probability (Post-op + immobilized, ?sign of DVT) Sent to Emergency Dept for further evaluation needs repeat CXR ?CT ?IV ABX
, Tachycardic secondary to pain vs infection vs PE Wells criteria: Moderate probability (Post-op + immobilized, sign of DVT) Sent to Emergency Dept for further evaluation. needs repeat CXR. CT. IV ABX.")
53
Case # 3 ED evaluation History: Sent to ED for “fever/cough/tachycardia since operation 5 days ago”. At ED, denies CP/SOB, No N/V. +Mild left knee pain, unchanged since operation Post-op history: Patient was observed to have fever in PACU and was treated for pneumonitis (? aspiration during intubation) vs. malignant hyperthermia (patient has family member with history of MH). Patient was observed in SICU overnight and discharged home on azithromycin.
 vs. malignant hyperthermia (patient has family member with history of MH). Patient was observed in SICU overnight and discharged home on azithromycin.")
54
Case # 3 ED evaluation Physical Exam:
Vital Signs: BP:142/70 HR: 122 T: F RR: 18 GEN: well-developed, well-nourished, in mild distress Lungs: CTAB, unlabored respirations with no accessory muscle use Heart: regular, tachycardic, no murmurs, no JVD Ext: left knee with +swelling, no warmth/erythema, appropriately tender, suture line c/d/i, +slight LE edema to calf

55
Case # 3 ED Evaluation Pulse Ox: 98%
CXR: Interval resolution of previously noted right upper and lower lobe alveolar opacities. Ultrasound: Vascular studies reveal probable calf vein thrombus Labs: CBC, Chem-7 – normal, WBC: 7.2 D-dimer: Not done EKG: Not done Spiral CT: Multiple bilateral pulmonary emboli as described, more extensive on the left. Enlarged main pulmonary artery to 3.4 cm, findings suggest right heart strain. Admitted for anticoagulation and pain control

56
Deep Vein Thrombosis - DVT
DVT of the lower extremity Distal (deep calf veins) Proximal (involves popliteal, femoral, iliac veins) Mortality rate of proximal DVT >> distal DVT Over 90% of acute PE are due to emboli emanating from the proximal veins Actual physical signs of DVT can be quite unreliable Not necessarily a correlation between the location of symptoms and site of thrombosis DVT of the upper extremity is less frequent Increasing incidence DVT of the lower extremity Distal (confined to deep calf veins) More associated with transient risk factors Proximal (involves popliteal, femoral, iliac veins) More associated with serious chronic disease Higher risk of progression to PE DVT of the upper extremity is less frequent Increasing incidence (likely because of ↑ indwelling central venous catheters)
 Proximal (involves popliteal, femoral, iliac veins) Mortality rate of proximal DVT >> distal DVT. Over 90% of acute PE are due to emboli emanating from the proximal veins. Actual physical signs of DVT can be quite unreliable. Not necessarily a correlation between the location of symptoms and site of thrombosis. DVT of the upper extremity is less frequent. Increasing incidence. DVT of the lower extremity. Distal (confined to deep calf veins) More associated with transient risk factors. Proximal (involves popliteal, femoral, iliac veins) More associated with serious chronic disease. Higher risk of progression to PE. DVT of the upper extremity is less frequent. Increasing incidence (likely because of ↑ indwelling central venous catheters)")
57
Deep Vein Thrombosis – Signs & Symptoms
Most Common Signs and Symptoms Pain or tenderness Erythema or discoloration Warmth Swelling Larger leg circumference in affected leg Homan’s sign – increased resistance to dorsiflexion of the foot +/- pain Visible surface veins Leg fatigue Signs and Symptoms and signs of DVT are more specific than with PE Pain or tenderness in one or both legs, which may occur only while standing or walking Red or discolored skin in the affected leg Warmth in the skin of the affected leg Swelling in one or both legs

58
Deep Vein Thrombosis – DVT of lower extremity
Differential Diagnosis Muscle strains, pulls, tears, and twists – 40% Leg swelling in paralyzed limb – 9% Lymphangitis – 7% Venous insufficiency – 7% Popliteal cysts (Baker’s cyst) – 5% Cellulitis – 3% Knee abnormality – 2% Compartment syndrome – 1% Unknown – 26%
 – 5% Cellulitis – 3% Knee abnormality – 2% Compartment syndrome – 1% Unknown – 26%")
59
Deep Vein Thrombosis– Signs & Symptoms
Only a minority of patients suspected of having DVT on clinical grounds actually has DVT Accurate diagnosis is essential High potential risks with diagnosis Untreated proximal DVT → can lead to fatal PE Anticoagulating patient without DVT → can lead to serious bleeding Importance of using validated algorithms + objective testing along with clinical suspicion Accurate diagnosis is essential - so take a detailed history Remember to ask about: recent potential precipitating conditions Use of OCPs/medications Past Medical History – prior VTE?, other illness Family History of coagulopathies Importance of OBJECTIVE diagnostic testing.

60
Wells’ criteria for Probability of DVT
Clinical Feature Score Active cancer +1 Paralysis, paresis, plaster (cast) Bedridden >3 days OR major surgery w/in 4 weeks Localized tenderness Swelling of entire leg Calf swelling > 3 cm Unilateral Pitting edema Previous documented DVT Collateral superficial veins Alternative diagnosis less likely -2 There’s even a Well’s score for DVT. The most studied clinical prediction rule is the Wells score for DVT Useful for differentiating low-probability patients (less than 10% prob DVT) from high-probability patients (> 65% prob DVT)
 Bedridden >3 days OR major surgery w/in 4 weeks. Localized tenderness. Swelling of entire leg. Calf swelling > 3 cm. Unilateral Pitting edema. Previous documented DVT. Collateral superficial veins. Alternative diagnosis less likely. -2. There’s even a Well’s score for DVT. The most studied clinical prediction rule is the Wells score for DVT. Useful for differentiating low-probability patients (less than 10% prob DVT) from high-probability patients (> 65% prob DVT)")
61
Wells’ criteria for Probability of DVT
Interpretation Score of 0 = low probability of DVT (less than 10%) Score of 1 or 2 = moderate probability of DVT Score of 3 or more = high probability of DVT (more than 65%)
 Score of 1 or 2 = moderate probability of DVT. Score of 3 or more = high probability of DVT (more than 65%)")
62
More algorithms

63
Deep Vein Thrombosis – OBJECTIVE Testing
D-Dimer Imaging Contrast Venography (gold standard) Compression Ultrasound with Doppler (real-time B-mode) Widely available Been proved accurate for diagnosing acute, symptomatic, proximal DVT Computed tomography (CT) – with contrast Magnetic resonance imaging (MRI) D-Dimer – we spoke about. Same clot – same fibrin degradation products Imaging Contrast Venography (gold standard) Invasive Used when noninvasive testing is non-diagnostic or impossible to perform Not for use in pregnancy Compression Ultrasound with Doppler (real-time B-mode) Non-invasive Widely available Been proved accurate for diagnosing acute, symptomatic, proximal DVT Duplex (D/B mode) Ultrasound – combo to detect flow and brightness Serial ultrasounds recommended for symptomatic patients with negative initial studies Computed tomography (CT) – with contrast With contrast Quick (1-4 minute scan) Not limited by casts, pain, open wounds, burns, obesity Allows visualization of IVC, SVC, heart, contralateral limb (for comparison) Magnetic resonance imaging (MRI) Directly images thrombi and non-occlusive clots Useful for visualization of both acute and chronic clots Useful when clot is in pelvis, IVC, arms Contrast nor radiation is required
 Compression Ultrasound with Doppler (real-time B-mode) Widely available. Been proved accurate for diagnosing acute, symptomatic, proximal DVT. Computed tomography (CT) – with contrast. Magnetic resonance imaging (MRI) D-Dimer – we spoke about. Same clot – same fibrin degradation products. Imaging. Contrast Venography (gold standard) Invasive. Used when noninvasive testing is non-diagnostic or impossible to perform. Not for use in pregnancy. Compression Ultrasound with Doppler (real-time B-mode) Non-invasive. Widely available. Been proved accurate for diagnosing acute, symptomatic, proximal DVT. Duplex (D/B mode) Ultrasound – combo to detect flow and brightness. Serial ultrasounds recommended for symptomatic patients with negative initial studies. Computed tomography (CT) – with contrast. With contrast. Quick (1-4 minute scan) Not limited by casts, pain, open wounds, burns, obesity. Allows visualization of IVC, SVC, heart, contralateral limb (for comparison) Magnetic resonance imaging (MRI) Directly images thrombi and non-occlusive clots. Useful for visualization of both acute and chronic clots. Useful when clot is in pelvis, IVC, arms. Contrast nor radiation is required.")
64
If only it were this easy….
TREATMENT OPTIONS. If only it were this easy….

65
Venous Thromboembolism - Treatment
Anticoagulant therapy Thrombolysis Inferior vena caval filters Embolectomy

66
Venous Thromboembolism - Treatment
Anticoagulation is the main therapy for acute PE and DVT Goal is to decrease mortality by preventing recurrent VTE Parenteral anticoagulant therapy should be initiated in all patients whom acute PE has been confirmed Efficacy of parenteral anticoagulant therapy depends upon achieving a therapeutic level within the first 24 hours of treatment. LMWH and fondaparinux are the preferred anticoagulants for initial therapy in most cases of acute PE as they confer superior or equivalent outcomes, are more convenient, and are associated with less thrombocytopenia. focus on anticoagulation - mainstay of therapy for both PE and DVT.

67
ANTICOAGULATION – Treatment of PE
Common questions asked by clinicians: Should I initiate anticoagulant therapy? Which anticoagulant should I initiate? What is the appropriate dose? How should I monitor treatment? What is the clinical evidence supporting its use? What are the common complications? For how long should I treat?

68
ANTICOAGULATION – Decision to anticoagulate
Bleeding Risk Factors Age >65 years Previous bleeding Thrombocytopenia Antiplatelet therapy Poor anticoagulant control Recent surgery Frequent falls Reduced functional capacity Previous stroke Diabetes Anemia Cancer Renal failure Liver failure Alcohol abuse Risk Class for Bleeding Points Low risk Moderate risk 1 High risk 2+ Should one initiate anticoagulation? That’s more of a role for an Emergency provider. However, it’s important to be aware of bleeding risk factors. Most of our patients will have NONE. (Maybe alcohol abuse risk of fall)
")
70
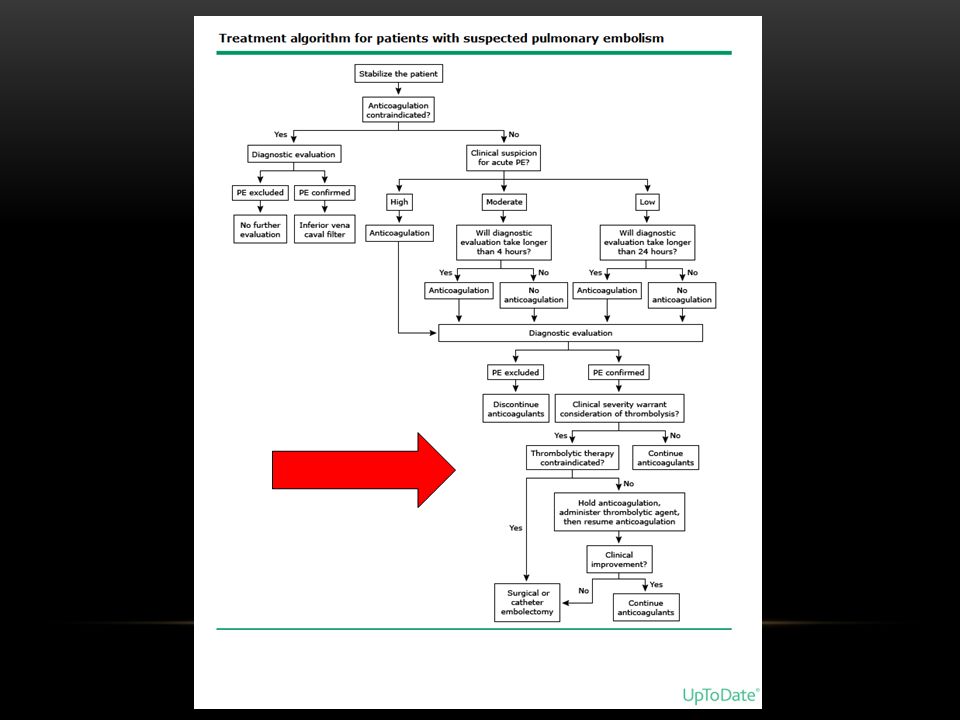
ANTICOAGULATION – Initiation
If clinical suspicion is HIGH - empiric anticoagulation is recommended If suspicion is MODERATE and the diagnostic evaluation is > 4 hours, anticoagulate Anticoagulation is NOT recommended empirically if suspicion is LOW. > Risk of recurrent PE without optimal anticoagulation (25%) Risk of major bleed with anticoagulant therapy (3%) If clinical suspicion is HIGH - when using validated prediction rule (ie. Wells criteria), empiric anticoagulation during diagnostic evaluation is recommended If suspicion is MODERATE and the diagnostic evaluation is expected to take > 4 hours, empiric anticoagulation is also warranted. Anticoagulation is NOT recommended empirically if suspicion is LOW.
 Risk of major bleed with anticoagulant therapy (3%) If clinical suspicion is HIGH - when using validated prediction rule (ie. Wells criteria), empiric anticoagulation during diagnostic evaluation is recommended. If suspicion is MODERATE and the diagnostic evaluation is expected to take > 4 hours, empiric anticoagulation is also warranted. Anticoagulation is NOT recommended empirically if suspicion is LOW.")
71
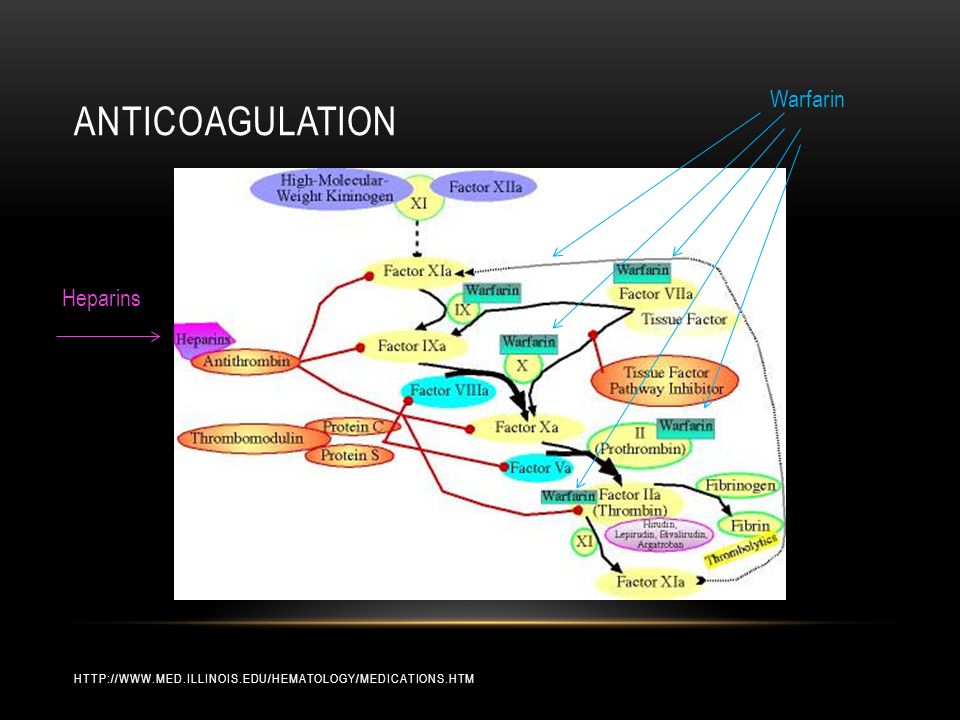
ANticoagulation Warfarin Heparins
72
ANTICOAGULATION – Heparins
Unfractionated Heparin Intravenous Unfractionated Heparin (IV UFH) Subcutaneous Unfractionated Heparin (SC UFH) Low Molecular Weight Heparin (LMWH) Fondaparinux (Arixtra) Unfractionated Heparin Once was the preferred initial treatment (Many studies comparing UFH to no treatment) But LMWH and fondaparinux are the preferred anticoagulants for initial therapy in most cases of acute PE as they confer superior or equivalent outcomes, are more convenient, and are associated with less thrombocytopenia.
 Subcutaneous Unfractionated Heparin (SC UFH) Low Molecular Weight Heparin (LMWH) Fondaparinux (Arixtra) Unfractionated Heparin. Once was the preferred initial treatment (Many studies comparing UFH to no treatment) But LMWH and fondaparinux are the preferred anticoagulants for initial therapy in most cases of acute PE as they confer superior or equivalent outcomes, are more convenient, and are associated with less thrombocytopenia.")
73
ANTICOAGULATION – Unfractionated Heparin (UFH)
Once was the preferred initial treatment Shortest acting anticoagulant Activity can be reversed by protamine sulfate (if major bleeding occurs) Intravenous Unfractionated Heparin (IV UFH) is still preferred in certain situations Dosing (Weight-based or Fixed) Monitoring - activated partial thromboplastin time (aPTT) SC not often used as LMWH, Fondaparinux are more convenient Unfractionated Heparin -Many studies comparing UFH to no treatment Shortest acting anticoagulant Activity can be reversed by protamine sulfate if major bleeding occurs) Intravenous Unfractionated Heparin (IV UFH) is still preferred agent if: Persistent hypotension due to acute PE Increased risk of bleeding Thrombolysis is being considered Severe renal insufficiency (CrCl < 30 ml/min) Concerns about subcutaneous absorption Morbid obesity, anasarca Dosing: Weight based protocol Goal is to achieve therapeutic aPTT within 24 hours Starting bolus of 80 units/kg, followed by infusion at 18 units/kg/hour, Titrate infusion rate every 4-6 hours to goal aPTT Therapeutic aPTT ranges and dose adjustments vary from institution to institution Fixed Dosing - Bolus 5000 units followed by infusion Monitoring- Using activated partial thromboplastin time (aPTT) to measure antithrombotic activity of heparin In most institutions, therapeutic aPTT is times the control aPTT Failing to achieve therapeutic aPTT in first 24 hours associated with higher rate of recurrent DVT or PE aPTT does not always correlate with heparin levels IV UFH Nomograms are often used.
 Intravenous Unfractionated Heparin (IV UFH) is still preferred in certain situations. Dosing (Weight-based or Fixed) Monitoring - activated partial thromboplastin time (aPTT) SC not often used as LMWH, Fondaparinux are more convenient. Unfractionated Heparin -Many studies comparing UFH to no treatment. Shortest acting anticoagulant. Activity can be reversed by protamine sulfate if major bleeding occurs) Intravenous Unfractionated Heparin (IV UFH) is still preferred agent if: Persistent hypotension due to acute PE. Increased risk of bleeding. Thrombolysis is being considered. Severe renal insufficiency (CrCl < 30 ml/min) Concerns about subcutaneous absorption. Morbid obesity, anasarca. Dosing: Weight based protocol. Goal is to achieve therapeutic aPTT within 24 hours. Starting bolus of 80 units/kg, followed by infusion at 18 units/kg/hour, Titrate infusion rate every 4-6 hours to goal aPTT. Therapeutic aPTT ranges and dose adjustments vary from institution to institution. Fixed Dosing - Bolus 5000 units followed by infusion. Monitoring- Using activated partial thromboplastin time (aPTT) to measure antithrombotic activity of heparin. In most institutions, therapeutic aPTT is times the control aPTT. Failing to achieve therapeutic aPTT in first 24 hours associated with higher rate of recurrent DVT or PE. aPTT does not always correlate with heparin levels. IV UFH Nomograms are often used.")
74
ANTICOAGULATION – Low Molecular Weight Heparin
Low Molecular Weight Heparin (LMWH) Recommended for most hemodynamically stable patients with acute PE rather than IV UFH or SC UFH. Anti-Xa activity Formulations and Dosing Enoxaparin (Lovenox) – administered subcutaneously 1mg/kg every 12 hours OR 1.5mg/kg daily Dalteparin – subcutaneous 200 IU/kg once daily Nadroparin – subcutaneously 171 IUs/kg once daily Tinzaparin – subcutaneously 175 IUs/kg once daily Enoxaparin 1mg/kg every 12 hours preferred for patients with cancer, extensive clot burden, actual body weight between kg, BMI bet
 Recommended for most hemodynamically stable patients with acute PE rather than IV UFH or SC UFH. Anti-Xa activity. Formulations and Dosing. Enoxaparin (Lovenox) – administered subcutaneously 1mg/kg every 12 hours OR 1.5mg/kg daily. Dalteparin – subcutaneous 200 IU/kg once daily. Nadroparin – subcutaneously 171 IUs/kg once daily. Tinzaparin – subcutaneously 175 IUs/kg once daily. Enoxaparin 1mg/kg every 12 hours preferred for patients with cancer, extensive clot burden, actual body weight between kg, BMI bet")
75
ANTICOAGULATION – Low Molecular Weight Heparin
LMWH advantages (numerous trials) Lower mortality Fewer recurrent thromboembolic events Less major bleeding Monitoring anti-Xa levels is not necessary for most patients* Greater bioavailability More predictable pharmacokinetics Once or twice daily administration Fixed dosing (without adjustment) Decreased likelihood of thrombocytopenia Monitoring anti-Xa levels with use of LMWH may be warranted in special circumstances: Obesity - Therapeutic anti-Xa levels found if actual body weight is up to 144 kg (enoxaparin) Low body weight - < 45kg women, < 57kg men, might increase risk of bleeding Periodic monitoring of anti-Xa activity is warranted Renal insufficiency No specific dose adjustment - mild to moderate renal insuff (CrCL ml/min) Do not use LMWH if severe renal insufficiency CrCl < 30 ml/min Pregnancy
 Lower mortality. Fewer recurrent thromboembolic events. Less major bleeding. Monitoring anti-Xa levels is not necessary for most patients* Greater bioavailability. More predictable pharmacokinetics. Once or twice daily administration. Fixed dosing (without adjustment) Decreased likelihood of thrombocytopenia. Monitoring anti-Xa levels with use of LMWH may be warranted in special circumstances: Obesity - Therapeutic anti-Xa levels found if actual body weight is up to 144 kg (enoxaparin) Low body weight - < 45kg women, < 57kg men, might increase risk of bleeding. Periodic monitoring of anti-Xa activity is warranted. Renal insufficiency. No specific dose adjustment - mild to moderate renal insuff (CrCL ml/min) Do not use LMWH if severe renal insufficiency CrCl < 30 ml/min. Pregnancy.")
76
ANTICOAGULATION – Fondaparinux
Fondaparinux (Arixtra) Synthetic Factor Xa Inhibitor – catalyzes factor Xa inactivation by antithrombin without inhibiting thrombin Dosing: subcutaneous administration once daily 5 mg for patients < 50 kg 7.5 mg for patients kg 10 mg for patients >100 kg Contraindicated in patients with severe renal insufficiency (CrCl<30ml/min) Routine monitoring of anti-Xa levels is not necessary Fondaparinux Similar effects on clinical outcomes: mortality, recurrent thromboembolism, major bleeding as does IV UFH Advantages over IV UFH: Once or twice daily administration Fixed dosing (no adjustment) Decreased likelihood of thrombocytopenia Has no difference in clinical outcomes compared to patients on LMWH for DVT Burdens and potential side effects are similar Has not been directly compared to LMWH in patients with PE
 Synthetic Factor Xa Inhibitor – catalyzes factor Xa inactivation by antithrombin without inhibiting thrombin. Dosing: subcutaneous administration once daily. 5 mg for patients < 50 kg. 7.5 mg for patients kg. 10 mg for patients >100 kg. Contraindicated in patients with severe renal insufficiency (CrCl<30ml/min) Routine monitoring of anti-Xa levels is not necessary. Fondaparinux. Similar effects on clinical outcomes: mortality, recurrent thromboembolism, major bleeding as does IV UFH. Advantages over IV UFH: Once or twice daily administration. Fixed dosing (no adjustment) Decreased likelihood of thrombocytopenia. Has no difference in clinical outcomes compared to patients on LMWH for DVT. Burdens and potential side effects are similar. Has not been directly compared to LMWH in patients with PE.")
77
ANTICOAGULATION – Warfarin
Oral anticoagulants are most often used for long-term anticoagulation Most oral anticoagulants are Vitamin K antagonists Suppresses production of Vitamin K-dependent clotting factors (II, VII, IX, and X) Warfarin (Coumadin) is the most common and best studied Warfarin is highly effective for preventing recurrent VTE
 Warfarin (Coumadin) is the most common and best studied. Warfarin is highly effective for preventing recurrent VTE.")
78
ANTICOAGULATION – Warfarin Initiation
Warfarin can be initiated on the same day or after heparin or fondaprinux is begun Warfarin should NOT be initiated prior to heparin or fondaparinux Warfarin alone is associated with 3x increase in recurrent PE or DVT Warfarin should be overlapped with heparin or fondaparinux for a minimum of 5 days until the International Normalized Ratio (INR) has been within the therapeutic range ( ) for at least 24 hours Its anticoagulant effect is not realized until the pre-existing factors are cleared from circulation (~ hours) Intrinsic clotting pathway remains intact until ~ 5 days
 has been within the therapeutic range ( ) for at least 24 hours. Its anticoagulant effect is not realized until the pre-existing factors are cleared from circulation (~ hours) Intrinsic clotting pathway remains intact until ~ 5 days.")
79
ANTICOAGULATION – Warfarin
Dosing: Administer Warfarin with initial dose of not more than 5mg per day for first 2 days Use smaller doses in elderly patients Adjust the daily dose according to the INR Rate at which individuals metabolize warfarin varies greatly Required dose can be impacted by multiple variables: Age Concomitant medications Diet

80
ANTICOAGULATION – Warfarin Monitoring
International Normalized Ratio (INR) is test most used to measure effects of warfarin Target INR for acute PE and DVT is 2.5 ( ) INR < 2.0 associated with increased likelihood of recurrent PE or DVT INR monitored daily at first → once every few days until stable dose is achieved → once every 4 weeks Use of Warfarin Nomogram MONITORING warfarin
 is test most used to measure effects of warfarin. Target INR for acute PE and DVT is 2.5 ( ) INR < 2.0 associated with increased likelihood of recurrent PE or DVT. INR monitored daily at first → once every few days until stable dose is achieved → once every 4 weeks. Use of Warfarin Nomogram. MONITORING warfarin.")
81
ANTICOAGULATION – OTHER Anticoagulants
Rivaroxaban (Xarelto) Oral Factor Xa inhibitor Fixed dose Does NOT require monitoring Apixaban (Eliquis) Dabigatrin (Pradaxa) Dabigatrin (Pradaxa) Not yet approved for use with PE or DVT Rivaroxaban (Xarelto) Oral Factor Xa inhibitor Fixed dose Does NOT require monitoring Approved by FDA for acute PE Should not be used if CrCL < 30 ml/min, significant hepatic impairment, or pregnancy Apixaban (Eliquis) orally active direct factor Xa inhibitor used for postoperative prophylaxis of VTE
 Oral Factor Xa inhibitor. Fixed dose. Does NOT require monitoring. Apixaban (Eliquis) Dabigatrin (Pradaxa) Dabigatrin (Pradaxa) Not yet approved for use with PE or DVT. Rivaroxaban (Xarelto) Oral Factor Xa inhibitor. Fixed dose. Does NOT require monitoring. Approved by FDA for acute PE. Should not be used if CrCL < 30 ml/min, significant hepatic impairment, or pregnancy. Apixaban (Eliquis) orally active direct factor Xa inhibitor used for postoperative prophylaxis of VTE.")
82
ANTICOAGULATION – COMPLICATIONS
Bleeding Major bleeding: Intracranial hemorrhage, Retroperitoneal hemorrhage, Bleeding that leads to death, hospitalization, or transfusion Frequency of major bleeding is proportional to number of risk factors LMWH appears to have a lower major bleeding rate than IV UFH Protamine sulfate can be used to reduce clinical bleeding by neutralizing antithrombin activity (LMWH, IV UFH, SC UFH) For fondaparinux – recombinant factor VIIa may be effective Vitamin K and fresh frozen plasma (FFP) can be used to reverse oral vitamin K antagonists Thrombocytopenia Heparin-induced thrombocytopenia (HIT) is a complication of heparin therapy BLEEDING Major bleeding: Intracranial hemorrhage Retroperitoneal hemorrhage Bleeding that leads to death, hospitalization, or transfusion Frequency of major bleeding is proportional to number of risk factors LMWH appears to have a lower major bleeding rate than IV UFH Protamine sulfate can be used to reduce clinical bleeding by neutralizing antithrombin activity LMWH, IV UFH, SC UFH Not for fondaparinux – but recombinant factor VIIa may be effective Vitamin K and fresh frozen plasma (FFP) can be used to reverse oral vitamin K antagonists Thrombocytopenia Heparin-induced thrombocytopenia (HIT) is a complication of heparin therapy HIT is less common with use of LMWH compared to either IV UFH or SC UFH Fondaparinux causes HIT infrequently (if at all)
 For fondaparinux – recombinant factor VIIa may be effective. Vitamin K and fresh frozen plasma (FFP) can be used to reverse oral vitamin K antagonists. Thrombocytopenia. Heparin-induced thrombocytopenia (HIT) is a complication of heparin therapy. BLEEDING. Major bleeding: Intracranial hemorrhage. Retroperitoneal hemorrhage. Bleeding that leads to death, hospitalization, or transfusion. Frequency of major bleeding is proportional to number of risk factors. LMWH appears to have a lower major bleeding rate than IV UFH. Protamine sulfate can be used to reduce clinical bleeding by neutralizing antithrombin activity. LMWH, IV UFH, SC UFH. Not for fondaparinux – but recombinant factor VIIa may be effective. Vitamin K and fresh frozen plasma (FFP) can be used to reverse oral vitamin K antagonists. Thrombocytopenia. Heparin-induced thrombocytopenia (HIT) is a complication of heparin therapy. HIT is less common with use of LMWH compared to either IV UFH or SC UFH. Fondaparinux causes HIT infrequently (if at all)")
83
ANTICOAGULATION – DURATION of Therapy
Risk for Recurrent VTE Bleeding Risk ↑ if recurrent event ↓ If longer duration tx ↓ risk if provoked PE ↓surgical ↑ if longer term therapy Low (0) Moderate (1) High (2+) Longer term therapy reduces the risk of recurrent VTE, but increases the risk of bleeding - look at the risk:benefit ratio. - take into consideration patient preferences. Take into account patient preferences: monitoring, diet, restrictions to activity
 Moderate (1) High (2+) Longer term therapy reduces the risk of recurrent VTE, but increases the risk of bleeding. - look at the risk:benefit ratio. - take into consideration patient preferences. Take into account patient preferences: monitoring, diet, restrictions to activity.")
84
ANTICOAGULATION – DURATION of Therapy
At least 3 months for most patients with a first episode VTE Vitamin K antagonists are preferred over LMWH for long term therapy of PE PE treatment can be for as little as 3 months, sometimes indefinitely Inpatient → outpatient Reversible or temporary risk factor (immobilization, surgery, trauma) → 3 months Unprovoked → 3 months → reassess Recurrent PE → 3 months → reassess Most patients with DVT are treated for 3 months Mostly Outpatient Unprovoked calf DVT or 1st VTE (provoked): 3 months Proximal DVT or 1st unprovoked VTE: 3-6 months Special considerations First episode of PE Reversible or temporary risk factor (immobilization, surgery, trauma)-3 months of warfarin Unprovoked - no identifiable risk factor- Anticoagulate for 3 months → reassess Recurrent PE-Anticoagulate for 3 months → reassess Special considerations :Cancer, Pregnancy DVT: Mostly Outpatient Unprovoked calf DVT or 1st VTE (provoked): 3 months Proximal DVT or 1st unprovoked VTE: 3-6 months Inpatient if: Massive DVT (eg. iliofemoral), w/ PE, Hi risk of bleed with anticoagulation, comorbid conditions Most patients with DVT are treated for 3 months After completing treatment for first unprovoked VTE event: 5 to 15 % risk of VTE recurrence within the first year following discontinuation of anticoagulation VTE provoked by surgery 1% first year; 0.5% thereafter VTE non-surgical 5%; 2.5% Unprovoked VTE 10%; 5% 2nd unprovoked VTE 15%; 7.5% Risk of recurrent VTE ~ 30-50% over next 5-10 years
 → 3 months. Unprovoked → 3 months → reassess. Recurrent PE → 3 months → reassess. Most patients with DVT are treated for 3 months. Mostly Outpatient. Unprovoked calf DVT or 1st VTE (provoked): 3 months. Proximal DVT or 1st unprovoked VTE: 3-6 months. Special considerations. First episode of PE. Reversible or temporary risk factor (immobilization, surgery, trauma)-3 months of warfarin. Unprovoked - no identifiable risk factor- Anticoagulate for 3 months → reassess. Recurrent PE-Anticoagulate for 3 months → reassess. Special considerations :Cancer, Pregnancy. DVT: Mostly Outpatient. Unprovoked calf DVT or 1st VTE (provoked): 3 months. Proximal DVT or 1st unprovoked VTE: 3-6 months. Inpatient if: Massive DVT (eg. iliofemoral), w/ PE, Hi risk of bleed with anticoagulation, comorbid conditions. Most patients with DVT are treated for 3 months. After completing treatment for first unprovoked VTE event: 5 to 15 % risk of VTE recurrence within the first year following discontinuation of anticoagulation. VTE provoked by surgery 1% first year; 0.5% thereafter. VTE non-surgical 5%; 2.5% Unprovoked VTE 10%; 5% 2nd unprovoked VTE 15%; 7.5% Risk of recurrent VTE ~ 30-50% over next 5-10 years.")
85
ANTICOAGULATION – Treatment for DVT
Thrombolytic Therapy and Thrombectomy (percutaneous or surgical) Inferior vena caval filter Thrombolytic Therapy and Thrombectomy (percutaneous or surgical) Controversial since most patients have an uncomplicated course with LMWH or UFH Considered for pts with proximal occlusive DVT associated with significant swelling/symptoms. Inferior vena caval filter Acute VTE with absolute contraindication to anticoagulant therapy Recent surgery Active bleeding Hemorrhagic stroke
 Inferior vena caval filter. Thrombolytic Therapy and Thrombectomy (percutaneous or surgical) Controversial since most patients have an uncomplicated course with LMWH or UFH. Considered for pts with proximal occlusive DVT associated with significant swelling/symptoms. Inferior vena caval filter. Acute VTE with absolute contraindication to anticoagulant therapy. Recent surgery. Active bleeding. Hemorrhagic stroke.")
86
Don’t forget your objective data, your algorithms, your scoring rules…
but sometimes you do also have to use the force.

Similar presentations







 in a deep vein, usually in the legs, which partially or completely.>")








 around valves propagation Virchow’s triad.>")



