Download presentation
Presentation is loading. Please wait.

1
Dr. Adel El Banna M.D Consultant of Cardiac Surgery Head of Cardiac Surgery Department National Heart Institute

2
Can you do Anything?

3
Acute cardiogenic shock is a lethal condition that results in death from myocardial failure, arrhythmia, or combinations of both.

4
Classic Criteria for Diagnosis of Cardiogenic Shock 1. Systemic Hypotension systolic arterial pressure < 80 mmHg 2. Persistent Hypotension at least 30 minutes 3. Reduced Systolic Cardiac Function Cardiac index < 1.8 x m²/min 4. Tissue Hypoperfusion Oliguria, cold extremities, confusion 5. Increased Left Ventricular Filling Pulmonary capillary wedge pressure > 18 mmHg

5
CardiogenicShock Lethal loop

7
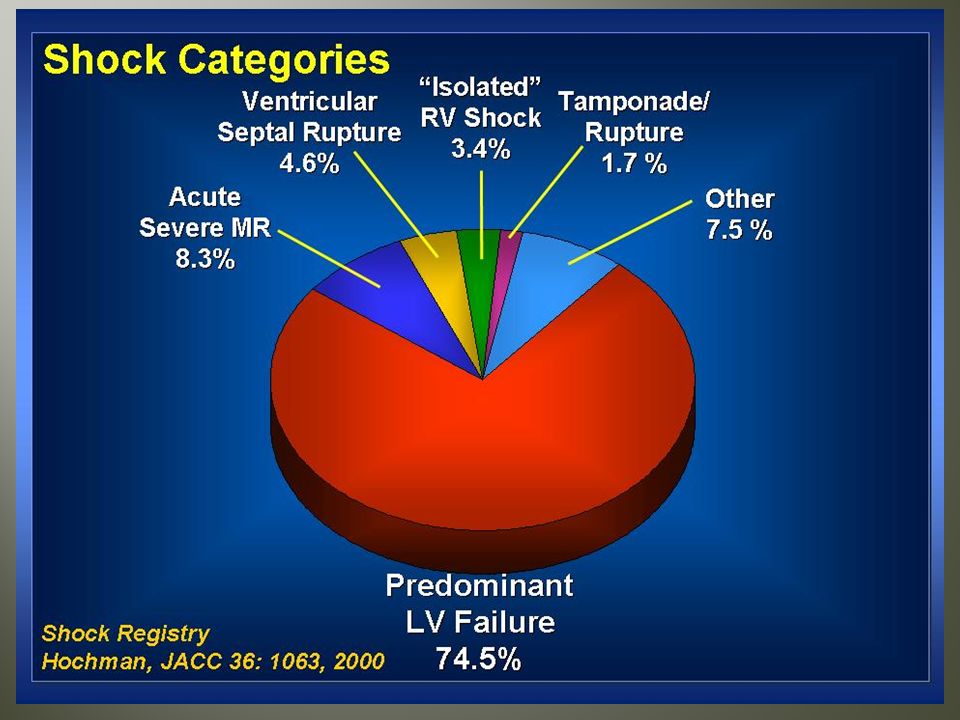
1. Acute myocardial infarction: About 7% of cases may complicate with cardiogenic shock. About 7% of cases may complicate with cardiogenic shock. associated with a high mortality [In-hospital mortality rate is 47% ]. associated with a high mortality [In-hospital mortality rate is 47% ]. The most common causes of death include pump failure or arrhythmia, or both. The most common causes of death include pump failure or arrhythmia, or both. Cardiogenic shock may result in any of this 2 situations:

8
2- Post-cardiotomy ~ 1-2% of cases ( fail to come of pump) ~ 1-2% of cases ( fail to come of pump) high mortality with death rates reaching 80% in the setting of low cardiac output and need for multiple high-dose inotropic drugs. high mortality with death rates reaching 80% in the setting of low cardiac output and need for multiple high-dose inotropic drugs. 3- Inflammatory myocarditis about 2000 case/yr. about 2000 case/yr.

9
Acute Failure Sudden Onset Very Severe Possibly Isolated Reactive Therapy Poor Outcomes Likely reversable Chronic Failure Gradual onset. Graded severity. Several co-morbidities Proactive therapy. Reasonable outcome. Unlikely recoverable. More Challenge

10
Class I 1. IABP is recommended for STEMI patients when cardiogenic shock is not quickly reversed with pharmacological therapy. The IABP is a stabilizing measure for angiography and prompt revascularization. 2. Intra-arterial monitoring is recommended for the management of STEMI patients with cardiogenic shock.

11
1. Early revascularization, either PCI or CABG, is recommended for patients < 75 years old with ST elevation or new LBBB who develop shock unless further support is futile due to patient’s wishes or unsuitability for further invasive care. 2. Fibrinolytic therapy should be administered to STEMI patients with cardiogenic shock who are unsuitable for further invasive care and do not have contraindications for fibrinolysis. 1. Echocardiography should be used to evaluate mechanical complications unless assessed by invasively Class I

12
ACC/AHA Guidelines for Cardiogenic Shock Class IIa 1.Pulmonary artery catheter monitoring can be useful for the management of STEMI patients with cardiogenic shock. 2.Early revascularization, either PCI or CABG, is reasonable for selected patients > 75 years with ST elevation or new LBBB who develop shock 75 years with ST elevation or new LBBB who develop shock < 36 hours of MI and who are suitable for revascularization that is performed < 18 hours of shock. Patients with good prior functional status who agree to invasive care may be selected for such an invasive strategy.

13
Hochman Circ 2003: 107:298 ACC/AHA Guidelines 2004

14
Algorithm for native heart recovery after acute myocardial infarction:

15
Intense antifalure therapy Needs splintage by assisst device No improvement Cardiac Transplantation improved Accepted for surgery Revascularization Mitral repaire Volume reduction surgery No contra indication To surgery

17
Splintage till heart recovers 1- Postcardiotomy cardiogenic shock. 2- Acute myocardial infarction suffering cardiogenic shock in (7% of cases). 3- Acute decompensation of chronic heart failure ( arrhythmia, infarction,infection). 4- Myocarditis. 5- Refractory ventricular arrhythmias. 6- High risk cardiac operations. RECENTLY:
. 3- Acute decompensation of chronic heart failure ( arrhythmia, infarction,infection). 4- Myocarditis. 5- Refractory ventricular arrhythmias. 6- High risk cardiac operations. RECENTLY:.")
18
Extracorporeal 1- Centrifugal pump. 2- Abiomed BVS 5000. 3- Thoratec device. 4- Berlin heart. 5- ECMO ( adult extracorporeal memb. Oxygenator). Intracorporeal 1- Intra Aortic Balloon pump. 2- Thoratec heart mate. 3- Thoratec intracorporeal VAD. 4- Novacor N 1000 PC. 5- Novacor II. 6- Lion heart LVD 2000. 7- Rotary pumps. 8- Cardiac compression device.
. Intracorporeal 1- Intra Aortic Balloon pump. 2- Thoratec heart mate. 3- Thoratec intracorporeal VAD. 4- Novacor N 1000 PC. 5- Novacor II. 6- Lion heart LVD Rotary pumps. 8- Cardiac compression device..")
19
The Intra- Aortic Balloon

20
Intra-aortic balloon pumping is known to be ineffective in severe cardiogenic shock when the systolic aortic pressure cannot be augmented to more than 60 or 70 mm Hg.

21
Contraindications to IABP 1.Significant aortic regurgitation 2.Abdominal aortic aneurysm 3.Aortic dissection 4.Uncontrolled septicemia 5.Uncontrolled bleeding diathesis 6.Severe bilateral peripheral vascular disease uncorrectable by peripheral angioplasty or cross-femoral surgery 7.Bilateral femoral-popliteal bypass grafts for severe peripheral vascular disease Grossman’s 2000

23
Ease of Placement and Operation Hemocompatible No compromise to valve function Improved limb and tissue perfusion Low Hemolysis, bleeding, and stroke rates Restored Hemodynamics Improved outcomes Unloading effect on the left ventricle

24
A self-contained electrohydraulic TAH. Is fully implantable skin. Utilizes a transcutaneous energy transfer (TET) system and a radiofrequency communication (RF Comm) system that allows it to be powered and controlled by signals transmitted across intact skin. AbioCor total artifical heart July 2, 2001
 system and a radiofrequency communication (RF Comm) system that allows it to be powered and controlled by signals transmitted across intact skin. AbioCor total artifical heart July 2,")
25
Systolic blood pressure < 80 mmHg {mean 65mmHg}. Pulmonary capillary wedge >20 mmHg Systemic vasculare resistance > 2100 dynes.sec/cm 5 urine output < 20 ml/hr { on diuretics}. Cardiac output < 2 lit /min /m 2 { on maximum inotropic support}. Right ventricular failure.

26
Clinical right-sided congestive symptoms. Patients with clear documentation of poor right ventricular EF. Fixed pulmonary hypertension above 60 mm Hg systolic. these patients better suited for transplantation.

27
The use of VAD for cardiogenic shock has received a considerable amount of attention with varying degrees of survival based on: 1. Timing of insertion. 2. Age. 3. The presence of comorbidities. 4. Duration of support. 5. Experience of the implanting center and surgeon.

28
Patients successfully bridged to recovery were those that had ancillary procedures done at the time of VAD insertion or shortly thereafter (ie, concomittent PCI or surgery). Patients successfully bridged to recovery were those that had ancillary procedures done at the time of VAD insertion or shortly thereafter (ie, concomittent PCI or surgery).
..")
32
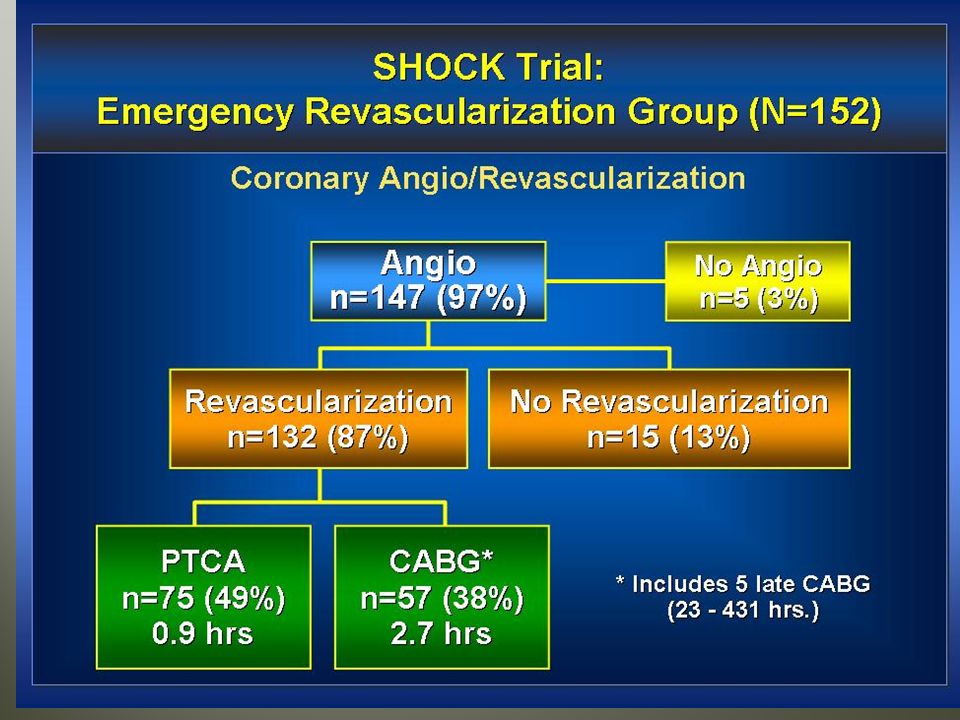
Hochman et al, NEJM 1999; 341:625.

34
Conclusion : Collaboration between cardiac surgery and cardiology, in the form of mechanical support and percutaneous interventions (ie, coronary angioplasty and ablative therapy) can be accomplished with the goal of restoring and maintaining native heart recovery.
 can be accomplished with the goal of restoring and maintaining native heart recovery.")
35
We favor an aggressive approach to promote myocardial recovery, and we utilize the surgical and medical resources to accomplish this end. In the absence of recovery, transplantation of permanent VAD therapy is appropriate.

36
1. Insert an Intra Aortic Balloon. 2. Insertion of an LV assisst device. 3. Perform urgent Myocardial revascularization. 4. Surgical correction of Ischemic complication ie, VSD, Pseudoaneurysm. ie, VSD, Pseudoaneurysm.

37
First Generation Hybrid Cardiac theater

Similar presentations







 VAD (Ventricular assist device)>")


>")













>")
