Download presentation
Presentation is loading. Please wait.

1
Osler Journal Club Dan Munoz and Adnan Malik September 13, 2006

2
Background Population-based case-control studyPopulation-based case-control study Investigating association between ACE inhibitors and abdominal aortic aneurysm (AAA) ruptureInvestigating association between ACE inhibitors and abdominal aortic aneurysm (AAA) rupture Based on animal data suggesting that ACE inhibition may prevent expansion and rupture of AAA’sBased on animal data suggesting that ACE inhibition may prevent expansion and rupture of AAA’s AAA’s are common (4-8% of men > 50 yrs)AAA’s are common (4-8% of men > 50 yrs) Mortality of AAA rupture is 80-90%Mortality of AAA rupture is 80-90%
 ruptureInvestigating association between ACE inhibitors and abdominal aortic aneurysm (AAA) rupture Based on animal data suggesting that ACE inhibition may prevent expansion and rupture of AAA’sBased on animal data suggesting that ACE inhibition may prevent expansion and rupture of AAA’s AAA’s are common (4-8% of men > 50 yrs)AAA’s are common (4-8% of men > 50 yrs) Mortality of AAA rupture is 80-90%Mortality of AAA rupture is 80-90%")
3
Study Outline 15,326 consecutive patients, greater than 65 in age, admitted with primary diagnosis of ruptured or intact AAA over a 10 year period (1992-2002)15,326 consecutive patients, greater than 65 in age, admitted with primary diagnosis of ruptured or intact AAA over a 10 year period (1992-2002) Data derived from four linked administrative databases in Ontario, Canada:Data derived from four linked administrative databases in Ontario, Canada: 1. Ontario Drug Benefit database 2. Canadian Institute for Health Information Discharge Abstract database 3. Ontario Health Insurance Plan database 4. Ontario Registered Persons database

4
Study Outline Analysis looks at association between ACE inhibitor use prior to admission and odds of admission for unruptured vs. ruptured aneurysm (primary diagnosis responsible for admission)Analysis looks at association between ACE inhibitor use prior to admission and odds of admission for unruptured vs. ruptured aneurysm (primary diagnosis responsible for admission) Primary outcome = AAA rupturePrimary outcome = AAA rupture Multivariable analysis performed to adjust for demographics, risk factors for aneurysm rupture, comorbidities, health care access and screeningMultivariable analysis performed to adjust for demographics, risk factors for aneurysm rupture, comorbidities, health care access and screening
Analysis looks at association between ACE inhibitor use prior to admission and odds of admission for unruptured vs. ruptured aneurysm (primary diagnosis responsible for admission) Primary outcome = AAA rupturePrimary outcome = AAA rupture Multivariable analysis performed to adjust for demographics, risk factors for aneurysm rupture, comorbidities, health care access and screeningMultivariable analysis performed to adjust for demographics, risk factors for aneurysm rupture, comorbidities, health care access and screening.")
5
Results Table 1. Baseline characteristics of patients.Table 1. Baseline characteristics of patients. Cases=patients with AAA ruptureCases=patients with AAA rupture Controls=patients with unruptured AAAControls=patients with unruptured AAA Notable for higher rate of imaging, electrocardiography, and cholesterol testing in control groupNotable for higher rate of imaging, electrocardiography, and cholesterol testing in control group Other health measures, comorbidities were similarOther health measures, comorbidities were similar

7
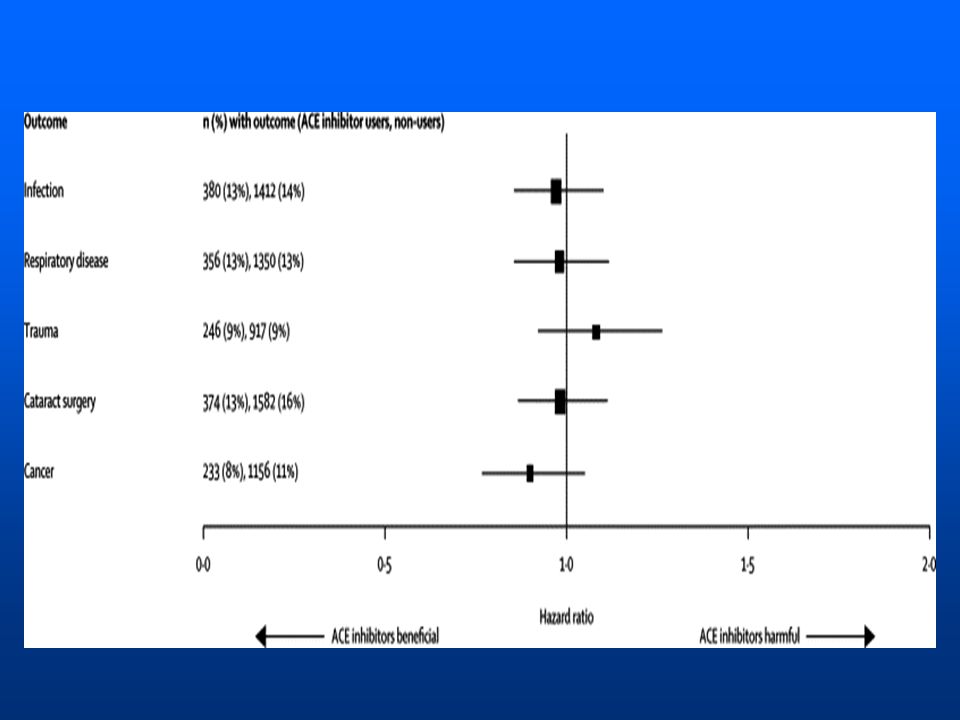
Results Patients receiving ACE-I before admission significantly less likely to present with ruptured aneurysm, OR 0.82 (CI 0.74- 0.90)Patients receiving ACE-I before admission significantly less likely to present with ruptured aneurysm, OR 0.82 (CI 0.74- 0.90) Dosing and specific type of ACE inhibitor did not affect associationDosing and specific type of ACE inhibitor did not affect association Table 2. Other antihypertensives were not associated with lower incidence of AAA ruptureTable 2. Other antihypertensives were not associated with lower incidence of AAA rupture

9
Implications Association between ACE-I use and reduced risk of aortic rupture in elderly population with underlying AA Dx Potentially unique effect of ACE-I among anti-hypertensives in imparting protection against rupture Animal models and this study suggest current role for ACE-I Rx in selected sub- populations, while we await more definitive clinical investigation

10
Strengths of Approach Rarity of condition (M 4-8%, F 0.5-1%, age >50) makes case-control design useful/practical Canadian HC system imparting uniformity of access to hospital care, physician services Rx drug coverage –Use of national utilization databases –Further attempts to control for case-mix: no obvious inherent health status differences between groups Selection of controls –(+) Demonstrated unruptured aneurysms –(-) Question of how coming to attention Findings not overstated –Authors caution: association vs. causation –Direction: non-surgical candidates, trials

11
Weaknesses of Approach Inherent to case-control design –Missed populations Ruptures not making it to medical attention Silent, undiagnosed aortic aneurysms Absence of detailed info on smoking status –Major risk factor for AA enlargement 10 year experience –Uniformity of intervention/technique quality? Definition of ACE-I therapy (Rx record) –Adherence/administration difficult to verify
 –Adherence/administration difficult to verify.")
12
Discussion Points How might this study have been better designed? Do you agree with the case-control model here? What other primary endpoints would be clinically relevant in examining ACE-I benefits/effects? –Rate of enlargement, threshold size, etc. What would be next investigational step? –How might a RCT be feasibly designed?

13
References Hackam D, et al., “Angiotensin-converting enzyme inhibitors and aortic rupture: a population-based case-control study,” Lancet 2006, 368: 659-665 Dr. Jeanne Clark, Division of GIM

14
Taxonomy of Clinical Research Designs Controlled Trials –Non-Randomized –Randomized Other Intervention Studies –Before vs After –External Controls –Historical Controls Prospective Cohort Study – –Concurrent – –Non-Concurrent Case-Control Study Cross-Sectional Study Other / Mixed / ? ExperimentalObservational

15
Comparison of 4 Major Study Designs Estimate PrevalenceFFFA+ Estimate IncidenceB-A+FF Prove CausalityA+B+B-D GeneralizabilityB-A-A-A FeasibilityCBAA Goal or Feature RCTPCS CC X-S RCT=Randomized, controlled trial; PCS=Prospective cohort study; CC=Case-control study; X-S=Cross-sectional study

16
Case Control Studies Ppts selected on disease –Present = cases; Absent = controls –Look back at exposures Etiology –Is head injury more common in pts with Alzheimers? –Is MI more common in women on HRT? Outcomes –Is history of FOB testing less common in people with colon CA?

17
Examples of Exposures & Outcomes in Clinical Research Traits & Behaviors Genetic Variants Infectious Agents Environmental Toxins Medications Surgical Procedures Behavior Modification Screening Programs Death Disease Sub-clinical Indicators of Disease Health-Related Traits Quality of Life Physical Function Costs Exposures Outcomes

Similar presentations





















 ASSISTANT PROFESSOR>")