Download presentation
Presentation is loading. Please wait.

1
Acute Cholangitis

2
Etiology Cholangitis may be acute or chronic
Symptoms result from inflammation, which usually requires at least partial obstruction to the flow of bile Ascending cholangitis or acute cholangitis is a bacterial infection ascending from its junction with the duodenum superimposed on an obstruction of the biliary tree most commonly from a gallstone. It may be associated with neoplasm or stricture Harrison’s Principles of Internal Medicine 17thed

3
Etiology Bile duct obstruction, which is usually present in acute cholangitis, is generally due to gallstones 10–30% of cases are due to other causes: benign stricturing (narrowing of the bile duct without an underlying tumor) postoperative damage or an altered structure of the bile ducts such as narrowing at the site of an anastomosis (surgical connection) various tumors (cancer of the bile duct, gallbladder cancer, cancer of the ampulla of Vater, pancreatic cancer or cancer of the duodenum) Kimura Y, Takada T, Kawarada Y et al. (2007). "Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines". J Hepatobiliary Pancreat Surg14 (1): 15–26
 postoperative damage or an altered structure of the bile ducts such as narrowing at the site of an anastomosis (surgical connection) various tumors (cancer of the bile duct, gallbladder cancer, cancer of the ampulla of Vater, pancreatic cancer or cancer of the duodenum) Kimura Y, Takada T, Kawarada Y et al. (2007). Definitions, pathophysiology, and epidemiology of acute cholangitis. and cholecystitis: Tokyo Guidelines . J Hepatobiliary Pancreat Surg14 (1): 15–26.")
4
Etiology Choledocholithiasis was the most common cause of biliary tract obstruction resulting in cholangitis Over the past 20 years, biliary tract manipulations/interventions and stents have reportedly become more common causes of cholangitis Hepatobiliary malignancies are a less common cause of biliary tract obstruction and subsequent bile contamination Historically, choledocholithiasis was the most common cause of biliary tract obstruction resulting in cholangitis. Over the past 20 years, biliary tract manipulations/interventions and stents have reportedly become more common causes of cholangitis. Hepatobiliary malignancies are a less common cause of biliary tract obstruction and subsequent bile contamination. Lee JG. Diagnosis and management of acute cholangitis. Nat Rev Gastroenterol Hepatol. Aug 4 2009;[Medline].

5
Etiology Most common organisms isolated in bile
Escherichia coli (27%) Klebsiella species (16%) Enterococcus species (15%) Streptococcus species (8%) Enterobacter species (7%) Pseudomonas aeruginosa (7%) Organisms isolated from blood cultures are similar to those found in the bile E coli (59%), Klebsiella species (16%), Pseudomonas aeruginosa (5%), and Enterococcus species (4%) The most common organisms isolated in bile are Escherichia coli (27%), Klebsiella species (16%), Enterococcus species (15%), Streptococcus species (8%), Enterobacter species (7%), and Pseudomonas aeruginosa (7%). Organisms isolated from blood cultures are similar to those found in the bile. The most common pathogens isolated in blood cultures are E coli (59%), Klebsiella species (16%), Pseudomonas aeruginosa (5%), and Enterococcus species (4%).
 Klebsiella species (16%) Enterococcus species (15%) Streptococcus species (8%) Enterobacter species (7%) Pseudomonas aeruginosa (7%) Organisms isolated from blood cultures are similar to those found in the bile. E coli (59%), Klebsiella species (16%), Pseudomonas aeruginosa (5%), and Enterococcus species (4%) The most common organisms isolated in bile are Escherichia coli (27%), Klebsiella species (16%), Enterococcus species (15%), Streptococcus species (8%), Enterobacter species (7%), and Pseudomonas aeruginosa (7%). Organisms isolated from blood cultures are similar to those found in the bile. The most common pathogens isolated in blood cultures are E coli (59%), Klebsiella species (16%), Pseudomonas aeruginosa (5%), and Enterococcus species (4%).")
6
Pathogenesis Main factors in the pathogenesis of acute cholangitis
biliarytract obstruction elevated intraluminalpressure infection of bile A biliary system that is colonized by bacteria but is unobstructed, typically does not result in cholangitis Biliary obstruction diminishes host antibacterial defenses, causes immune dysfunction, and subsequently increases small bowel bacterial colonization The infection can be suppurative in the biliary tract In the presence of gallbladder or common duct stones (CBD), the incidence of bactibilia increases The main factors in the pathogenesis of acute cholangitis are biliary tract obstruction, elevated intraluminal pressure, and infection of bile. A biliary system that is colonized by bacteria but is unobstructed, typically does not result in cholangitis. It is believed that biliary obstruction diminishes host antibacterial defenses, causes immune dysfunction, and subsequently increases small bowel bacterial colonization. Although the exact mechanism is unclear, it is believed that bacteria gain access to the biliary tree by retrograde ascent from the duodenum or from portal venous blood. As a result, infection ascends into the hepatic ducts, causing serious infection. Increased biliary pressure pushes the infection into the biliarycanaliculi, hepatic veins, and perihepaticlymphatics, leading to bacteremia (25-40%). The infection can be suppurative in the biliary tract. The bile is normally sterile. In the presence of gallbladder or common duct stones (CBD), however, the incidence of bactibilia increases.
, the incidence of bactibilia increases. The main factors in the pathogenesis of acute cholangitis are biliary tract obstruction, elevated intraluminal pressure, and infection of bile. A biliary system that is colonized by bacteria but is unobstructed, typically does not result in cholangitis. It is believed that biliary obstruction diminishes host antibacterial defenses, causes immune dysfunction, and subsequently increases small bowel bacterial colonization. Although the exact mechanism is unclear, it is believed that bacteria gain access to the biliary tree by retrograde ascent from the duodenum or from portal venous blood. As a result, infection ascends into the hepatic ducts, causing serious infection. Increased biliary pressure pushes the infection into the biliarycanaliculi, hepatic veins, and perihepaticlymphatics, leading to bacteremia (25-40%). The infection can be suppurative in the biliary tract. The bile is normally sterile. In the presence of gallbladder or common duct stones (CBD), however, the incidence of bactibilia increases.")
7
Infection ascends into the hepatic ducts, causing serious infection
Pathogenesis Bacteria gain access to the biliary tree by retrograde ascent from the duodenum or from portal venous blood as a result of partial obstruction and decreased function of the sphincter of Oddi Infection ascends into the hepatic ducts, causing serious infection Increased biliary pressure resulting from obstruction in the bile duct widens spaces between the cells lining the duct, bringing bacterially contaminated bile in contact with the blood stream Pushes the infection into the biliary canaliculi, hepatic veins, and perihepatic lymphatics, leading to bacteremia (25-40%) Although the exact mechanism is unclear, it is believed that bacteria gain access to the biliary tree by retrograde ascent from the duodenum or from portal venous blood. As a result, infection ascends into the hepatic ducts, causing serious infection. Increased biliary pressure resulting from obstruction in the bile duct widens spaces between the cells lining the duct, bringing bacterially contaminated bile in contact with the blood stream. This pushes the infection into the biliarycanaliculi, hepatic veins, and perihepaticlymphatics, leading to bacteremia (25-40%). The infection can be suppurative in the biliary tract. The bile is normally sterile. In the presence of gallbladder or common duct stones (CBD), however, the incidence of bactibilia increases. Kinney TP (April 2007). "Management of ascending cholangitis". Gastrointest Endosc Clin N Am17 (2): 289–306
 Although the exact mechanism is unclear, it is believed that bacteria gain access to the biliary tree by retrograde ascent from the duodenum or from portal venous blood. As a result, infection ascends into the hepatic ducts, causing serious infection. Increased biliary pressure resulting from obstruction in the bile duct widens spaces between the cells lining the duct, bringing bacterially contaminated bile in contact with the blood stream. This pushes the infection into the biliarycanaliculi, hepatic veins, and perihepaticlymphatics, leading to bacteremia (25-40%). The infection can be suppurative in the biliary tract. The bile is normally sterile. In the presence of gallbladder or common duct stones (CBD), however, the incidence of bactibilia increases. Kinney TP (April 2007). Management of ascending cholangitis . Gastrointest Endosc Clin N Am17 (2): 289–306.")
8
Clinical Features Cholangitis may present as anything from a mild, intermittent, and self-limited disease to a fulminant, potentially life-threatening septicemia Symptoms result from inflammation, which usually is caused by at least partial obstruction to the flow of bile On abdominal examination, the findings are indistinguishable from those of acute cholecystitis Harrison's Principles of Internal Medicine 17th ed, Chapter 305 Sabiston Textbook of Surgery, 18th ed. Schwartz's Surgery 2007

9
Clinical Features The most common presentation is fever with chills, right upper quadrant pain, and jaundice (Charcot's triad), present in about 2/3 of patients The illness may progress rapidly with shock (hypotension, septicemia) and mental status changes, known as Reynolds pentad (e.g., fever, jaundice, right upper quadrant pain, septic shock, and disorientation/lethargy) Harrison's Principles of Internal Medicine 17th ed, Chapter 305 Sabiston Textbook of Surgery, 18th ed. Schwartz's Surgery 2007
, present in about 2/3 of patients. The illness may progress rapidly with shock (hypotension, septicemia) and mental status changes, known as Reynolds pentad (e.g., fever, jaundice, right upper quadrant pain, septic shock, and disorientation/lethargy) Harrison s Principles of Internal Medicine 17th ed, Chapter 305. Sabiston Textbook of Surgery, 18th ed. Schwartz s Surgery")
10
Clinical Presentation
Fever and chills are the most common presentation and are due to cholangiovenous and cholangiolymphatic reflux However, the presentation may be atypical, with little if any fever, jaundice, or pain (occurs most commonly in the elderly, who may have unremarkable symptoms until they collapse with septicemia) Harrison's Principles of Internal Medicine 17th ed, Chapter 305 Sabiston Textbook of Surgery, 18th ed. Schwartz's Surgery 2007
 Harrison s Principles of Internal Medicine 17th ed, Chapter 305. Sabiston Textbook of Surgery, 18th ed. Schwartz s Surgery")
11
Diagnosis Early diagnosis should be made based on clinical signs/symptoms and laboratory findings.

12
Clinical Diagnosis of Acute Cholangitis
Fever Epigastric pain Icteric sclerae BP: 130/70 PR:105/min RR:28/min Slightly distended, tympanitic abdomen, no mass Hypoactive bowel sounds Charcot’s Triad

13
Diagnosis: Laboratory Work-up
The diagnosis of acute cholangitis requires: WBC count - leukocytosis C-reactive protein level Liver function tests – hyperbilirubinemia, elevated ALT and AST Assessment of the severity of the illness requires knowledge of the: Platelet count Blood urea nitrogen Creatinine Prothrombin time (PT) Blood cultures (severity assessment and for selection of antimicrobial drugs) Hyperamylasemia is a useful parameter to identify complications such as choledocholithiasis causing biliary pancreatitis (level 1a).12
 Blood cultures (severity assessment and for selection of antimicrobial drugs) Hyperamylasemia is a useful parameter to identify complications such as choledocholithiasis causing biliary pancreatitis (level 1a).12.")
14
Diagnosis: Imaging Studies
The role of diagnostic imaging in acute cholangitis is: To determine the presence/absence of biliary obstruction The level of the obstruction The cause of the obstruction, such as gallstones and/or biliary strictures Miura et al Flowchart for the diagnosis and treatment of acute cholangitis and cholecystits. Journal of Hepatobiliary and Pancreatic Surgery. 14:27-34.

15
Imaging Studies Ultrasonography – first-line imaging modality
Abdominal CT – first-line imaging modality Endoscopic Retrograde Cholangiography (ERC) Percutaneous Transhepatic Cholangiography (PTC)
 Percutaneous Transhepatic Cholangiography (PTC)")
16
Imaging Studies Ultrasonography Abdominal CT
Endoscopic Retrograde Cholangiography (ERC) Percutaneous Transhepatic Cholangiography (PTC)
 Percutaneous Transhepatic Cholangiography (PTC)")
17
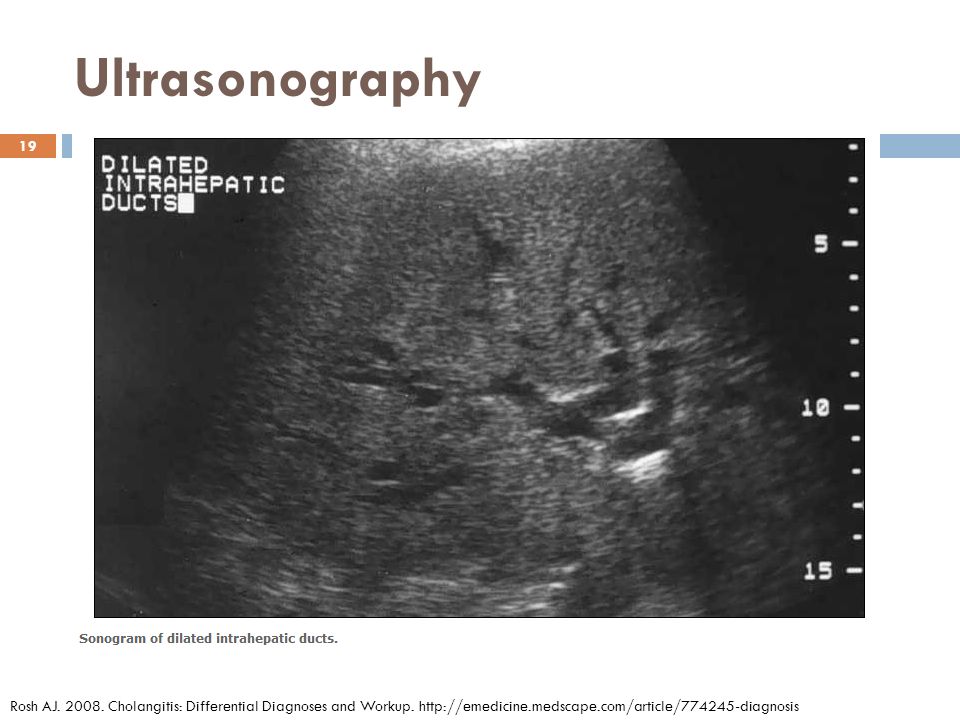
Ultrasonography Transabdominal ultrasonography is the initial imaging study of choice. Performed in all patients suspected of having acute biliary inflammation / infection. Ultrasonography can differentiate intrahepatic obstruction from extrahepatic obstruction and image dilated ducts. In one study of cholangitis, only 13% of CBD stones were observed on ultrasonography, but dilated CBD was found in 64%. A normal sonogram does not rule out acute cholangitis. Advantages to sonography include the ability to be performed rapidly at the bedside, capacity to image other structures (eg, aorta, pancreas, liver), identification of complications (eg, perforation, empyema, abscess), and lack of radiation. Disadvantages to sonography include operator and patient dependence, cannot image the cystic duct, and decreased sensitivity for distal CBD stones. Schwartz’s Priciples of Surgery, 8th ed. Rosh AJ Cholangitis: Differential Diagnoses and Workup.
, identification of complications (eg, perforation, empyema, abscess), and lack of radiation. Disadvantages to sonography include operator and patient dependence, cannot image the cystic duct, and decreased sensitivity for distal CBD stones. Schwartz’s Priciples of Surgery, 8th ed. Rosh AJ Cholangitis: Differential Diagnoses and Workup.")
18
Ultrasonography Advantages to sonography include the ability to be performed rapidly at the bedside, capacity to image other structures (eg, aorta, pancreas, liver), identification of complications (eg, perforation, empyema, abscess), and lack of radiation. Disadvantages to sonography include operator and patient dependence, cannot image the cystic duct, and decreased sensitivity for distal CBD stones. Rosh AJ Cholangitis: Differential Diagnoses and Workup.
, identification of complications (eg, perforation, empyema, abscess), and lack of radiation. Disadvantages to sonography include operator and patient dependence, cannot image the cystic duct, and decreased sensitivity for distal CBD stones. Rosh AJ Cholangitis: Differential Diagnoses and Workup.")
19
Ultrasonography Rosh AJ Cholangitis: Differential Diagnoses and Workup.
20
Imaging Studies Ultrasonography Abdominal CT
Endoscopic Retrograde Cholangiography (ERC) Percutaneous Transhepatic Cholangiography (PTC)
 Percutaneous Transhepatic Cholangiography (PTC)")
21
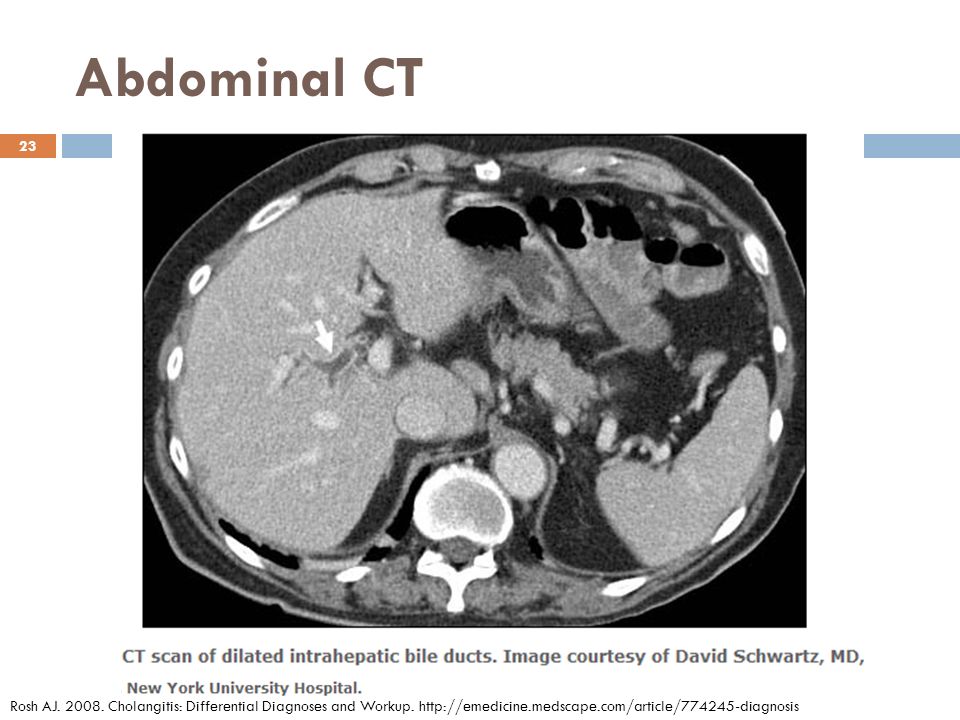
Abdominal CT CT is adjunctive to and may replace ultrasonography.
Spiral or helical CT improves imaging of the biliary tree. CT cholangiography uses a contrast agent that is taken up by the hepatocytes and secreted into the biliary system. Enhances the ability to visualize radiolucent stones and increases detection of other biliary pathology. Dilated intrahepatic and extrahepatic ducts and inflammation of the biliary tree are imaged. Gallstones are poorly visualized with traditional CT scan. Rosh AJ Cholangitis: Differential Diagnoses and Workup.

22
Abdominal CT Advantages of CT include the following:
Other pathologies that are causes or complications of cholangitis (eg, ampullary tumors, pericholecystic fluid, liver abscesses) can be imaged. Pathology that must be distinguished from cholangitis also can be observed (eg, right-sided diverticulitis, papillary necrosis, some evidence of pyelonephritis, mesenteric ischemia, ruptured appendix). Detection of biliary pathology with CT cholangiography approaches that of ERCP. Disadvantages of CT include poor imaging of gallstones, allergic reaction to contrast, exposure to ionizing radiation, and diminished ability to visualize the biliary tree with elevated serum bilirubin level.
 can be imaged. Pathology that must be distinguished from cholangitis also can be observed (eg, right-sided diverticulitis, papillary necrosis, some evidence of pyelonephritis, mesenteric ischemia, ruptured appendix). Detection of biliary pathology with CT cholangiography approaches that of ERCP. Disadvantages of CT include poor imaging of gallstones, allergic reaction to contrast, exposure to ionizing radiation, and diminished ability to visualize the biliary tree with elevated serum bilirubin level.")
23
Abdominal CT Rosh AJ Cholangitis: Differential Diagnoses and Workup.
24
Imaging Studies Ultrasonography Abdominal CT
Endoscopic Retrograde Cholangiopancreatography (ERCP) Percutaneous Transhepatic Cholangiography (PTC)
 Percutaneous Transhepatic Cholangiography (PTC)")
25
Endoscopic Retrograde Cholangiopancreatography (ERCP)
The definitive diagnostic test (criterion standard for imaging the biliary system) Diagnostic and therapeutic Patients with a high clinical suspicion for cholangitis should proceed directly to ERCP. Shows the level and the reason for the obstruction Allows culture of the bile Possibly allows the removal of stones if present Drainage of the bile ducts with drainage catheters or stents. Schwartz’s Priciples of Surgery, 8th ed. Sabiston Textbook of Surgery, 18th ed. Rosh AJ Cholangitis: Differential Diagnoses and Workup.
 Diagnostic and therapeutic. Patients with a high clinical suspicion for cholangitis should proceed directly to ERCP. Shows the level and the reason for the obstruction. Allows culture of the bile. Possibly allows the removal of stones if present. Drainage of the bile ducts with drainage catheters or stents. Schwartz’s Priciples of Surgery, 8th ed. Sabiston Textbook of Surgery, 18th ed. Rosh AJ Cholangitis: Differential Diagnoses and Workup.")
26
Imaging Studies Ultrasonography Abdominal CT
Endoscopic Retrograde Cholangiography (ERC) Percutaneous Transhepatic Cholangiography (PTC)
 Percutaneous Transhepatic Cholangiography (PTC)")
27
Percutaneous Transhepatic Cholangiography (PTC)
Done if ERCP is not available Shows the level and the reason for the obstruction Allows culture of the bile Possibly allows the removal of stones if present Drainage of the bile ducts with drainage catheters or stents. Schwartz’s Priciples of Surgery, 8th ed. Sabiston Textbook of Surgery, 18th ed. Rosh AJ Cholangitis: Differential Diagnoses and Workup.

28
Course of Acute Cholangitis
An ascending bacterial infection in association with partial or complete obstruction of the bile ducts Hepatic bile is sterile, and bile in the bile ducts is kept sterile by continuous bile flow and by the presence of antibacterial substances in bile such as immunoglobulin. Mechanical hindrance to bile flow facilitates bacterial contamination Harrison’s Principle of Internal Medicine , 17th edition 2008

29
Course of Acute Cholangitis
May range from an acute ascending cholangitis, associated with incomplete bile duct obstruction, and ascending bacteria from the duodenum to acute obstructive suppurative cholangitis Current diagnosis & treatment in infectious diseases By Walter R. Wilson, Merle A. Sande, William Lawrence Drew

30
Course of Acute Cholangitis
Non-suppurative Most common and may respond relatively rapidly to supportive measures and to treatment of antibiotics Suppurative The presence of pus under pressure in a completely obstructed ductal system leads to symptoms of severe toxicity- mental confusion, bacteremia and septic shock Harrison’s Principle of Internal Medicine 17th edition 2008

31
Management Antibiotics and supportive treatment
Identify the severity of ascending cholangitis Urgent biliary decompression in some cases ERCP with endoscopic sphincterotomy percutaneous transhepatic route Emergent operation and decompression of the common bile duct with a T tube Townsend: Sabiston Textbook of Surgery, 18th ed.

32
Severity Assessment Based on the response to treatment
Mild (grade I) acute cholangitis Moderate (grade II) acute cholangitis Severe (grade III) acute cholangitis Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines
 acute cholangitis. Moderate (grade II) acute cholangitis. Severe (grade III) acute cholangitis. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines.")
33
Mild (grade I) acute cholangitis
Medical treatment may be sufficient. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines

34
Moderate (grade II) acute cholangitis
Patients with acute cholangitis who do not respond to medical treatment early endoscopic or percutaneous drainage or even emergent operative drainage with a T-tube should be performed A definitive procedure should be performed to remove the cause of the obstruction once the patient is in a stable condition Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines

35
Severe (grade III) acute cholangitis
Patients with acute cholangitis and organ failure Require organ support, such as ventilatory/ circulatory management, and treatment for disseminated intravascular coagulation (DIC) in addition to the general medical management Urgent biliary drainage must be anticipated When the patient is stabilized, urgent (ASAP) endoscopic or percutaneous transhepatic biliary drainage or an emergent operation with decompression of the bile duct with a T-tube should be performed. Definitive treatment of the cause of the obstruction should be considered once the acute illness has resolved. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines
 in addition to the general medical management. Urgent biliary drainage must be anticipated. When the patient is stabilized, urgent (ASAP) endoscopic or percutaneous transhepatic biliary drainage or an emergent operation with decompression of the bile duct with a T-tube should be performed. Definitive treatment of the cause of the obstruction should be considered once the acute illness has resolved. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines.")
36
Diagnosis of acute cholangitis
Launch of medical treatment Severity assessment Mild (Grade I) Moderate (Grade II) Severe (Grade III) Observation Early biliary drainage Urgent Treatment for etiology (Endoscopic treatment, percutaneous treatment, or surgery) Organ support for severe cases Medical treatment Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines
 Moderate. (Grade II) Severe. (Grade III) Observation. Early. biliary. drainage. Urgent. Treatment for etiology (Endoscopic treatment, percutaneous treatment, or surgery) Organ support for severe cases. Medical treatment. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines.")
37
Diagnostic and therapeutic algorithm of patients with ascending cholangitis
Another algorithm..

38
Antibiotics and supportive treatment
Because of the wide range of possible infecting organisms and the possibility of mixed infection, broad-spectrum antibiotic is required, which should be able to cover gram-negative bacilli. Ampicillin together with an aminoglycoside Mezlocillin alone was found more effective and has fewer adverse effects but is ineffective against Pseudomonas Trials comparing various antibiotics have not shown the superiority of any agent A reasonable choice for initial antibiotic treatment of acute cholangitis is ticarcillin and clavulanante (Timentin) or piperacillin and tazobactam (Tazocin). About 90% of patients with acute cholangitis respond to antibiotics and other supportive treatment within 24 to 48 hours Response is usually measured by improvement of clinical signs and body temperature, normalizing liver function tests, and subjective improvement.
 or piperacillin and tazobactam (Tazocin). About 90% of patients with acute cholangitis respond to antibiotics and other supportive treatment within 24 to 48 hours. Response is usually measured by improvement of clinical signs and body temperature, normalizing liver function tests, and subjective improvement. book=surg&part=A2741.")
39
Surgical drainage Stone extraction, T-tube insertion, transhepatic intubation of bile duct or bilio-enteric bypass Has been associated with high morbidity and mortality Age, comorbidities, jaundice, renal failure, acidosis, thrombocytopenia and malignant diseases are risk factors associated with increased perioperative mortality.

40
Endoscopic drainage Endoscopic management of bacterial cholangitis is as effective as surgical intervention. Endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy is safe and the preferred initial procedure for both establishing a definitive diagnosis and providing effective therapy. Harrison‘s Principles of Internal Medicine 17th ed.
 with endoscopic sphincterotomy is safe and the preferred initial procedure for both establishing a definitive diagnosis and providing effective therapy. Harrison‘s Principles of Internal Medicine 17th ed.")
41
Percutaneous transhepatic biliary drainage (PTBD)
Primary aim of emergency PTBD is to establish drainage rather than definitive cholangiography in the acute phase of cholangitis Major advantage of PTBD compared with surgery or endoscopic treatment no need for systemic sedation or anesthesia, which can result in hemodynamic instability and respiratory complications Disadvantage of PTBD includes the need to puncture the liver which may result in serious complications, especially in patients with severe sepsis, clotting derangement and thrombocytopenia. Higher complication rate and an inferior successful rate when compared with endoscopic drainage procedure PTBD is reserved for patients who have strong contraindication for endoscopic intervention (for example, previous Billroth II gastrectomy) and who have failed endoscopic intervention or hilar cholangiocarcinoma.
 and who have failed endoscopic intervention or hilar cholangiocarcinoma. book=surg&part=A2741.")
42
Management Definitive operative therapy should be deferred until the cholangitis has been treated, the patient stabilized, and the diagnosis confirmed. (A must) In the management of acute cholecystitis, Definitive operative therapy should be deferred until the cholangitis has been treated, the patient stabilized, and the diagnosis confirmed. Townsend: Sabiston Textbook of Surgery, 18th ed.
 In the management of acute cholecystitis, Definitive operative therapy should be deferred until the cholangitis has been treated, the patient stabilized, and the diagnosis confirmed. Townsend: Sabiston Textbook of Surgery, 18th ed.")
43
References Fumihiko M. “Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg (2007) 14:27–34. Chi-Leung Liu & Sheung-Tat Fan. “Acute cholangitis”. Copyright © 2001 W. Zuckschwerdt Verlag GmbH. Lee JG. Diagnosis and management of acute cholangitis. Nat Rev Gastroenterol Hepatol. Aug 4 2009;[Medline]. Kimura Y, Takada T, Kawarada Y et al. (2007). "Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines". J Hepatobiliary Pancreat Surg14 (1): 15–26 Miura et al Flowchart for the diagnosis and treatment of acute cholangitis and cholecystits. Journal of Hepatobiliary and Pancreatic Surgery. 14:27-34. Rosh AJ Cholangitis: Differential Diagnoses and Workup. Harrison's Principles of Internal Medicine 17th ed. Sabiston Textbook of Surgery, 18th ed. Schwartz's Surgery 2007 Current diagnosis & treatment in infectious diseases by Walter R. Wilson, Merle A. Sande, William Lawrence Drew
 14:27–34. Chi-Leung Liu & Sheung-Tat Fan. Acute cholangitis . Copyright © 2001 W. Zuckschwerdt Verlag GmbH. book=surg&part=A2741. Lee JG. Diagnosis and management of acute cholangitis. Nat Rev Gastroenterol Hepatol. Aug ;[Medline]. Kimura Y, Takada T, Kawarada Y et al. (2007). Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines . J Hepatobiliary Pancreat Surg14 (1): 15–26. Miura et al Flowchart for the diagnosis and treatment of acute cholangitis and cholecystits. Journal of Hepatobiliary and Pancreatic Surgery. 14: Rosh AJ Cholangitis: Differential Diagnoses and Workup. book=surg&part=A Harrison s Principles of Internal Medicine 17th ed. Sabiston Textbook of Surgery, 18th ed. Schwartz s Surgery Current diagnosis & treatment in infectious diseases by Walter R. Wilson, Merle A. Sande, William Lawrence Drew.")
Similar presentations






>")












