Download presentation
Presentation is loading. Please wait.

1
CHOLINERGIC AGONISTS Joseph De Soto MD, PhD, FAIC

2
Overview Cholinergic drugs are agonists at receptors that bind acetylcholine. Hence, they are agonist at the muscarinic and/or nicotinic receptors. Cholinergic drugs by definition then may stimulate primarily the parasympathetic and somatic nervous systems. A cholinergic medication may also stimulate the sympathetic nervous system if it is an agonist to the N N receptor. Neurotransmission in cholinergic neurons involves six sequential steps: 1) Synthesis, 2) Storage, 3) Release, 4) Binding to receptor, 5) Degradation, and 6) Recycling of acetylcholine.
 Synthesis, 2) Storage, 3) Release, 4) Binding to receptor, 5) Degradation, and 6) Recycling of acetylcholine..")
3
Synthesis of Acetylcholine In the synthesis of acetylcholine we must actively transport choline from the extracellular fluid into the cell. This is the rate limiting step. This transporter can be locked by hemicholine. Choline will react with acetyl coenzyme A (CoA) in the presence of the enzyme Cholineacetyltransferase to form acetylcholine.
 in the presence of the enzyme Cholineacetyltransferase to form acetylcholine..")
4
Storage and Release of Acetylcholine Acetylcholine is placed in and stored into vesicles by active transport which is coupled by proton efflux within the terminus of the axon. ATP and proteoglycan is also stored in the vesicles with acetylcholine. When an action potential arrives at the axon terminus voltage gated Ca ++ channels open with allows the vesicles to fuse with the terminal plasma membrane and release the acetylcholine, proteoglycan and ATP into the synaptic cleft. The botulin toxin which can be found in contaminated foods such as honey can prevent this step.

6
Binding to the Receptor and Degradation of Acetylcholine Acetylcholine once released into the synaptic vesicle diffuses across the synapse and binds to post synaptic receptors. These post synaptic receptors can be either muscarinic or nicotinic. Binding of the receptor leads to a biological response of the cell. Acetylcholine is rapidly degraded due to the enzyme acetylcholinesterase which breaks down acetylcholine to acetate and choline. The choline diffuses back to the presynapse and is reabsorbed to form new acetylcholine.

8
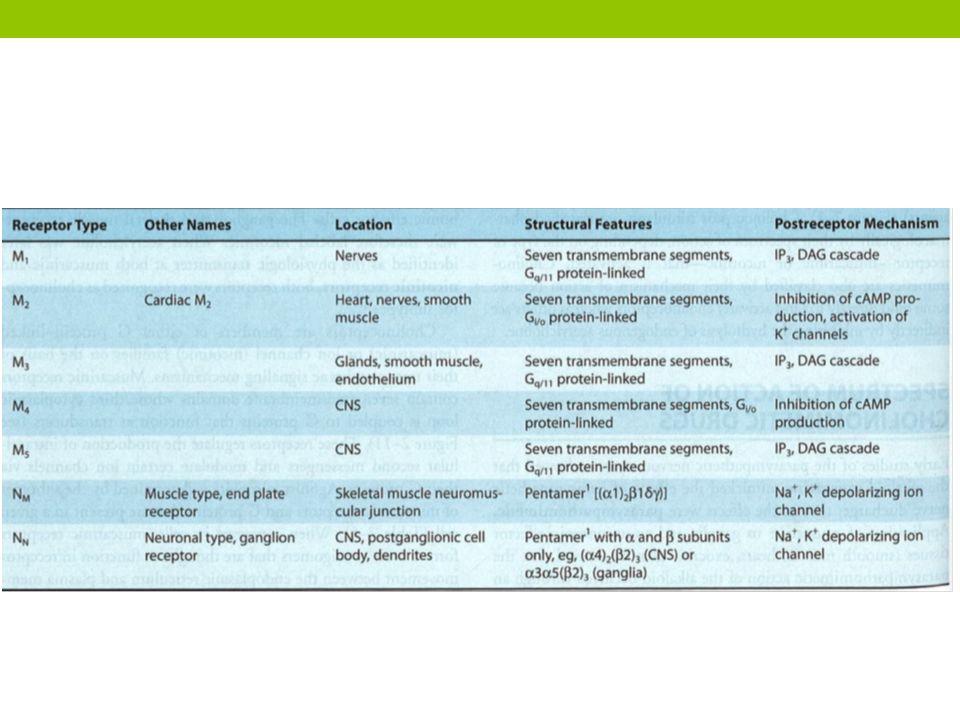
Muscarinic Receptors All three major muscarinic receptors (M1,M2 and M3) are found in the central nervous system with M1 being important for memory. The M1 receptor is found in the CNS, salivary glands, and stomach. The M1 receptor is important for memory. Gq protein utilized The M2 receptor is found in the heart. Slow the heart rate. Gi protein used. The M3 receptor is found in the gut, bronchioles, and sphincters. Contraction of gut muscles, contsriction of airways and relax sphincters. Gq protein used. Drugs that are specific for muscarinic receptors at high levels may bind nicotinic receptors

10
Mechanism of Acetylcholine Signal Transduction M1 & M3 M2 inhibits adenylate cyclase and increase intracellular potassium

11
Nicotinic Receptors Nicotinic receptors will bind acetylcholine and nicotine. The binding of two acetylcholine molecules will cause a conformational change that will allow the entry of sodium channels allowing for the depolarization of the effector cell. Mecamylamine blocks N N and atracurium blocks N M’

12
Direct Acting Cholinergic Agonists Cholinergic agonists mimic the effects of acetylcholine. These cholinergic agonists can be broken down into two groups 1) endogenous and synthetic cholines such as carbachol & bethanechol and 2) natural occurring alkaloids such as nicotine and pilocarpine. Pilocarpine and bethanechol preferentially bind to muscarinic receptors.
 endogenous and synthetic cholines such as carbachol & bethanechol and 2) natural occurring alkaloids such as nicotine and pilocarpine. Pilocarpine and bethanechol preferentially bind to muscarinic receptors..")
13
Acetylcholine Acetylcholine is a quaternary ammonium that cannot penetrate membranes. Because of its short half-life and ability to bind all cholinergic receptors its clinical use is limited. Acetylcholine will decrease the heart rate by reducing the firing at he S.A. node. Acetylcholine will reduce blood pressure by activating M 3 on the cell wall of the endothelial muscle. This allows for the production of nitric oxide from arginine. The nitric oxide then diffuses to stimulate protein kinase G activity, leading to hyperpolarization and smooth muscle relaxation via phosphodiesterase-3 inhibition.

15
Bethanechol Bethanechol is structurally related to acetylcholine though it is NOT hydrolyzed by acetylcholine esterase. It lacks nicotinic activity, but has strong muscarinic activity. This medication is used to treat atonic bladder especially when associated with postpartum, postoperative and when nonobstructive urinary retention is present. This medication stimulates the detrusor muscle of the bladder. Bethanechol causes generalized cholinergic stimulation thus, we may see sweating, decreased blood pressure, abdominal pain, bronchospasm, and flushing.

16
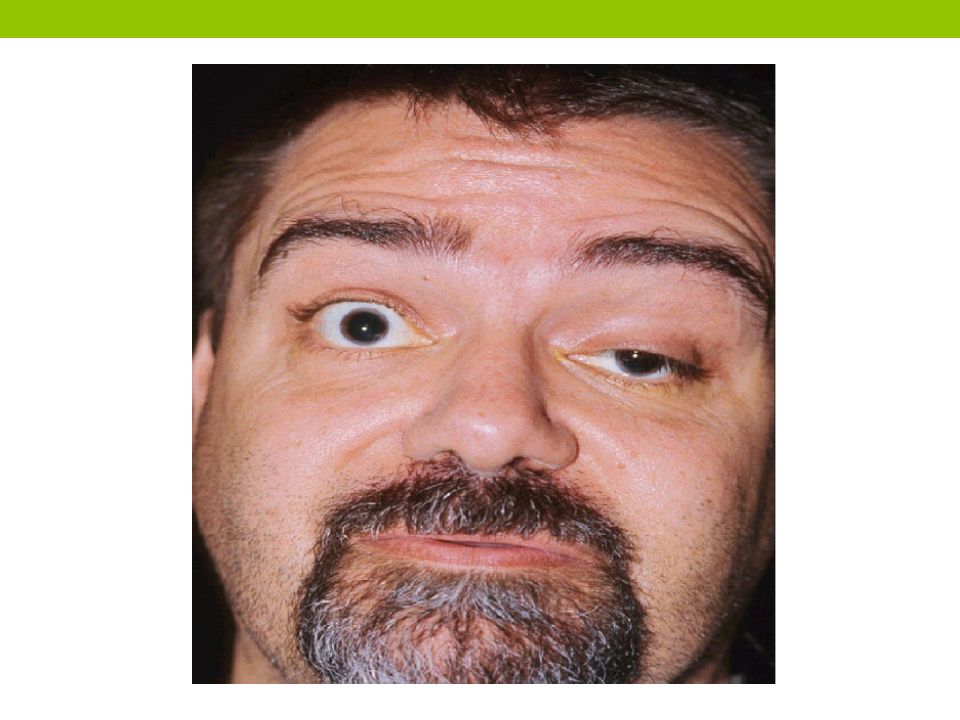
Cholinergic Syndrome

17
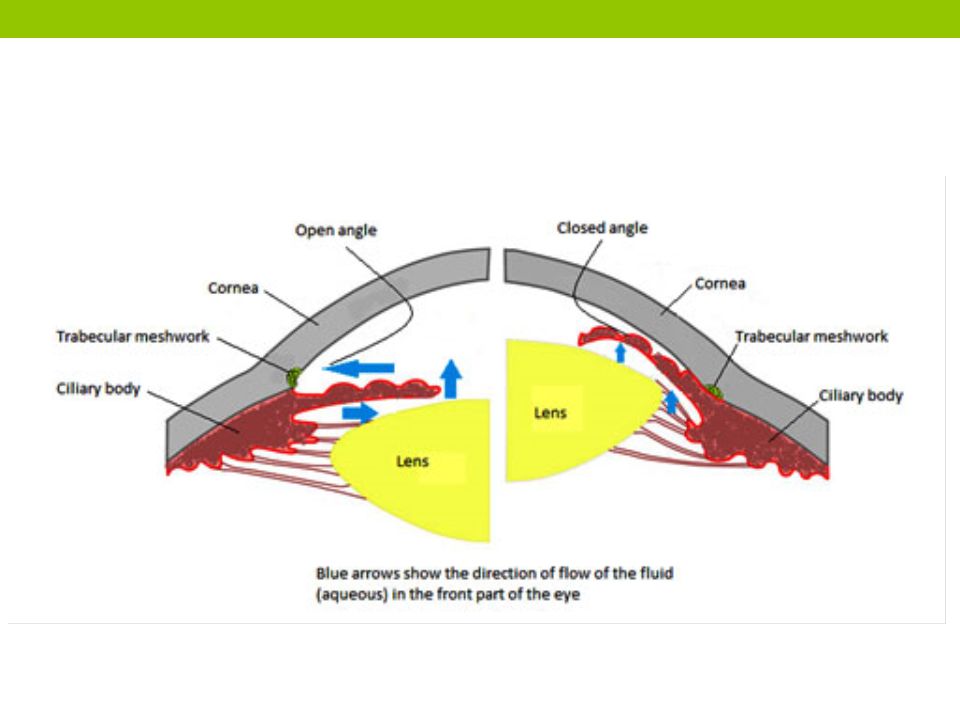
Pilocarpine Pilocarpine is a tertiary amine and is relatively stable compared to acetylcholine. Pilocarpine can penetrate the CNS. Clinically, pilocarpine produces rapid miosis in an eye. This medication also is a potent stimulator of sweat, tears and saliva. Hence, its use in xerostomia from irradiation of the head and Sjogrens syndrome which is characterized by dry mouth and a lack of tears. Pilocarpine is the drug of choice for open-angle and closed angle glaucoma.

19
Anticholinesterase Inhibitors An acetylcholinesterase inhibitor inhibits the breaking down acetylcholine, increasing both the level and duration of action of the neurotransmitter acetylcholine. Acetylcholinesterase inhibitors are classified as reversible, irreversible. They can be used to treat: Glaucoma, Alzheimer's, Myasthenia Gravis, lucid dreaming, postural tachycardia syndrome, Lewy Body Dementia, Parkinson’s, and Autism.

21
Edrophonium Edrophonium is a reversible acetylcholinesterase inhibitor. It prevents breakdown of the neurotransmitter acetylcholine and acts by competitively inhibiting the enzyme acetylcholinesterase predominantly at the neuromuscular junction. Edrophonium is used to differentiate myasthenia gravis from cholinergic crisis and Lambert-Eaton syndrome. Edrophonium will improve myasthenia gravis, do little to Lambert- Eaton Syndrome and worsen cholinergic crisis. The drug has a half life of 7-12 minutes

22
Physostigmine Physostigmine is a competitive acetylcholinesterase inhibitor. It occurs naturally in the West African Calabar bean. Physostigmine is a tertiary amine thus, it can cross the blood–brain barrier, and it is used to treat overdoses of atropine and other anticholinergics. Physostigmine is also used to treat glaucoma, Alzheimer's disease, and delayed gastric emptying. An overdose can cause cholinergic syndrome. Half-life. 15–40 minutes.

23
Neostigmine Neostigmine is an acetylcholinesterase competitive inhibitor. Like Physostigmine it indirectly stimulates both nicotinic and muscarinic receptors. Neostigmine has a quaternary nitrogen therefore it does not enter the CNS, but it does cross the placenta. Its effect on skeletal muscle is greater than that of physostigmine. Neostigmine is used to improve muscle tone in those with myasthenia gravis and to reverse the effects of non-depolarizing muscle relaxants used as anesthesia. Side effects: Headache, blurred vision, vomiting, cramps, bradycardia. Half Life 50-90 minutes

24
Pyridostigmine & Ambenonium Pyridostigmine is a cholinesterase inhibitor and like neostigmine has a quaternary amine and cannot penetrate across the blood–brain barrier. Pyridostigmine is used to treat myasthenia gravis and is used by military use during combat situations as an agent to be given prior to exposure to the nerve agent Soman in order to increase survival. Half- Life 1.8 hours. Ambenonium is another cholinesterase inhibitor used to treat myasthenia gravis. Half life is similar to pyridostigmine.

25
Tacrine, Donepezil, Rivastigmine Patients with Alzheimer’s have a deficiency of cholinergic neurons. Tacrine, Donepezil and Rivastigmine were developed to inhibit CNS acetylcholinesterase. Tacrine (Cognex): was the prototypical acetylcholinesterase inhibitor for the treatment of Alzheimer's disease. It was discontinued for causing liver failure. Donepezil (Aricept): It has an oral bioavailability of 100% and easily crosses the blood–brain barrier. It has a biological half-life of about 70 hours. Rivastigmine (Exelon): Can be given by transdermal patch or orally. Half-life is about 1.4-3.8 hours. Side Effects:nausea and vomiting, decreased appetite and weight loss. These Drugs DO NOT Slow down Alzheimer’s Disease
: was the prototypical acetylcholinesterase inhibitor for the treatment of Alzheimer s disease. It was discontinued for causing liver failure. Donepezil (Aricept): It has an oral bioavailability of 100% and easily crosses the blood–brain barrier. It has a biological half-life of about 70 hours. Rivastigmine (Exelon): Can be given by transdermal patch or orally. Half-life is about hours. Side Effects:nausea and vomiting, decreased appetite and weight loss. These Drugs DO NOT Slow down Alzheimer’s Disease.")
27
Irreversible Anticholinesterase Inhibitors Irreversible anticholinesterase inhibitors are either organophosphates or carbamates. In this country, many insecticides are organophosphates. Organophosphate nerve gases such as Sarin and VX. Poisoning by a nerve agent leads to contraction of pupils, profuse salivation, convulsions, involuntary urination and defecation, and death by asphyxiation due to lung muscle paralysis.

29
Pralidoxime Pralidoxime is used in cases of organophosphate poisoning and is often used with atropine.. After some time though, some organophosphates can develop a permanent bond with cholinesterase, known as aging, where oximes such a pralidoxime cannot reverse the bond. Pralidoxime is only effective in organophosphate toxicity it does not have an effect if the acetylcholinesterase enzyme is carbamylated, as occurs with neostigmine or physostigmine.

30
Toxicology Atropine (belladonna) is given to treat overstimulation of the cholinergic system. atropine is a competitive antagonist of the muscarinic acetylcholine receptors. Atropine in itself may have side effects such as: ventricular fibrillation, or tachycardia, dizziness, nausea, blurred vision, loss of balance, dilated pupils, photophobia, dry mouth, confusion, dissociative hallucinations and excitation. Atropine is contraindicated in patients pre-disposed to narrow angle glaucoma

Similar presentations



















 Sensory.>")




