Download presentation
Presentation is loading. Please wait.

1
AUTOMATED MODES OF VENTILATION: SUPERIOR TO TRADITIONNAL MODES ? François LELLOUCHE, MD, PhD

2
CONFLICTS OF INTEREST - Research contracts with Drager medical (travel expenses for the Canadian study on SmartCare) - Research contracts with Hamilton medical to conduct Intellivent evaluation (Salary of the research assistant) - Program of research on automated ventilation and oxygen therapy: Canadian for Innovation(Fonds des Leaders)/FRSQ grants - President of a R&D compagny that develops automated systems for oxygen therapy and mechanical ventilation
 - Research contracts with Hamilton medical to conduct Intellivent evaluation (Salary of the research assistant) - Program of research on automated ventilation and oxygen therapy: Canadian for Innovation(Fonds des Leaders)/FRSQ grants - President of a R&D compagny that develops automated systems for oxygen therapy and mechanical ventilation")
3
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

4
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

5
Age pyramid US: 1950-2050 Millions of people ♀ ♂ Why automated modes are required ? …. To the first baby-boomers !!

6
Angus JAMA 2000 patients on MV Number of clinicians Age Pyramid Comorbidities

7
Needham CCM 2005

8
Increasing number of patients with prolonged MV (> 96 hours) Cost of MV : 16 billions of $/per year in 2003 60 billions of $/per year in 2020 (projection) Zilberberg, CCM 2008 Data for USA
 Cost of MV : 16 billions of $/per year in 2003 60 billions of $/per year in 2020 (projection) Zilberberg, CCM 2008 Data for USA")
9
Failure of the knowledge transfert Weaning/protective ventilatory strategy Rubbenfeld Respiratory Care 2004 Vilar Acta Anesthesiol Scand 2004 Scale Crit Care Med 2008 Why automated modes are required ?

10
…. To the first baby-boomers !! ARMA Study 6 vs 12 ml/Kg of PBW FAILURE TO IMPLEMENT KNOWLEDGE CHALLENGES FOR HEALTH CARE SYSTEM AUTOMATED SYSTEMS

11
Mandatory Minute Ventilation Evita (Dräger)Hewlett Anesthesia 1977 AutomodeServo (Maquet)Holdt Resp Care 2001 ASVG5 (Hamilton)Laubscher IEEE Biomed Eng 1994 SmartCareEvita XL, V500 (Dräger)Dojat Int J Clin Monit 1992 ASV IntelliventG5 (Hamilton)Brunner 2002 COMMERCIALLY AVAILABLE AUTOMATED MODES
Hewlett Anesthesia 1977 AutomodeServo (Maquet)Holdt Resp Care 2001 ASVG5 (Hamilton)Laubscher IEEE Biomed Eng 1994 SmartCareEvita XL, V500 (Dräger)Dojat Int J Clin Monit 1992 ASV IntelliventG5 (Hamilton)Brunner 2002 COMMERCIALLY AVAILABLE AUTOMATED MODES")
12
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

13
Weaning protocols are efficient (Ely NEJM 1996, Saura ICM 1996, Kollef CCM 1997, Marelich 2000) Weaning protocols are recommended (Mc Intyre Chest 2001, Boles ERJ 2007) …..but many obstacles (Ely AJRCCM 1999, Vitacca ICM 2001) to implement weaning protocols trainings on a regular basis required, problems with new protocols and new practices acceptance… Rationale for weaning automation
 Weaning protocols are recommended (Mc Intyre Chest 2001, Boles ERJ 2007) …..but many obstacles (Ely AJRCCM 1999, Vitacca ICM 2001) to implement weaning protocols trainings on a regular basis required, problems with new protocols and new practices acceptance… Rationale for weaning automation")
14
Control Patient MonitorAlarms Ventilator Control Patient Monitor Alarms Ventilator in PSV Patient Automated Weaning: SmartCare 1) Automated adaptation of PSV level 2) Automated weaning protocol –automatic decrease of the PSV –automatic SBT Ventilator in PSV RR, TV, EtCO 2 Input Automated pressure support Automated Weaning Output Automatic Weaning System SmartCare Processing
 Automated adaptation of PSV level 2) Automated weaning protocol –automatic decrease of the PSV –automatic SBT Ventilator in PSV RR, TV, EtCO 2 Input Automated pressure support Automated Weaning Output Automatic Weaning System SmartCare Processing")
15
Pressure support ventilationPressure support ventilation Automated adaptation of the PS levelAutomated adaptation of the PS level Comfort Zone : 15 < RR < 30 breath/min Tidal Vol > min level, E T CO 2 min level, E T CO 2 < safety limit Automated weaning strategyAutomated weaning strategy Progressive decrease of the PS level Spontaneous breathing test before extubation Recommendation for extubation Dojat et al. Int J Clin Monit Comput 1992 PEEP and FiO 2 are not managed by the system Automated Weaning : SmartCare

16
Minimum level of PS « Automated SBT » EXTUBATIONEXTUBATION Automated reduction of the PSV level Message: « separation from ventilator » PEEP must be 5 cmH 2 O Example of Weaning with «SmartCare »

17
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

18
Intellivent stems from ASV ASV = Pressure controlled and Pressure assisted mode –Automatic transition from controlled to assisted ventilation –Automatic adjustement of RR (Ti/Te) and TV (Pressure, cycling off) for Constant minute ventilation SET BY THE CLINICIAN WITH ASV Minimized work of breathing (based on patient’s respiratory mechanics: time constant and resistance continuously evaluated) Minimized intrinsic PEEP –Based on physiologic Otis and Meade equations –With ASV NO ADJUSTMENT OF PEEP AND FiO 2 INTELLIVENT
 and TV (Pressure, cycling off) for Constant minute ventilation SET BY THE CLINICIAN WITH ASV Minimized work of breathing (based on patient’s respiratory mechanics: time constant and resistance continuously evaluated) Minimized intrinsic PEEP –Based on physiologic Otis and Meade equations –With ASV NO ADJUSTMENT OF PEEP AND FiO 2 INTELLIVENT")
19
Otis, JAP 1950 Mead, JAP 1960

20
Control Patient MonitorAlarms Ventilator Control Patient Monitor Alarms Patient Automated Ventilation : Intellivent 1) Ventilation controller: Automated adaptation of minute ventilation (RR, TV) / EtCO 2 2) Oxygenation controller: Automated adaptation of PEEP and FiO 2 / SpO 2 RR, TV, EtCO 2 Input Automated Ventilation (RR,TV) Automated Oxygenation (PEEP/FiO 2 ) Output Automatic Weaning System Intellivent Processing SpO 2, Heart Lung Index
 Ventilation controller: Automated adaptation of minute ventilation (RR, TV) / EtCO 2 2) Oxygenation controller: Automated adaptation of PEEP and FiO 2 / SpO 2 RR, TV, EtCO 2 Input Automated Ventilation (RR,TV) Automated Oxygenation (PEEP/FiO 2 ) Output Automatic Weaning System Intellivent Processing SpO 2, Heart Lung Index")
21
PEEP limitation - Heart-Lung Index (HLI) HEART vs LUNG: not OK HEART vs LUNG: OK Pulse oxymeter Plethysmogram (mm) Arterial Pressure (mmHg) Airway Pressure (cmH 2 O) Delta PP Delta POP
 HEART vs LUNG: not OK HEART vs LUNG: OK Pulse oxymeter Plethysmogram (mm) Arterial Pressure (mmHg) Airway Pressure (cmH 2 O) Delta PP Delta POP")
22
Adaptive Support Ventilation Still 3 knobs…

23
Intellivent: the NO knobs concept… FULLY AUTOMATIC

24
Intellivent = fully automatic Gender, patient height estimation of the target minute ventilation Clinical situations modifies the target for the controllers Press Start ! Ventilation controller ASV Oxygenation controller EtCO 2 SpO 2

25
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

26
Dojat et al. AJRCCM 1996 Good performances of the system to predict extubation success/failures 38 patients Dojat et al. AJRCCM 2000 Efficiency of the system to maintain the patient in a comfort zone Reduction of time with high P 0.1 56 modifications of PSV/24 hrs vs 1 modification PSV/24 hrs 10 patients Dojat et al. AJRCCM 1992 Maintain of the patients in the comfort zone 95% of time 19 patients INITIAL CLINICAL EVALUATIONS OF SMARTCARE (prototype = NéoGanesh) Bouadma, Lellouche et al. Intensive Care Med 2005 Possibility to ventilate patients with the system during prolonged periods (up to 12 days)-Pilot study for multicenter RCT 42 patients
 Bouadma, Lellouche et al. Intensive Care Med 2005 Possibility to ventilate patients with the system during prolonged periods (up to 12 days)-Pilot study for multicenter RCT 42 patients.")
27
1 st Multicenter Randomized Study Objective of the study Automated weaning Usual protocolized weaning VS Primary end point: Weaning time (inclusion first extubation)
")
28
Lellouche et al, AJRCCM 2006,174:894-900

29
WEAN pilot study Co-PI: K.Burns/F.Lellouche RCT PILOT/ FEASABILITY SmartCare vs written weaning protocols 8 Centers Primary outcome acceptance of weaning protocols

30
OUTCOME DATA VariablesProtocol Weaning (n=43) Automated Weaning (n=51) p-value Time to first extubation, days median (25-75) 4 (2-12)3 (2-5)0.02 Time to first successful extubation, days median (25-75) 5 (3-19)4 (2-7)0.10 Reintubation, n (%) 11 (25.5%)9 (17.7%)0.35 Patients with prolonged ventilation (>21 days), n (%) 6 (18.2%)00.01 Ever had tracheostomy, n (%) 15 (34.9%)8 (16%)0.04 Total duration of intubation, days median (25-75) 10.5 (8, 17.5)12 (6, 25)0.37 Duration of ICU stay, days median (25-75) 9 (5, 25)7 (5, 14)0.13 Duration of Hospitalization, days median (25-75) 31.5 (16. 49.5)22 (14, 33)0.19 ICU death, n (%) 9 (20.9%)9 (17.7%)0.69 Feasibility for a larger RCT ?......
22 (14, 33)0.19 ICU death, n (%) 9 (20.9%)9 (17.7%)0.69 Feasibility for a larger RCT")
31
Automated weaning (SmartCare) vs local weaning protocols in post-surgical patients Randomized Controlled Trial Post-op patients with MV > 9 hours 300 patients included 94±144 hours (SmartCare) 118±165 hours (Protocols) (P=0.12)
 vs local weaning protocols in post-surgical patients Randomized Controlled Trial Post-op patients with MV > 9 hours 300 patients included 94±144 hours (SmartCare) 118±165 hours (Protocols) (P=0.12)")
32
Rose Intensive Care Medicine 2008 Randomized Controlled Trial Medical patients 102 patients included

33
Schadler, ATS 2009 Lellouche, AJRCCM 2006 In the context of increasing gap between needs and supply to manage patients on MV, both studies are positive : Better (or same outcome) with less human interventions
 with less human interventions")
34
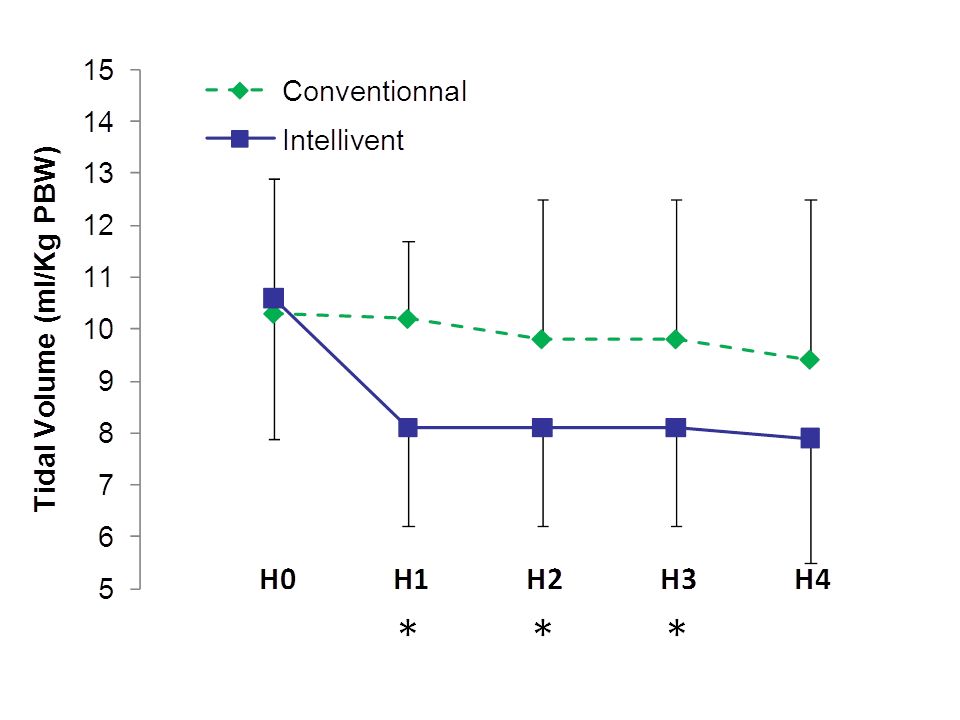
EVALUATION OF INTELLIVENT = FULLY AUTOMATIC MECHANICAL VENTILATION Feasibility study Does the system can safely manage stable patients after cardiac surgery ? Does the system reduce the workload ? Context: recent data (from cardiac surgery database) showing the need to reduce tidal volume after cardiac surgery (prophylactic protective ventilation…)
 showing the need to reduce tidal volume after cardiac surgery (prophylactic protective ventilation…).")
35
Non parametric logistic regression Impact of tidal volumes even in patients with normal lungs 3434 patients after CABG or valve surgery Multivariate analysis High tidal volumes after cardiac surgery are independant risk factors for - organ dysfunction - ICU Length of stay Lellouche et al ATS 2010

36
Cardiac surgery = interesting to evaluate a fully automated system Dynamic clinical condition Within 2-4 hours – Temperature 35˚C 37˚C (↗CO 2 production) – FiO 2 70 40-30% – Controlled assisted ventilation Workload related to mechanical ventilation settings: – Adjustment of minute-ventilation – PEEP/FiO 2 weaning – Switch to PSV
 – FiO 2 70 40-30% – Controlled assisted ventilation Workload related to mechanical ventilation settings: – Adjustment of minute-ventilation – PEEP/FiO 2 weaning – Switch to PSV")
37
Criteria for Consent SURGERY Inclusion criteria + Exclusion criteria - Consent ICU admission Connection to a G5 ventilator Settings by the anesthesiologist 15 minutes Intellivent group Automated ventilation Modified G5 Control group Protocolized Ventilation G5 : SIMV+PSV Randomization 4 hours - Hemodynamic stability 1. < 3 red-cell Tf units within last 15 min 2. Epi or norepinephrine below < 1 mg/h 3. Bleeding <100 ml within last 15 min - No anuria - Unexpected surgical procedure - Major complication during surgery - Early extubation expected (< 1 hour) - Broncho-pleural fistula - Study ventilator not available Inclusion Criteria Exclusion Criteria Study design Data from the ventilator recorded Timing of the interventions Time with optimal/non optimal ventilation
 - Broncho-pleural fistula - Study ventilator not available Inclusion Criteria Exclusion Criteria Study design Data from the ventilator recorded Timing of the interventions Time with optimal/non optimal ventilation.")
38
RESULTS - 90 consent signed Delayed surgery (morning to afternoon cases) Surgery postponed (emergent cases) Hemodynamic instability at ICU arrival 60 patients included from 07/2009 to 12/2009. ALL THE PATIENTS COMPLETED THE STUDY. 1 patient needed re-operation for massive bleeding 1 hour after the randomization (Intellivent group).. Duration of the study (min): Control group Intellivent group P value 194 + 43 207 + 47 0.24
.. Duration of the study (min): Control group Intellivent group P value")
40
RESULTS: MAIN OUTCOME % n Number of manual settings 148 5 Control arm Intellivent arm Control arm Intellivent arm Optimal ventilation (TV < 10ml/Kg of PBW, Pressure < 30, SpO 2, EtCO 2 ) * *
 * *")
41
Why automated modes are required ? SmartCare: automated adjustment of pressure support, automated weaning Intellivent: automated mechanical ventilation Clinical evaluation SmartCare Intellivent Conclusion: even equivalent would be worth….. PLAN

42
Computers in ICU: panacea or plague ? East TD, Respiratory Care 1992

44
Conclusion: Even results equivalent to traditionnal modes would be worth….. in the demographic context Several studies demonstrate positive results to reduce the duration of mechanical ventilation and potential for workload reduction With…first generation systems More evaluation required (Intellivent …) Room for improvement in the next years AUTOMATED MODES OF VENTILATION: SUPERIOR TO TRADITIONNAL MODES ? AUTOMATED MODES OF VENTILATION: SUPERIOR TO HUMAN SETTINGS ?
 Room for improvement in the next years AUTOMATED MODES OF VENTILATION: SUPERIOR TO TRADITIONNAL MODES . AUTOMATED MODES OF VENTILATION: SUPERIOR TO HUMAN SETTINGS .")
45
We should accept that automated systems could be superior to humans for specific tasks…

46
THANKS ! PA Bouchard C Bouchard MC Ferland P Dubé ….

Similar presentations

 for severe sepsis and septic shock treatment>")





 Trial>")











