Download presentation
Presentation is loading. Please wait.

1
GIORGOS - GRIGORIS KARACHALIOS Orthopaedic Surgeon Director of Arthroscopic Surgery Dpt Director of Arthroscopic Surgery Dpt Iatriko Kentro Athinon P.Falirou P. Faliro, Athinai, Hellas. P. Faliro, Athinai, Hellas. GLENOID FRACTURES : ARTHROSCOPIC TREATMENT

2
Confusing literature Complex anatomy and function. Complex anatomy and function. There is no generally accepted classification ( Euler & Ruedi, Goss, Ideberg, Thompson, Zdravkovic & Damholt ). There is no generally accepted classification ( Euler & Ruedi, Goss, Ideberg, Thompson, Zdravkovic & Damholt ). The decision on treatment is mainly based on personal experience, since these are rare. The decision on treatment is mainly based on personal experience, since these are rare. Very often indicators of major trauma – the # is often neglected Very often indicators of major trauma – the # is often neglected
. There is no generally accepted classification ( Euler & Ruedi, Goss, Ideberg, Thompson, Zdravkovic & Damholt ). The decision on treatment is mainly based on personal experience, since these are rare. The decision on treatment is mainly based on personal experience, since these are rare. Very often indicators of major trauma – the # is often neglected Very often indicators of major trauma – the # is often neglected.")
3
Epidemiology 5% of all fractures to the shoulder girdle 5% of all fractures to the shoulder girdle 3% of all injuries to the shoulder girdle 3% of all injuries to the shoulder girdle 0.4 – 1% of all fractures 0.4 – 1% of all fractures Mean age 35 - 45 years

4
One per 3000 operated fractures ~ 10% of glenoid fractures internal fixation

5
Scapular fractures classification Intra-articular - extra-articular Intra-articular - extra-articular Body and spine 50% glenoid neck 25% glenoid cavity 10% acromion 7% coracoid 7% Body and spine 50% glenoid neck 25% glenoid cavity 10% acromion 7% coracoid 7%

6
intra-articular Ideberg intra-articular Ideberg

7
Glenoid fossa Goss

8
Types II through V : closed reduction under anaesthesia ALWAYS unsuccessful. Late improvement. 75% good results by early mobilization. European literature more aggressive Types II through V : closed reduction under anaesthesia ALWAYS unsuccessful. Late improvement. 75% good results by early mobilization. European literature more aggressive

9
Type I to be distinguished from 1. Bony Bankart lesion 1. Bony Bankart lesion 2. Type II joint surface < glenoid neck 2. Type II joint surface < glenoid neck

10
Mechanism of dislocation Mechanism of dislocation sometimes redislocation after reduction sometimes redislocation after reduction

11
risk : Instability ( late dislocation or subluxation ) Joint degeneration
 Joint degeneration")
12
TREATMENT ? TREATMENT ? TARGET retain congruity of the articular surface TARGET retain congruity of the articular surface stability of the joint stability of the joint

13
indications for internal fixation indications for internal fixation displacement > 10 mm. & fragment > ¼ of the glenoid displacement > 10 mm. & fragment > ¼ of the glenoid internal fixation ( De Palma ) internal fixation ( De Palma ) fragment > ¼ of the glenoid & instability internal fixation ( Rockwood ) fragment > ¼ of the glenoid & instability internal fixation ( Rockwood )
 internal fixation ( De Palma ) fragment > ¼ of the glenoid & instability internal fixation ( Rockwood ) fragment > ¼ of the glenoid & instability internal fixation ( Rockwood ).")
14
indications for internal fixation indications for internal fixation Type I fracture ( Ideberg ) > 21% of the length of the glenoid ( av. 26,2 % in his pts ) One fragment Step > 2 mm No neurological deficit Fragment ‘s size 27 % Sugaya 2005 Tauber 2008
 One fragment Step > 2 mm No neurological deficit Fragment ‘s size 27 % Sugaya 2005 Tauber")
15
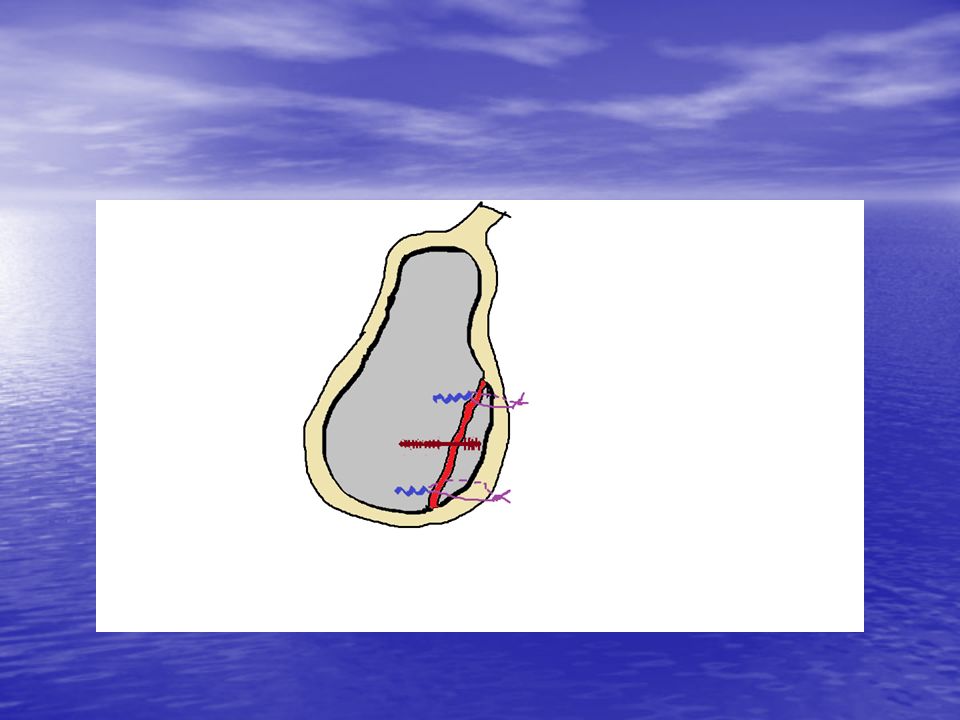
indications for internal fixation indications for internal fixation ( A x 96,5% - B ) / A x 100 fragment > 21% of the length of the glenoid ( av. width 6.8 mm ) fragment > 21% of the length of the glenoid ( av. width 6.8 mm ) resecting a fragment > 6,8 mm and refixing the capsular-ligamentous complex to the glenoid defect, creates instability and reduces the ext. rotation Itoi 2000 resecting a fragment > 6,8 mm and refixing the capsular-ligamentous complex to the glenoid defect, creates instability and reduces the ext. rotation Itoi 2000 21%
 fragment > 21% of the length of the glenoid ( av. width 6.8 mm ) resecting a fragment > 6,8 mm and refixing the capsular-ligamentous complex to the glenoid defect, creates instability and reduces the ext. rotation Itoi 2000 resecting a fragment > 6,8 mm and refixing the capsular-ligamentous complex to the glenoid defect, creates instability and reduces the ext. rotation Itoi %.")
16
open reduction and internal fixation open reduction and internal fixation failure 10 % failure 10 % complications 10% Schandelmaier 2002 complications 10% Schandelmaier 2002 good- excellent functional outcome 82 % good- excellent functional outcome 82 % anatomic reduction 89 % Mayo 1998 anatomic reduction 89 % Mayo 1998 implant impingement - loosening implant impingement - loosening neural injury infection stiffness neural injury infection stiffness

17
potential advantages of arthroscopic fixation Initial diagnostic arthroscopy to exclude / assess associated injuries Reduced soft tissue damage ( particulary of the subscapularis tendon) Overall lower postop morbidity
 Overall lower postop morbidity")
18
the arthroscopic assessment, offers : > of C - arm > of C - arm Confirmation of the reduction … … and the stability of the joint

19
Attempts of arthroscopic fixation using : Suture anchors Percutaneous wire fixation Screw fixation

20
Sugaya 2005

21
Bauer 2006

25
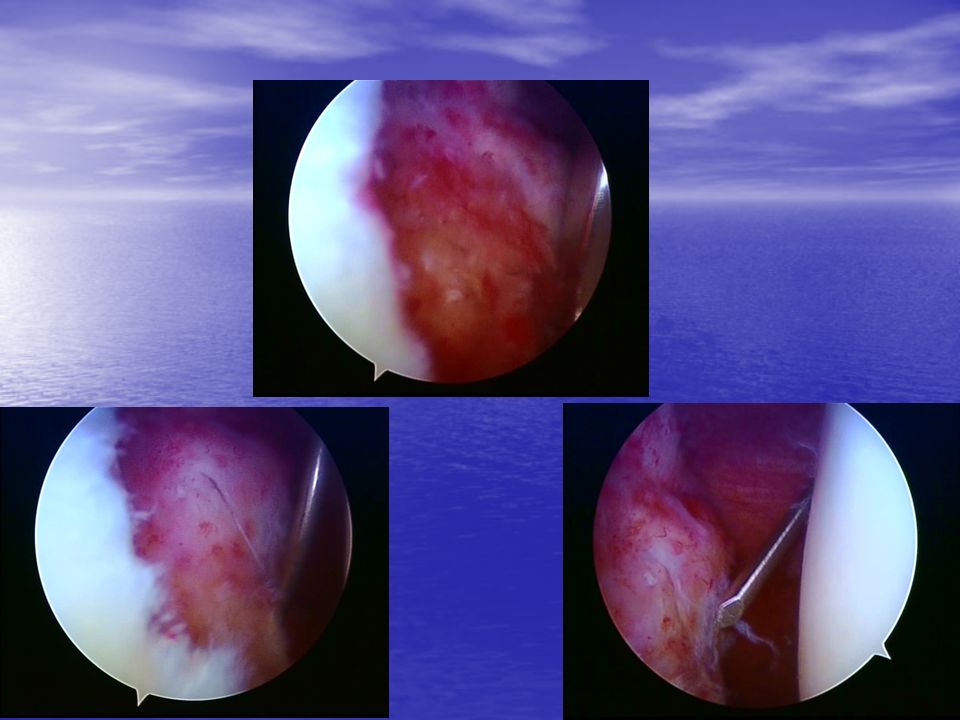
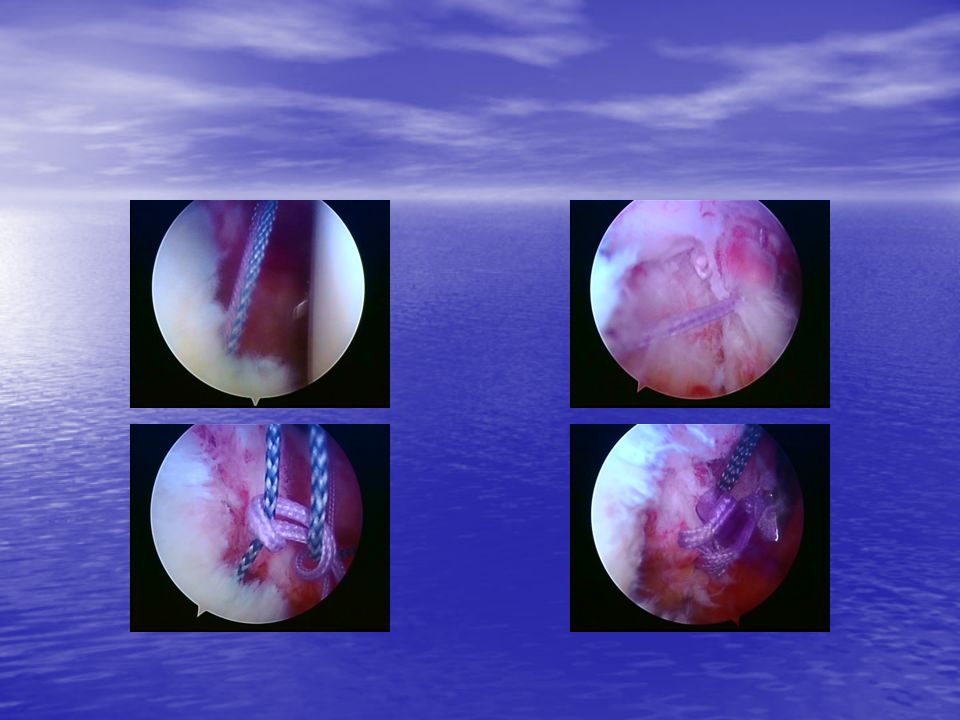
assesment 1 2 3 Assesement of the injury and mobility of the fragment

26
4 5 6 7 mobilizationdebridement

27
8 9 10 11 reduction Temporary fixation by k-wire

28
average glenoid length : 35 mm average glenoid width : 25 mm average glenoid length : 35 mm average glenoid width : 25 mm ACUTRAK – ACUMED tapered cannulated cannulated HEADLESS HEADLESS self-taping self-taping usually length of 25 – 30 mm is adequate usually length of 25 – 30 mm is adequate length – instrumentation ??? Arthroscopic use

29
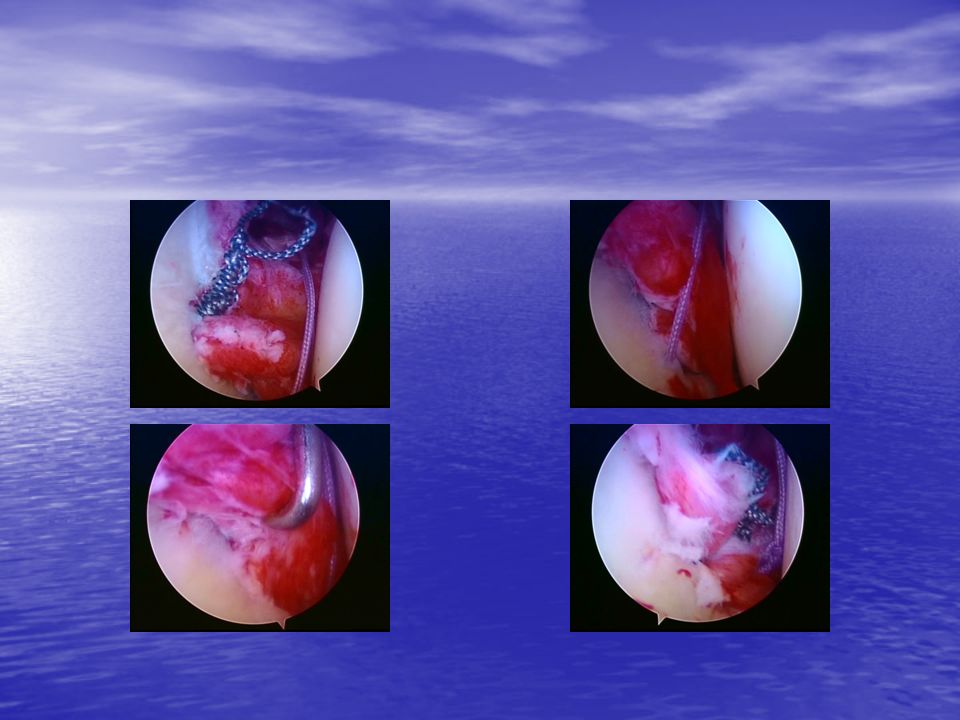
12 13 drilling Screw placement

33
Assesement of the injury and mobility of the fragment

34
reduction

35
insertion of two screws – at the proximal and distal edges of the fractures -

36
Suture passing around the bony element of the fragment and reduction - temporary fixation by a guide K-wire, before the knot tying

37
Knot tying

38
Self – tapping Threaded head Longer pitch of the distal threads Smooth proximal section 10/10 k-wire Barouk screw DePuy

39
Drilling screw placement

40
Check of reduction Check of screw impingement posterior portal anterior portal

44
displacement

45
meticulus mobilization

46
bioabsorbable “ anchor “ transosseous suture

47
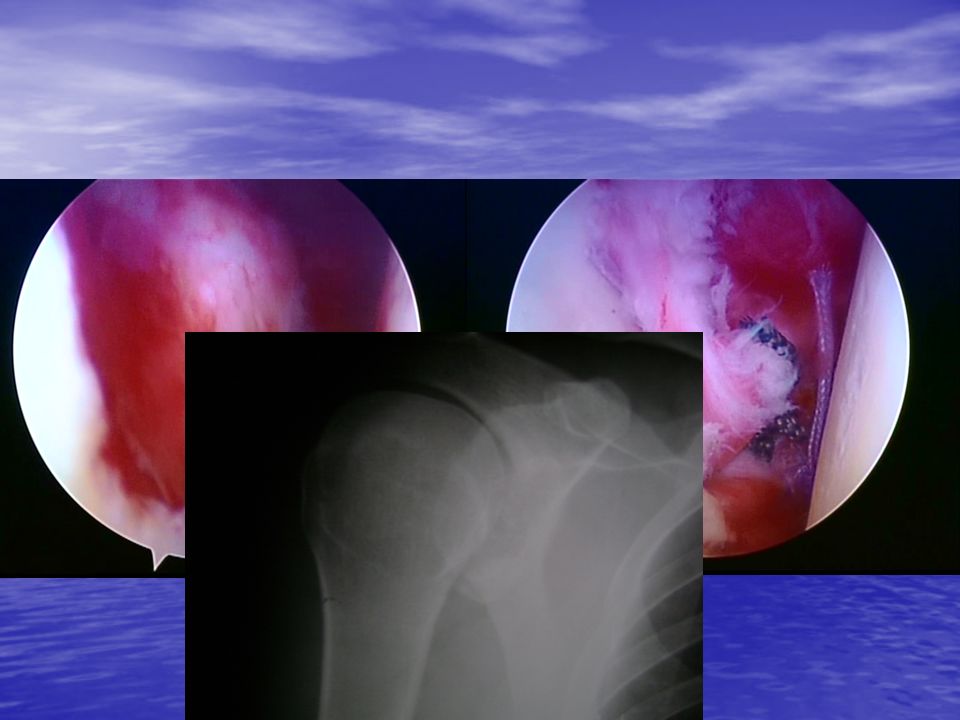
screw ( Barouk – DePuy ) check
 check")
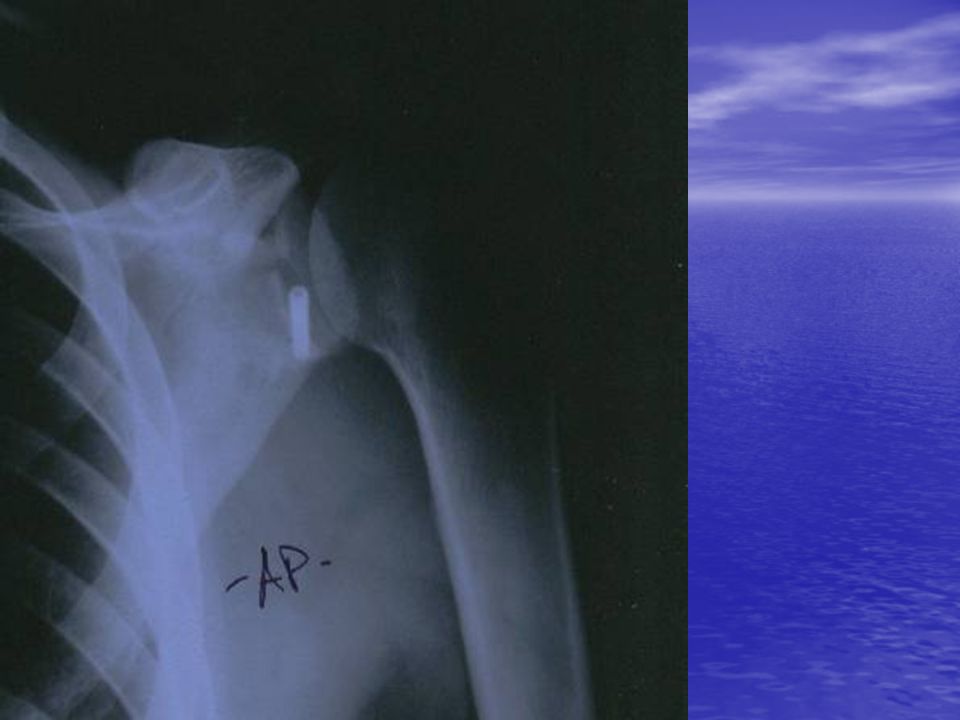
48
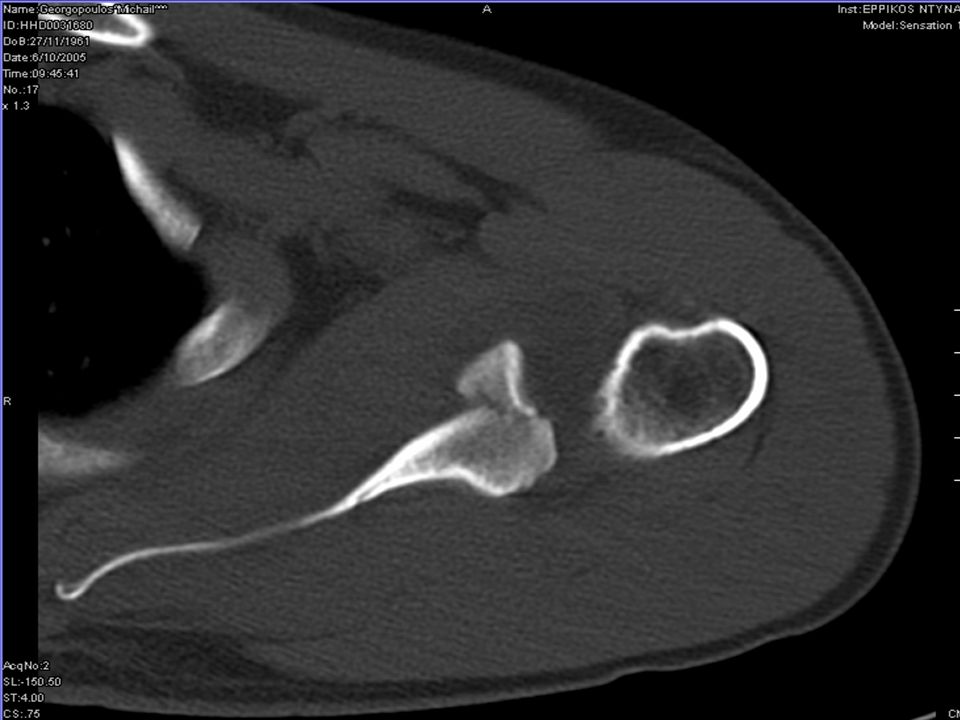
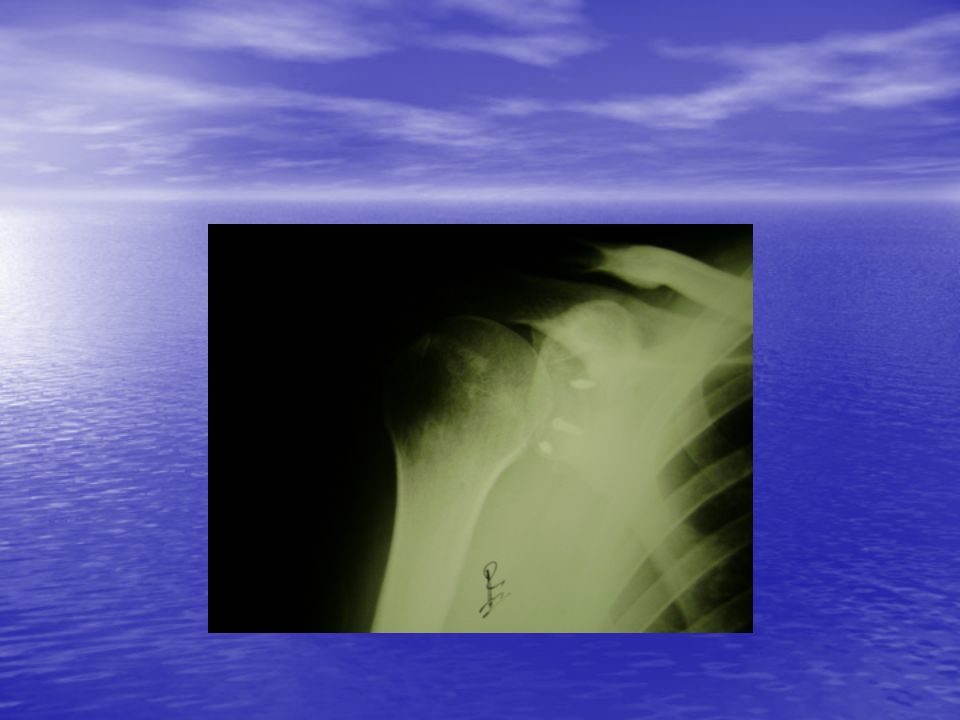
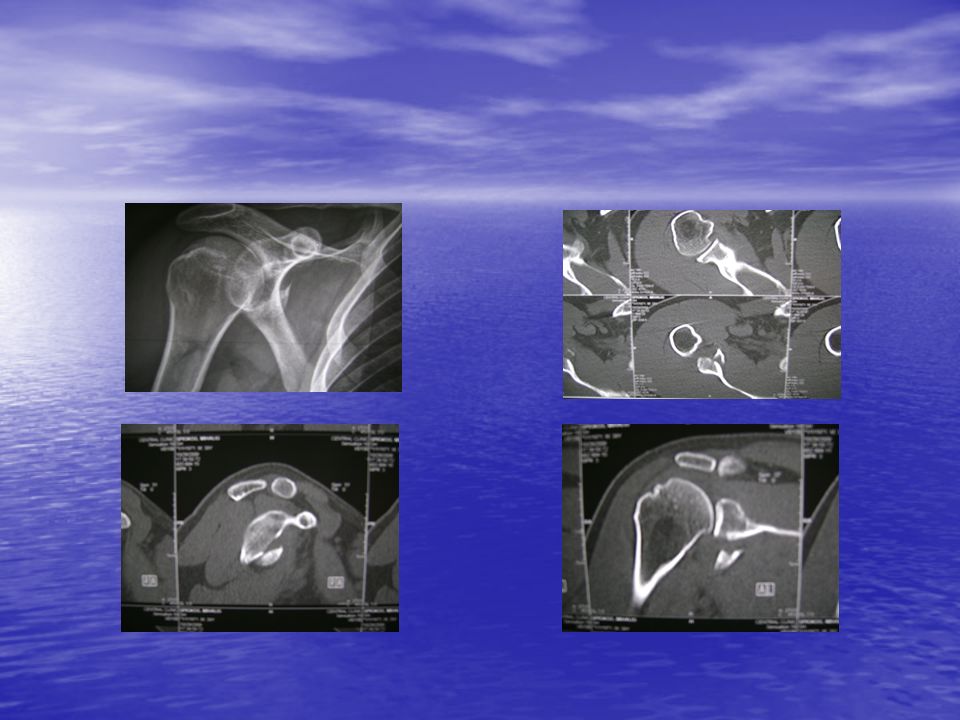
Male, 47, r shoulder

53
What was the problem ? Probably the orientation of the fragment : upper edge bellow 3 ‘ clock Longer distance Higher risk Difficult reduction

54
Ευχαριστώ και καλή σας ημέρα Thank you and … have a nice day

55
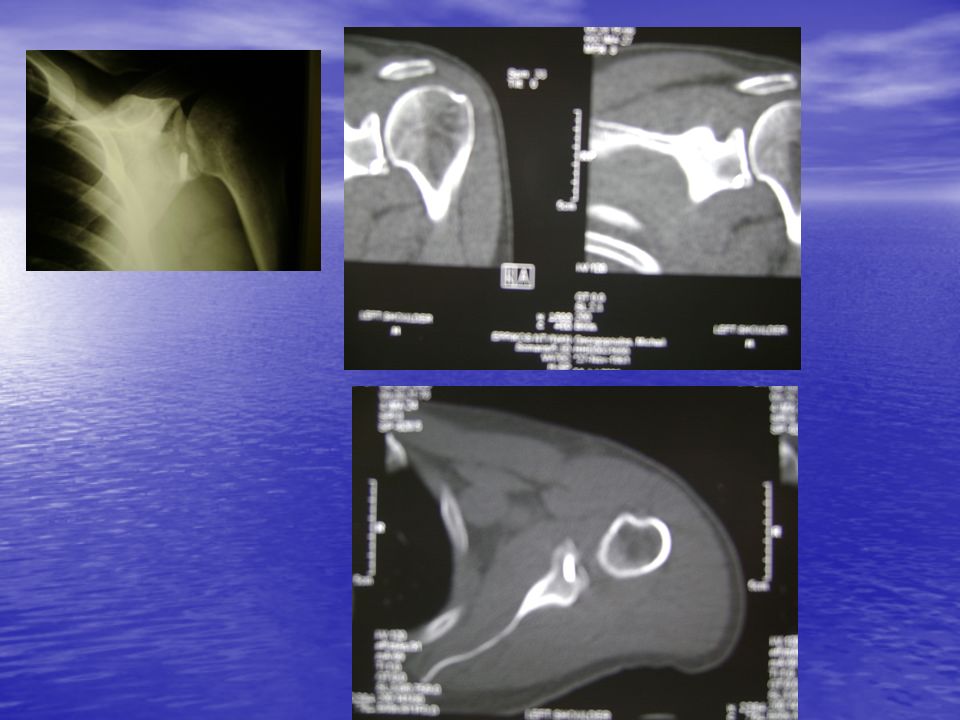
Male, 44 left side, nondom. Attempt to hold heavy item, ? dislocation Pain, movement restriction

57
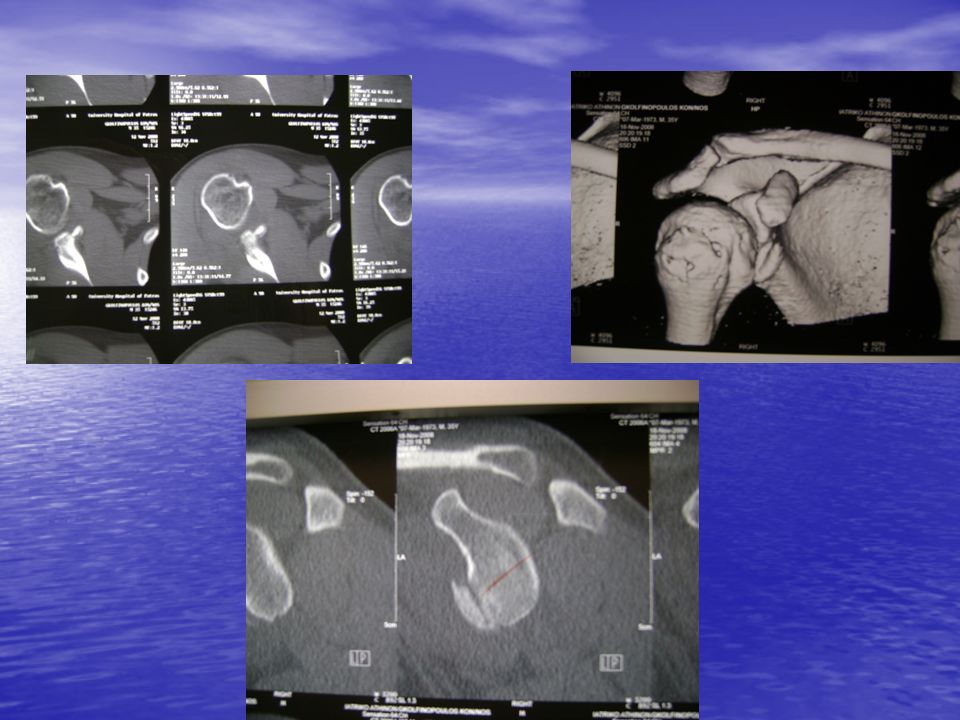
Male, 44, right side – dom. Dislocation. Closed reduction. Pain, restriction of movements. Male, 44, right side – dom. Dislocation. Closed reduction. Pain, restriction of movements.

59
14 ΤΕΛΙΚΟΣ ΕΛΕΓΧΟΣ

60
Type II Transverse or oblique # Transverse or oblique # Inf glenoid : free fragment Inf glenoid : free fragment Humeral head : sublux inferiorly Humeral head : sublux inferiorly ORIF ORIF

61
Type III Upper third of the glenoid and coracoid Upper third of the glenoid and coracoid Assoc. injuries : acromion #, clavicle #, acromioclavicular separation. Assoc. injuries : acromion #, clavicle #, acromioclavicular separation. ORIF : > 5 mm step- off, two incisions. ORIF : > 5 mm step- off, two incisions.

62
Type IV Horizontal # “ all the way “ to the vertebral border. Horizontal # “ all the way “ to the vertebral border. ORIF : separated or displaced # ORIF : separated or displaced #

63
Type V Combinaton of type II – IV Combinaton of type II – IV ORIF, more conservative if h.h. is well centered. ORIF, more conservative if h.h. is well centered.

Similar presentations















 Acromioclavicular (AC) Coracoclavicular (CC) Glenohumeral (GH) Scapulothoracic.>")






