Download presentation
Presentation is loading. Please wait.

1
Management of Locally Advanced NSCLC Shilpen Patel MD FACRO Department of Radiation Oncology, University of Washington, Seattle, WA

2
Roadmap Background Evolution of therapy Radiation alone Sequential chemotherapy and radiation Concurrent chemotherapy and radiation Trimodality versus bimodality Superior Sulcus Tumors Imaging

3
Survival Improvement in Stage III NSCLC since 1980’s9.8 13.8 17.7

4
Evolution: Radiation Alone In the 1970’s stage III NSCLC was an unresectable disease Standard of care was radiation alone

6
Evolution: Sequential chemotherapy and radiation

7
Dillman et al. Improved Survival in Stage III NSCLC: 7yr f/u of CALGB #8433. JNCI Vol 88, No 17: 1210-14, 1990 & 1996 165 Pts w/ stage III NSCLC randomized to: Cisplatin + vinorelbine Radiation-- 60Gy

8
Dillman et al. Improved Survival in Stage III NSCLC: 7yr f/u of CALGB #8433. JNCI Vol 88, No 17: 1210-14, 1990 & 1996 Median survival improved with chemotherapy –9.7 months with radiation alone –13.8 months with chemotherapy and radiation OS improved at 7 years: –6% with radiation alone –13% with chemotherapy and radiation

9
Evolution: Concurrent Chemoradiation

10
RTOG 94-10: Curran, et al, J Natl Cancer Inst. 2011 Oct 5;103(19):1452-60 RANDOMIZATIONRANDOMIZATION cDDP 100 mg/m 2 d1, 29 Vlb 5 mg/m 2 Q wk X 5 (d1, 8, 15, 22, 29) Standard fractionated RT (60 Gy) d 50 cDDP 100 mg/m 2 d1, 29 Vlb 5 mg/m 2 Q wk X 5 (d1, 8, 15, 22, 29) Standard fractionated RT(60 Gy) d1 cDDP 50 mg/m 2 d1, 8, 29, 36 VP-16 50 mg/m 2 d1-5, 8-12, 29-33, 36-40 Hyperfractionated RT (69.6 Gy) d1 CON- QD CON- BID SEQ
: RANDOMIZATIONRANDOMIZATION cDDP 100 mg/m 2 d1, 29 Vlb 5 mg/m 2 Q wk X 5 (d1, 8, 15, 22, 29) Standard fractionated RT (60 Gy) d 50 cDDP 100 mg/m 2 d1, 29 Vlb 5 mg/m 2 Q wk X 5 (d1, 8, 15, 22, 29) Standard fractionated RT(60 Gy) d1 cDDP 50 mg/m 2 d1, 8, 29, 36 VP mg/m 2 d1-5, 8-12, 29-33, Hyperfractionated RT (69.6 Gy) d1 CON- QD CON- BID SEQ.")
11
RTOG 94-10: Curran, et al, J Natl Cancer Inst. 2011 Oct 5;103(19):1452-60 Courtesy of Walter Curran, MD
: Courtesy of Walter Curran, MD.")
12
RTOG 94-10: Curran, et al, J Natl Cancer Inst. 2011 Oct 5;103(19):1452-60 Courtesy of Walter Curran, MD
: Courtesy of Walter Curran, MD.")
13
RTOG 94-10: Curran, et al, J Natl Cancer Inst. 2011 Oct 5;103(19):1452-60 In Field failure rates –Sequential:38% –Concurrent:33% –Hyperfractionated: 25%
: In Field failure rates –Sequential:38% –Concurrent:33% –Hyperfractionated: 25%.")
14
Local Control 65%

15
Evolution: Trimodality

16
Intergroup 0139- Albain, et al., 2009 Stage IIIA (T1-3, pN2, M0) NSCLC N = 429 (396 eligible) Considered Resectable RANDOMIZERANDOMIZE Cis/VP16 x 2 cycles w/concurrent XRT 45Gy Cis/VP16 x 2 cycles w/concurrent XRT 45Gy Surgery Cis/VP16 x 2 cycles Cis/VP16 x 2 cycles Re-evaluate 2 to 4 weeks post RT; if no PD Re-evaluate 7 days prior to RT completion; if no PD Continue RT to 61GY Median F/U 81 months
 NSCLC N = 429 (396 eligible) Considered Resectable RANDOMIZERANDOMIZE Cis/VP16 x 2 cycles w/concurrent XRT 45Gy Cis/VP16 x 2 cycles w/concurrent XRT 45Gy Surgery Cis/VP16 x 2 cycles Cis/VP16 x 2 cycles Re-evaluate 2 to 4 weeks post RT; if no PD Re-evaluate 7 days prior to RT completion; if no PD Continue RT to 61GY Median F/U 81 months")
17
Results: Intergroup 0139 Courtesy of Kathy Albain, MD

18
Intergroup 0139/RTOG 9309 Progression-Free Survival by Treatment Arms Percent Alive Months Trimodality ( n=201) Median 12.8 months 5-year 22.4% Chemoradiation (n=191) Median 10.5 months 5-year 11.1% 0 20 40 60 80 100 0612182430364248 / / / / / / / / // /// //// // / // / / // // / / / / / / / // / //////// // /// ///// /// Log rank p = 0.017
 Median 12.8 months 5-year 22.4% Chemoradiation (n=191) Median 10.5 months 5-year 11.1% / / / / / / / / // /// //// // / // / / // // / / / / / / / // / //////// // /// ///// /// Log rank p = 0.017")
19
Intergroup 0139/RTOG 9309 Lancet 8/1/09 Independent Favorable Survival Predictors Female No weight loss Trimodality Arm –pN0OS=41% –pN1-3OS=24% –No SurgeryOS=8%

20
Joshua Sonett, MD, et al Pulmonary Resection after curative intent radiotherapy (>59 Gy) and concurrent chemotherapy in NSCLC. Ann Thor Surg 2004;78(4) 40 consecutive patients who received high dose radiotherapy and concurrent platinum based chemotherapy between January 1994-May 2000 who then went on to undergo a lung resection. Patients –Stage IIB – 7 patients –Stage IIIA – 21 patients –Stage IIIB – 10 patients –Stage IV – 2 patients
 40 consecutive patients who received high dose radiotherapy and concurrent platinum based chemotherapy between January 1994-May 2000 who then went on to undergo a lung resection. Patients –Stage IIB – 7 patients –Stage IIIA – 21 patients –Stage IIIB – 10 patients –Stage IV – 2 patients.")
21
Surgery Median time to surgical resection 52.5 days (20-258 days) Surgeries –29 lobectomies –11 pneumonectomies No post-operative deaths Median ICU time = 2 days Overall length of stay = 6 days One patient developed post pneumonectomy pulmonary edema One patient developed a BP fistula
 Surgeries –29 lobectomies –11 pneumonectomies No post-operative deaths Median ICU time = 2 days Overall length of stay = 6 days One patient developed post pneumonectomy pulmonary edema One patient developed a BP fistula")
22
Results 34/40 patients (85%) were downstaged pathologically 33/40 patients (82.5%) had no residual lymphadenopathy 18/40 patients (45%) exhibited a complete pathologic response 22/26 patients (85%) with N2 disease exhibited pathologic confirmed sterilization of their mediastinal disease
 were downstaged pathologically 33/40 patients (82.5%) had no residual lymphadenopathy 18/40 patients (45%) exhibited a complete pathologic response 22/26 patients (85%) with N2 disease exhibited pathologic confirmed sterilization of their mediastinal disease")
23
Results Median follow-up was 2.8 years Overall survival at 1,2, and 5 years is 92%, 67%, 46% respectively. Median overall survival 53 months. Disease free survival at 1, 2, and 5 years is 73%, 67%, 56%. Median disease free survival not reached Failure Pattern –14% Local and distant –29% Brain only –29% Distant only –29% Local only

25
RTOG 0229, Suntharalingam IJROBP 2012 Stage III (pathologic ally proven N2 or N3) NSCLC N = 60 (57 eligible) CBDCA AUC =2.0, paclitaxel 50 mg/m 2 q week x 6, 50.4 Gy to the mediastinum and primary tumor and boost of 10.8 Gy to gross dz Surgery CBDCA AUC =6, paclitaxel 200 mg/m 2 q 21d x 2. Re-evaluate 2 to 4 weeks post RT; if no PD Median follow-up is 20 months.

26
RTOG 0229, Suntharalingam IJROBP 2012 Grade 3/4 toxicities: heme 35%, GI 14%, pulmonary 23%. 43 pts (75%) were evaluable for the primary endpoint; 36 pts underwent resection. 7 pts had residual mediastinal dz. 27/43 (63%) achieved mediastinal clearance. There was a 14% (5/37) incidence of grade 3 postoperative pulmonary complications. There was only one postop grade 5 toxicity (3%).
 were evaluable for the primary endpoint; 36 pts underwent resection. 7 pts had residual mediastinal dz. 27/43 (63%) achieved mediastinal clearance. There was a 14% (5/37) incidence of grade 3 postoperative pulmonary complications. There was only one postop grade 5 toxicity (3%)..")
27
RTOG 0229, Suntharalingam IJROBP 2012 With a median follow-up of 24 months for all patients, the 2-year overall survival rate was 54%, and the 2-year progression-free survival rate was 33%. The 2 year survival rate was 75% for those who achieved nodal clearance. Next steps? RTOG 0839

28
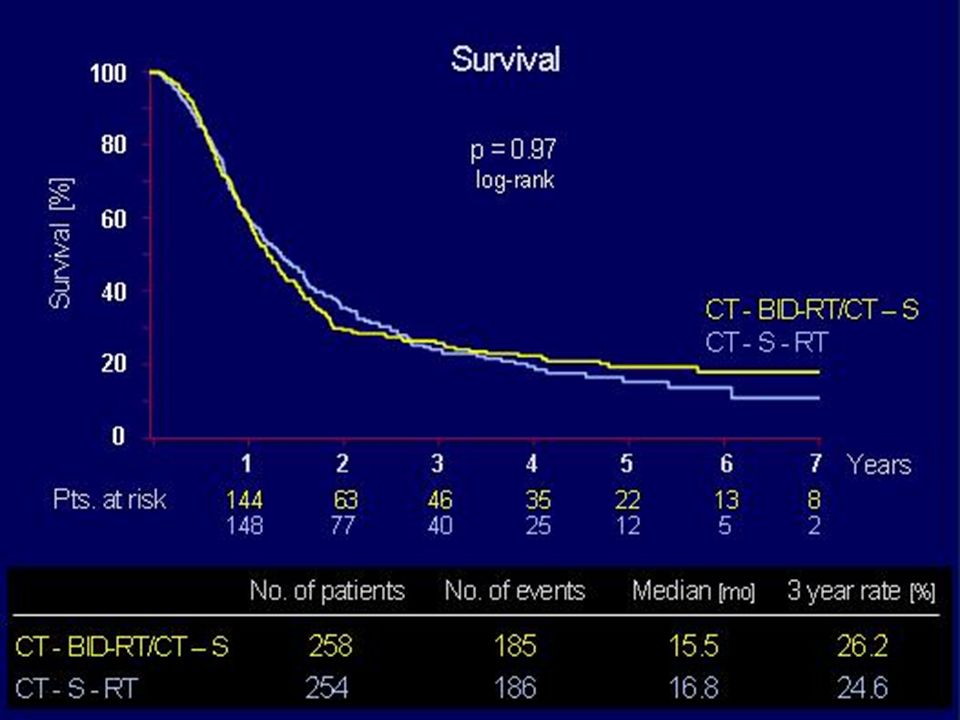
Thomas M, Macha HN, Ukena D, et al. Cisplatin/etoposide followed by twice daily chemoradiation versus cisplatin/etoposide alone before surgery in Stage III NSCLC: A randomized Phase III trial of the German Lung Cancer Cooperative Group. Lancet Oncology 2008

34
Thomas M, Macha Et al. Lancet Oncology 2008. Only 54-57% of Stage IIIA patients in either arm underwent a complete resection (R0) MST was not different between the arms (15.5 mo. in chemoradiotherapy and 16.8 mo. in chemotherapy only arm, p=0.97) Radiation was delivered in a non standard form (and we know from RTOG 9410 that BID is inferior!) Pneumonectomy contributed to mortality (14% versus 6%)
 MST was not different between the arms (15.5 mo. in chemoradiotherapy and 16.8 mo. in chemotherapy only arm, p=0.97) Radiation was delivered in a non standard form (and we know from RTOG 9410 that BID is inferior!) Pneumonectomy contributed to mortality (14% versus 6%).")
37
Van Meerbeeck et al JNCI 99(6) p 442-450 EORTC 08941 579 pts stage IIIA N2 NSCLC randomized: Platinum based chemo Radiation-- 60Gy Surgical Resection Radiation
 p EORTC pts stage IIIA N2 NSCLC randomized: Platinum based chemo Radiation-- 60Gy Surgical Resection Radiation")
38
Van Meerbeeck et al JNCI 99(6) p 442-450 EORTC 08941 In the XRT arm, g 3/4 acute and late esophageal and pulmonary toxicity was 4% and 7% Median and 5 y Overall survival (resection versus XRT) was 16.4 versus 17.5 mo and 15.7% versus 14%
 p EORTC In the XRT arm, g 3/4 acute and late esophageal and pulmonary toxicity was 4% and 7% Median and 5 y Overall survival (resection versus XRT) was 16.4 versus 17.5 mo and 15.7% versus 14%")
39
Is long term survival predicted by pathologic response?/Does mediastinal clearance matter? Rusch VW, Albain KS, Crowley JJ, et al Surgical Resection of Stage IIIA/IIIB NSCLC after induction chemoradiotherapy. J. Thorac Cardiovasc Surgery 1993;105:96-106 Sugarbaker DJ, Herdon J, Kohman LJ, Krasna MJ, Green MR, CALGB Thoracic Surgery Group. Results of CALGB 8935. A multiinstitutional phase II trimodality trial for Stage IIIA NSCLC. J Thorac Cardiovasc Surg 1995; 109; 473-83 Voltoni L, Luca L, Ghiribelli C, Paladini P, Di Bisceglie M, Gotti G. Results of induction chemotherapy followed by surgical resection in patients with stage IIIA NSCLC; the importance of nodal down staging after chemotherapy. Eur J Cardiothoracic Surg 2001;20:1106-12. Betticher DC, Schmitts S, Totsch M, et al Mediastinal lymph node clearance after docetaxol-cisplatin neoadjuvant chemotherapy is prognostic of survival in patients with stage IIIA pN2 NSCLC:a multicenter phase II trial JCO 21:1752-9.

40
What about superior sulcus tumors?

41
SWOG 9416 Pancoast tumors (n=83) Cis/Etoposide + XRT 45 Gy Surgery 2 cycles of chemo Re-evaluate 2 to 4 weeks post RT; if no PD
 Cis/Etoposide + XRT 45 Gy Surgery 2 cycles of chemo Re-evaluate 2 to 4 weeks post RT; if no PD")
44
Kwong KF, et al High-dose radiotherapy in trimodality treatment of Pancoast tumors results in high pathologic complete response rates and excellent long-term survival. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1250-7 36 patients with Pancoast tumor Stage IIB-IV R0 resection was achieved in 36 (97.3%) patients High-dose radiotherapy (mean 56.9Gy; range, 30- 70.2 Gy) was successfully tolerated in all but 1 patient Pathologic complete response was found in 40.5% (n = 15) of patients
: patients with Pancoast tumor Stage IIB-IV R0 resection was achieved in 36 (97.3%) patients High-dose radiotherapy (mean 56.9Gy; range, Gy) was successfully tolerated in all but 1 patient Pathologic complete response was found in 40.5% (n = 15) of patients.")
45
Kwong KF, et al. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1250-7 Operative mortality rate was 2.7% (n=1/37). Significant morbidities occurred in 10 patients (n=10/37, 27% patients) but were variable and without a dominant pattern
: Operative mortality rate was 2.7% (n=1/37). Significant morbidities occurred in 10 patients (n=10/37, 27% patients) but were variable and without a dominant pattern.")
46
Recurrences occurred in 50% of patients Distant recurrence accounted for the majority of recurrences (13 patients / 36.1%) Local recurrences in the lung-mediastinum occurred in 5 patients (13.8%) Kwong KF, et al. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1250-7
:")
48
New technology requires careful planning Treatment planning cannot make up for drawing the wrong volumes The most radioresistant tumor cell is the one that’s not in the field!

49
What about PET?

50
Assessing Gross Tumor Volume

51
Imaging in Lung Cancer Assessing Gross Tumor Volume

52
CT-then-PET Registration

53
PET-CT

54
Staging – PET/CT

55
What Respiratory 4D PET/CT Will Show … … 4D PET (tomorrow) 3D PET (today) }
 3D PET (today) }")
56
Imaging Questions

57
When is the tumor within my fields? –Tumor motion, mostly respiratory –4D CT –Does motion change during Rx? Infection Response to Rx How often should we re-measure motion? –Who would most benefit? How does the tumor change shape during Rx? –Second-to-second –Day-to-day

58
Benefits of Cone Beam CT

59
Imaging Questions for Radiation Oncology –Normal tissue function/risk? Interpatient differences –Radiosensitivity –Underlying disease –Pretreatment vs. post treatment imaging Can Dose/function histograms be developed?

60
Should we incorporate SPECT?

61
Voxel-by-voxel ventilation

62
Ventilation

64
Imaging Questions for Radiation Oncology –How do you account for these changes with IMRT or protons? –How do doses add together? –How do we image biology? Tumor? –SUV? –MR Spectroscopy? –Hypoxia, other markers?

65
Take Home Points Current standard of care for stage IIIA/IIIB NSCLC continues to be defined Trimodality is reasonable option on study and/or with well informed patients –Role of surgery should be based Nodal Status Performance Status Surgeon experience

66
Take Home Points Success of trimodality depends on: –Good radiotherapy techniques –Good surgical techniques Higher doses of radiation pre- operatively may improve outcomes Imaging will grow in importance in oncology

Similar presentations



















 CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 E V A L U A.>")











