Download presentation
Presentation is loading. Please wait.

1
What is it? Why do we need it POC?
Coagulation Testing What is it? Why do we need it POC? Marcia L. Zucker, Ph.D. Director of Clinical Research ITC Educational Services, Edison, NJ

2
Coagulation Testing Monitoring hemostasis Bleeding Clotting

3
Maintaining Hemostasis
Counterbalance thrombosis with anticoagulant therapy Thrombosis

4
Maintaining Hemostasis
Counterbalance bleeding by correcting defect (i.e., neutralize heparin, transfuse blood product) Bleeding
 Bleeding.")
5
Components of Hemostasis
Vessels Coagulation Proteins Platelets Fibrinolysis / Inhibitors

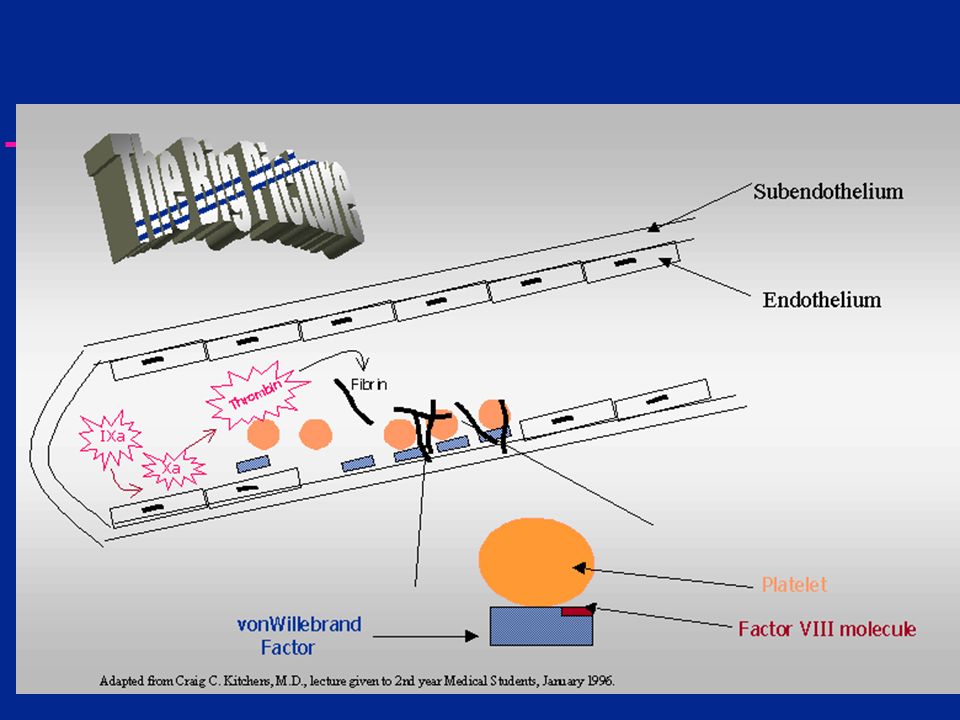
6
Vascular System Basement membrane Endothelial cells
Red blood cells Platelets White blood cells

7
Components of Hemostasis
Vessels Coagulation Proteins Platelets Fibrinolysis / Inhibitors

8
Anatomy of a Platelet

9
Resting Platelets

10
Platelet Aggregate

11
Hemostasis Primary hemostasis Secondary hemostasis Platelet Adhesion
Coagulation Fibrin clot formation

13
Platelet Function Platelet Adhesion shape change release 3 sec 10 sec
5 min ADP release Platelet Aggregation Coagulation Fibrin formation

14
Platelet Testing Peripheral smear Platelet count Platelet aggregation
Bleeding time

15
Peripheral Blood Smear

16
+ Platelet Aggregation Aggregate Clumping Platelet Rich Plasma (PRP)
Aggregating Agent Baseline Light Transmission Increased Light Transmission

17
Bleeding Time Cut 1 mm deep, 5 mm long Constant pressure
Expected Range : minutes

18
Components of Hemostasis
Vessels Coagulation Proteins Platelets Fibrinolysis / Inhibitors

19
Coagulation Inactive enzyme Active enzyme Inactive enzyme

20
Coagulation is Complex

21
Coagulation Testing Heparin Coumadin Thrombolytics Monitor with
Intrinsic Pathway Extrinsic Pathway Common Pathway CLOT Heparin Coumadin Monitor with ACT / aPTT Monitor with PT Thrombolytics TT / Fibrinogen

22
Common(?) Coagulation Tests
Laboratory PT.. aPTT TT.. Fib. Anti Xa Anti IIa Factor Assays Point of Care ACT Celite® Kaolin Glass beads Silica thromboplastin

23
Differences in test methods
Standard Laboratory Platelet Poor Plasma Sodium Citrate Anticoagulant 1:9 Dilution Variable Preanalytical Delay Point of Care Whole Blood Usually No Added Anticoagulant No Dilution No Preanalytical Delay

24
POC Coagulation Analyzers
HEMOCHRON 401 / 801 / Response HEMOCHRON Jr. Signature/ Signature+ ProTime Medtronic HMS/ HMS+ / HemoTec ACT II CoaguChek/ S / CoaguChek Pro/ Pro DM Bayer RapidPoint i-STAT Helena Actalyke Others

25
POC Coag Analyzers Differ
Test methodology Sample size and application Sample measurement Clot detection method Enzyme detection method Reagent composition Results

26
Semi - Automation - 1969 HEMOCHRONOMETER (HEMOCHRON)
Magnet in tube, detector in instrument Upon clot formation, magnet is deflected Clotting time displayed

27
HEMOCHRON Test Menu ACT aPTT and PT Thrombin time based assays
FTCA510, FTKACT, P214 aPTT and PT Fresh or citrated whole blood Thrombin time based assays TT, HNTT, HiTT Fibrinogen Dosing Assays HRT, PRT, PDAO Celite and kaolin

28
1980’s HemoTec (later ACTII) Medtronics HMS uses same technology
Smaller sample volume Mechanical detection Flag moves up and down As clot forms, motion slows Instrument displays clotting time Medtronics HMS uses same technology

29
Medtronics test menu ACT (kaolin) Empty cartridge for aPTT
PT (look up conversion) Heparinase ACT HMS Dosing Assays HDR, HPT
 Heparinase ACT. HMS Dosing Assays. HDR, HPT.")
30
Newer technologies Sample introduction by capillary action
CoaguChek Pro/ DM Time to when capillary flow stops determines endpoint Bayer RapidPoint Sample mixes with magnetic particles Pulsating magnetic field Motion detected optically

31
Test Menu CoaguChek ProDM CoaguChek / S Bayer RapidPoint ACT PT (FWB)
Tissue factor activated PT (FWB) aPTT (FWB) CoaguChek / S Detection as per RapidPoint PT only CLIA waived Bayer RapidPoint HMT aPTT F & C WB and plasma PT ECT (ecarin time) Compassionate use only ENOX Accent Dosing HTT, PRT
 aPTT (FWB) CoaguChek / S. Detection as per RapidPoint. PT only. CLIA waived. Bayer RapidPoint. HMT. aPTT. F & C WB and plasma. PT. ECT (ecarin time) Compassionate use only. ENOX. Accent Dosing. HTT, PRT.")
32
Newer Technologies Chemical endpoint detection i-STAT – Abbott
Synthetic thrombin substrate Electro-active compound formed and detected amperometrically Coagulation Test Menu ACT (Celite®) PT (cleared but not yet introduced)
 PT (cleared but not yet introduced)")
33
Newer Technologies Active pumping system Hemochron Jr Signature
ProTime microcoagulation system

34
Test Menu ProTime HEMOCHRON Jr Signature PT only CLIA waived ACT
Home use approved Integral Controls Meet CLIA and CAP requirement for daily QC testing HEMOCHRON Jr Signature ACT ACT+, ACT-LR PT Fresh or citrated WB aPTT

35
Activated Clotting Time
Extrinsic Pathway Intrinsic Pathway ACT Common Pathway CLOT

36
What do we use an ACT for? Maintain Balance Heparin
Bleeding Thrombosis Heparin Rapid Anticoagulant Effect Individual sensitivities vary significantly Potency differences Source: Bovine or Porcine Lot to Lot variability Rapidly Reversible with Protamine

37
Why are there so many different ACTs?

38
Monitoring - ACT Benefits Industry Standard Since 1970s
Recommended as primary method in AmSECT guidelines (perfusion) Easy to run
 Easy to run.")
39
Monitoring - ACT Disadvantages Each system yields different numbers
High sensitivity to hypothermia and hemodilution (with exceptions) Little or no correlation to heparin level especially true for pediatric patients
 Little or no correlation to heparin level. especially true for pediatric patients.")
40
Clinical Applications
Operating Room Cardiac Surgery Interventional Cardiology and Radiology Critical Care Satellite Sites Dialysis ECMO Emergency Room

41
Heparinized ACT - CPB Data from Huffman, et.al AmSECT meeting 17

42
Monitoring in CPB - ACT Data from clinical evaluation, on file, ITC

43
Pharmaceutical Intervention
Amicar or Tranexamic Acid No effect on standard celite ACT Continued debate on efficacy Multiple reports Reduction in post-operative blood loss Reduced transfusion requirements

44
Pharmaceutical Intervention
Aprotinin Significant elevation of celite ACT Two dosing regimens Full Hammersmith 2 x 106 KIU loading dose; 2 x 106 KIU pump prime; x 106 KIU/hr infusion Half Hammersmith 1 x 106 KIU loading dose; 1 x 106 KIU pump prime; x 106 KIU/hr infusion

45
ACT Monitoring-Aprotinin Treatment
Celite ACT Not recommended Still used with target times of >750 seconds Kaolin ACT Unaffected by moderate doses of aprotinin Used with target times of > 480 seconds ACT+ Unaffected by ALL doses of aprotinin Used with target times of > 400 seconds

46
ACT Monitoring -Aprotinin Treatment
Data from clinical evaluation, on file, ITC

47
Non-ACT Monitoring - Aprotinin
HiTT - High Dose Thrombin Time Adapted from Huyzen, et. al. J.CardioThorac. Vasc. Anesth. 8:153, 1994

48
Alternative Monitoring - Aprotinin
Adapted from Huyzen, et. al. J.CardioThorac.Vasc.Anesth. 8:153, 1994

49
Thrombin Time TT Intrinsic Pathway Extrinsic Pathway Common Pathway
CLOT

50
Other POC in the OR Heparin Level Xa Activity Medtronic Hepcon HMS
laboratory only, impractical Medtronic Hepcon HMS indirect measure of protamine reversible heparin activity in whole blood correlates with Xa and IIa activity HEMOCHRON PRT ACT based protamine titration HEMOCHRON HiTT unaffected by hemodilution, hypothermia insensitive to aprotinin

51
Monitoring - Heparin Level
Benefits Measures concentration, not activity Correlates with laboratory standards Disadvantages Each system yields different numbers apples and oranges do not compare Correlation to anticoagulation status is still disputed Target for neonate, pediatric and adult patients may differ

52
Monitoring - Heparin Level
Young: <4.5 years Shayevitz, JR and O’Kelly, SW Progress in Anesthesiology, vol. IX, chapter

53
Other POC Coag in the OR aPTT / PT Fibrinogen Dosing Assays
Pre- and post-procedural screening Fibrinogen Dosing Assays Customize heparin and protamine for each patient HEMOCHRON HRT / PRT Hepcon HMS

54
Other POC Coag in the OR Heparin neutralization verification
Ensure complete removal of circulating heparin aPTT PDA-O - ACT based TT / HNTT - Thrombin Time based heparinase ACT

55
Outcome studies - POC in OR
Reduced Blood Loss/Transfusion Use of HRT and PRT (RxDx System) Jobes, D. et. al., J.Thorac.Cardiovasc.Surg. Reduced Cost Resulting from POC Assays RxDx combined with TT / HNTT Jobes, D. et. al., Am Soc Anesth Mtg.
 Jobes, D. et. al., J.Thorac.Cardiovasc.Surg. Reduced Cost. Resulting from POC Assays. RxDx combined with TT / HNTT. Jobes, D. et. al., Am Soc Anesth Mtg.")
56
Outcome studies - POC in OR
Reduced Complication Rates TT /HNTT Re-Exploration for Bleeding Reduced from 2.5% to 1.1% Re-Exploration for Coagulopathy Reduced from 1.0% to 0.0% Jobes, et.al. 1997, NACB Presentation, Phila.

57
Clinical Applications
Operating Room Cardiac Surgery Interventional Cardiology and Radiology

58
Procedures Diagnostic Interventional Catheterization Electrophysiology
locate and map vessel blockage(s) determine need for interventional procedures Electrophysiology Interventional Balloon angioplasty Atherectomy (roto-rooter)
 determine need for interventional procedures. Electrophysiology. Interventional. Balloon angioplasty. Atherectomy (roto-rooter)")
59
Diagnostic – Low dose heparin
Catheterization and Electrophysiology unit bolus dose frequently not monitored if monitored – ACT aPTT

60
Interventional – Moderate dose
Angioplasty and Atherectomy 10,000 unit bolus dose or mg/kg target ACT seconds unless platelet inhibitors used 200 – 300 in presence of ReoPro

61
Why use platelet inhibitors?

62
Angioplasty promotes aggregation

64
Platelet Inhibitors ReoPro Integrelin Aggrastat elevates ACTs
target time = 250 sec with ReoPro determined using FTCA510 tube Integrelin No clinically significant effects on ACT Slight decrease in ACT observed Aggrastat No reported effects on ACT

65
QUESTIONS?

66
What is it? Why do we need it POC?
Coagulation Testing What is it? Why do we need it POC? PART 2 ITC Educational Services, Edison, NJ

67
Why Bother with POC Coag?
Improved TAT - Turn Around Time Defined from the Clinician, not Lab view When is Turn Around Important Emergency Room ICU/CCU Dose Adjustments Operating Room / Cath Lab STAT Testing Turn Around

68
STAT Testing TAT Fitch, et.al, J. Clin Monit & Comput :

69
Clinical Applications
Operating Room Cardiac Surgery Interventional Cardiology and Radiology Critical Care Satellite Sites Dialysis ECMO Emergency Room Anticoagulation Clinic

70
ACT or aPTT Determine when to pull the femoral sheath
Premature sheath pull can lead to bleeding. Delayed removal can increase time in CCU. Target set at each site. ACT targets range from 150 – 220 seconds aPTT targets range from 40 – 70 seconds

71
ACT or aPTT Monitor heparin therapy
Target times determined by each facility APTT outcome study Reduce time to result (112 vs <5 minute) Reduce time to stabilization Reduce dose adjustments Reduce length of stay By using POC aPTT instead of lab Poster at AACC 2000 – Staikos, et.al.
 Reduce time to stabilization. Reduce dose adjustments. Reduce length of stay. By using POC aPTT instead of lab. Poster at AACC 2000 – Staikos, et.al.")
72
What did it say? Mean time to lab result = 112 min
Mean time to POC result <5 min Fewer dose adjustments needed in POC group to reach therapeutic level Shorter time required to reach therapeutic level in POC group Fewer dose changes in POC group

73
Activated Partial Thromboplastin Time
Extrinsic Pathway Intrinsic Pathway APTT Common Pathway CLOT

74
Activated Partial Thromboplastin Time
NOT a PTT PTT is the predecessor of the aPTT Not used anymore Laboratory or Point of Care High APTT values the presence of heparin underlying coagulopathy Monitor heparin / coumadin® cross-over

75
Heparin versus Warfarin

76
Prothrombin Time PT Intrinsic Pathway Extrinsic Pathway Common Pathway
CLOT

77
Prothrombin Time Monitor warfarin therapy
Monitor heparin/warfarin crossover Target times are set by International Normalized Ratio (INR) ISI = international Sensitivity Index INR target ranges are specified by patient populations prophylactic therapy for DVT: INR= artificial heart valve: INR=2.5 – 3.5
 ISI = international Sensitivity Index. INR target ranges are specified by patient populations. prophylactic therapy for DVT: INR= artificial heart valve: INR=2.5 – 3.5.")
78
Will POC Results Match the Lab?
NO! (Probably Not) but it WILL Correlate
 but it WILL Correlate.")
79
Correlate Does Not Mean Match

80
Coag is NOT Chemistry

81
Compare for your site. Same System / Multiple Sites

82
Are differences important?
Sometimes no - aPTT C

83
Sometimes VERY - aPTT SP

84
Lot to Lot Reproducibility

85
Clinical Applications
Operating Room Cardiac Surgery Interventional Cardiology and Radiology Critical Care Satellite Sites Dialysis ECMO Emergency Room Anticoagulation Clinic

86
Dialysis / ECMO ACT (or nothing in dialysis)
Majority use P214 glass activated ACT Some use ACT-LR; HemoTec Better Control of Anticoagulation Leads to Increased Dialyzer Reuse Potential for Long Term Cost Savings No Compromise in Dialysis Efficacy (Kt/V) Ouseph, R. et.al. Am J Kidney Dis 35:89-94; 2000
 Ouseph, R. et.al. Am J Kidney Dis 35:89-94;")
87
Emergency Room ACT; aPTT; PT; Fibrinogen
Immediate Identification of Coagulopathies Optimization of Critical Decision Pathways ACT Allows Early Detection of Traumatic Coagulopathy Allows Early Treatment Decisions Aids Damage Control Decisions Aucar, J. et.al SW Surgeons Congress Optimize Staffing During Off Hours

88
Anticoagulation Clinics
Results Available While Patient is Present Improved Anticoagulation Management Improved Standard of Care Staff Efficiency Immediate Retesting (if needed) Fingerstick Sampling Same System for Clinic and Home Bound Patients Standardized ISI / PT normal Test System Specific
 Fingerstick Sampling. Same System for Clinic and Home Bound Patients. Standardized ISI / PT normal. Test System Specific.")
89
Anticoagulation Clinics
Potential for Self-Testing High Risk Patients Patients Who Travel Frequently Home-Bound Patients in Rural Areas Far from Clinic Improved Outcomes Through More Frequent Testing

90
How to compare INR differences
Has the Hemostatic Balance been Upset? Is the Clinical Response Different?

91
Patient Management 6.0 5.0 4.0 3.0 2.0 1.0 Target INR 3.0
Must change dose Target INR 3.0 Range Call Clinic May change dose Patient Management

92
What’s the catch? Regulatory compliance Connectivity

93
Regulatory compliance
Who sets the rules? JCAHO Joint Commission on Accreditation of Health Care Organizations CAP College of American Pathologists FDA Food and Drug Administration CMS (formerly HCFA) Centers for Medicare & Medicaid Services CDC Centers for Disease Control
 Centers for Medicare & Medicaid Services. CDC. Centers for Disease Control.")
94
CLIAC CLIA Committee CLIA - Clinical Laboratory Improvement Act
Define and interpret CLIA regulations CLIA - Clinical Laboratory Improvement Act Designed to ensure accuracy of results from clinical laboratories Compliance required to pass JCAHO and / or CAP inspections CLIA defines regulations for each test CDC / FDA / CMS / CDC complexity categories

95
CLIA Applies to ALL Testing Areas
Central Laboratory Satellite Labs Critical Care Surgical Suite Clinics Bedside testing Doctor’s office Home Testing

96
CLIA Regulations for Coagulation
Central Laboratory can hold the CLIA license Satellites can have independent licensure Moderately Complex tests Except - ProTime and Coaguchek / S are waived Requires Certified Laboratory Director Record Keeping Training Quality Policy

97
Implementing POC coag requires:
RECORD KEEPING Method Validation - accuracy comparison to current standard Performance Range Assessment “Linearity” often used Calibration/ verification NOT required for coag Is assay performance appropriate to clinical needs? Does dose responsiveness span clinical range? Training competency evaluations at predetermined intervals

98
Routine Quality Control
Instrument Performance Verification Electronic Quality Control with Numeric Output In GA, make sure state approves specific EQC Two levels per 8 hour shift Assay Performance Verification Wet QC as per Manufacturer’s Recommendation Two levels for each box of reagent when opened

99
Connectivity Everyone wants it Multiple definitions
Almost no one is ready to implement Multiple definitions Download to computer To LIS or to HIS or to both or to data management software Real time or batch QC data, patient data, or both

100
Short term solutions Interim programs for configuration, data capture, QC compliance tracking transfer to file format easily adaptable Requires independent transfer protocol e.g., ITC Configuration Manager, ReportMaker, HRDM Dedicated interface specific to one manufacturer’s instrumentation e.g., Abbott; Lifescan Manufacturer ensures system compatibility
![]()
101
Instrument manufacturer neutral interface
RALS-plus Telcor Manufacturer works with interface supplier to ensure compatibility Interface supplier works with LIS / HIS supplier to ensure compatibility

102
Long term Solutions POC Connectivity Industry Consortium
Accepted as NCCLS document POCT1-A sections of the CIC specification approved by: IEEE HL7 Standardization of POC connectivity: Messages Protocols Technologies

103
Why Bother with POC Coag?
Improved TAT - Turn Around Time Standardized Clinical Interpretation Defined Assay Sensitivity Requires Lot to Lot Reproducibility Defined Reagent Variability Identical Instrumentation /Reagents at All Testing Sites Defined Critical Clinical Decision Points No Change of Normal Ranges or Target Times Between Lots of Test Reagents or Testing Locations

104
Why Bother with POC Coag?
Improved Clinical Outcome Reduced LOS – Length of Stay Improved, timely patient care

Similar presentations












 V, VIII, XIII, Fibrinogen Inactive Factor Xa Common Pathway Inactive.>")







