Download presentation
Presentation is loading. Please wait.

1
Outpatient Surgery Centers Draw Cases Away from Hospitals, Impact Resident Training Volume Kyle Dunning, MD* Eric Liedtke DO* Lori Toedter, PhD† Chand Rohatgi, MD FASC* *Department of Surgery, Easton Hospital, Easton, PA †Department of Psychology, Moravian College, Bethlehem, PA

2
Background The first independent Ambulatory Surgery Center (ASC) was established in Phoenix, Arizona in 1970. Today, over 4,000 ASCs span all fifty states and account for over six million procedures per year. Currently, over 50% of colonoscopy services in the United States are performed in ASC’s.

4
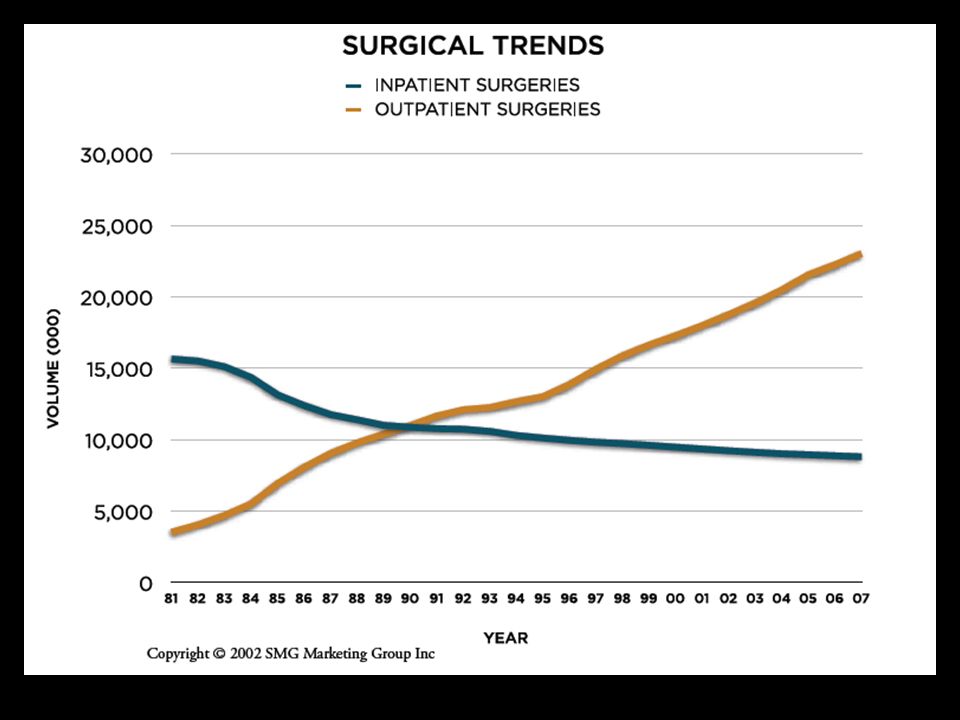
Purpose Ambulatory surgery centers (ASC’s) are increasing in both number and surgical volume Impact on reimbursement, patient safety, and surgical productivity and efficiency Shift toward outpatient surgery in non- hospital settings is concerning with respect to resident training
 are increasing in both number and surgical volume Impact on reimbursement, patient safety, and surgical productivity and efficiency Shift toward outpatient surgery in non- hospital settings is concerning with respect to resident training")
6
Hypothesis Due to the expansion of local surgery centers, hospital-based outpatient procedures would decline and, in turn, negatively affect case loads for our surgical residents.

8
Methods Performed a retrospective review Reviewed cases commonly performed in ASCs Reviewed cases commonly performed in ASCs Hernias, breast biopsies, endoscopies, etc. Double-armed evaluation Double-armed evaluation Analyzed data from two separate sources to perform independent evaluations 1. Reviewed resident reported data by year 2. Reviewed facility reported data per state reporting agency Resident reported data and hospital reported statistics are not directly comparable (reported by academic year and hospital data by calendar year)
.")
9
Study Design Resident reported data arm Reviewed case log data (July 2004–June 2007) Reviewed case log data (July 2004–June 2007) Tallied by academic year PGY1 – PGY3 resident data evaluated (n=30) ACGME electronic case log system Compared by procedure on yearly intervals Compared by procedure on yearly intervals Tabulated each procedure by number performed Evaluated for statistically significant increase or decrease
 Reviewed case log data (July 2004–June 2007) Tallied by academic year PGY1 – PGY3 resident data evaluated (n=30) ACGME electronic case log system Compared by procedure on yearly intervals Compared by procedure on yearly intervals Tabulated each procedure by number performed Evaluated for statistically significant increase or decrease")
10
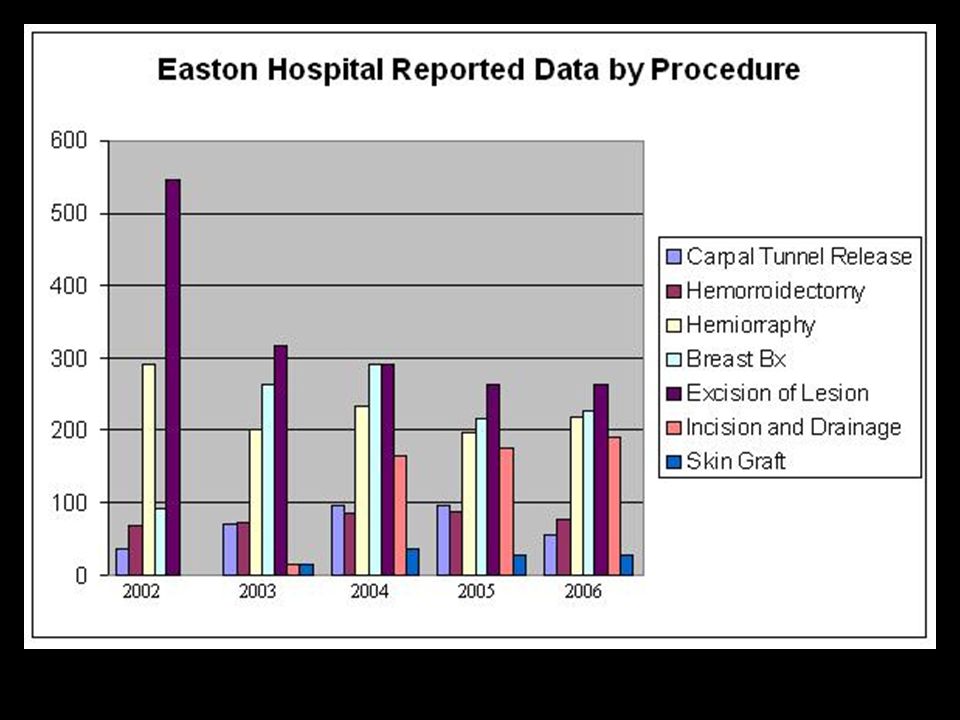
Results: Resident reported data Statistically significant decline in : Hemorrhoidectomies Hemorrhoidectomies carpal tunnel releases carpal tunnel releases excision of skin lesions excision of skin lesions breast biopsies breast biopsies skin grafts skin grafts

11
Study Design State reported data arm Outpatient Market Share State Data from the state of Pennsylvania Outpatient Market Share State Data from the state of Pennsylvania Data tallied by Pennsylvania Health Care Cost Containment Council (PHC4) Analyzed data between 2001-2006 by calendar year Included our institution and four local ASCs that participated in voluntary reporting Compared hospital outpatient procedures vs. the four ASCs individually and in total Calculated specified procedures as a percentage of total hospital volume to account for any errors from fluctuating volume

12
Results: State reported data 2003 vs. 2005 there was a significant decrease for some specific procedures: colonoscopy (p<.0001); colonoscopy (p<.0001); inguinal/femoral hernia (p=.04); inguinal/femoral hernia (p=.04); excision of skin lesion (p=.0022) excision of skin lesion (p=.0022) incision/drainage (p<.0001). incision/drainage (p<.0001). No significant differences were noted for carpal tunnel release, endoscopy, hemorrhoidectomy, lumpectomy or skin graft. No significant differences were noted for carpal tunnel release, endoscopy, hemorrhoidectomy, lumpectomy or skin graft. Trend toward significant decrease each year from 2001 to 2006, however could not complete calculations due to some missing intervals
; colonoscopy (p<.0001); inguinal/femoral hernia (p=.04); inguinal/femoral hernia (p=.04); excision of skin lesion (p=.0022) excision of skin lesion (p=.0022) incision/drainage (p<.0001). incision/drainage (p<.0001). No significant differences were noted for carpal tunnel release, endoscopy, hemorrhoidectomy, lumpectomy or skin graft. No significant differences were noted for carpal tunnel release, endoscopy, hemorrhoidectomy, lumpectomy or skin graft. Trend toward significant decrease each year from 2001 to 2006, however could not complete calculations due to some missing intervals.")
14
Results: State reported data The total number of cases for both inpatient and outpatient surgeries between 2003 and 2005 ASC’s reported a combined total of 9,089 cases in 2003 compared with 12,832 cases in 2005 for a 41.2% increase in volume ASC’s reported a combined total of 9,089 cases in 2003 compared with 12,832 cases in 2005 for a 41.2% increase in volume Our institution increased 6% (11,587 to 12,279) Our institution increased 6% (11,587 to 12,279) While the total volume increased by 6%, there was a 4% decrease in selected cases 1 performed between these two years. (p<.0001) 2. The selected cases represented 29.9% of all the hospital cases in 2003, compared to 28.5%, 27.2% and 27.5% in 2004 through 2006. 1 Pre-selected cases for this study 2 Chi-square Goodness-of-Fit test
 2. The selected cases represented 29.9% of all the hospital cases in 2003, compared to 28.5%, 27.2% and 27.5% in 2004 through Pre-selected cases for this study 2 Chi-square Goodness-of-Fit test.")
15
Pennsylvania Health Care Cost Containment Council (PHC4)
")
16
Discussion Operative case numbers as a measure of surgical training Is it an effective measurement? Is it an effective measurement? How many to be certified; competent; proficient? How many to be certified; competent; proficient? Today, outpatient procedures constitute the bulk of all surgeries Residents are losing exposure to more basic cases that serve as building block for surgical skills May be less prepared for more challenging procedures May be less prepared for more challenging procedures The “80-hour work week”

17
Confounding Variables Compliance and accuracy of resident reported data Varies among residents Varies among residents Only available for past 4 years Only available for past 4 years Voluntary reporting to State agency Some centers have gaps in certain years Some centers have gaps in certain years Not all centers reporting in area Not all centers reporting in area Academic vs. Calendar year data Allowed two separate analysis of same hypothesis Allowed two separate analysis of same hypothesis Study area is not isolated Patients may have gone to other hospitals Patients may have gone to other hospitals Also may have had procedure performed in non-reporting ASCs Also may have had procedure performed in non-reporting ASCs

18
Pennsylvania Health Care Cost Containment Council (PHC4)
")
19
Conclusions Based on our results, ASCs have significantly impacted certain cases available to our residents More data will be collected and prospectively followed in the years to come Surgical residency directors must look to include access to ASCs in the their residency programs to assure the highest quality training

20
References Ambulatory Surgery Center Association http://www.ascassociation.org/advocacy/AmbulatorySurgeryCentersPositiveTrend HealthCare.pdf Frakes JT. Ambulatory endoscopy centers: what the interviewing fellow needs to know. Gastrointest Endosc 2005; 62: 112-113. Ferguson CM, Kellogg KC, et al. Effect of Work-hour Reforms on Operative Case Volume of Surgical Residents. J Am Coll Surg 2005;62(5):535-538. Pennsylvania Health Care Cost Containment Council (PHC4) http://www.phc4.org/default.htm Carlin AM, Gasevic E, Shepard A. Effect of the 80-hour work week on resident operative experience in general surgery. Am J Surg 2007; 193:326-330. Smale BF, Reber HA, Terry BE, Silver D. The creation of a surgical endoscopy training program-Is there sufficient clinical material? Surg 1983; 94:180-185. Spencer AU, Teitelbaum DH. Impact of Work-Hour Restrictions on Residents’ Operative Volume on a Subspecialty Surgical Service. J Am Coll Surg 2005;200:670-676.
: Pennsylvania Health Care Cost Containment Council (PHC4) Carlin AM, Gasevic E, Shepard A. Effect of the 80-hour work week on resident operative experience in general surgery. Am J Surg 2007; 193: Smale BF, Reber HA, Terry BE, Silver D. The creation of a surgical endoscopy training program-Is there sufficient clinical material. Surg 1983; 94: Spencer AU, Teitelbaum DH. Impact of Work-Hour Restrictions on Residents’ Operative Volume on a Subspecialty Surgical Service. J Am Coll Surg 2005;200:")
Similar presentations