Download presentation
Presentation is loading. Please wait.

1
Clostridium difficile David B. Blossom, MD MS Division of Healthcare Quality Promotion Coordinating Center for Infectious Diseases Centers for Disease Control and Prevention

2
Objectives Review of Clostridium difficile Discuss the transmission and virulence of C. difficile Describe briefly the clinical manifestations, evaluation and treatment of C. difficile-associated disease (CDAD) Identify the changing epidemiology of CDAD Define surveillance strategies Clarify preventive measures
 Identify the changing epidemiology of CDAD Define surveillance strategies Clarify preventive measures.")
3
Clostridium difficile Anaerobic spore-forming bacillus Ubiquitous in nature –Prevalent in soil –Isolated also from river, lake, sea, and swimming pool water as well as from farm animals, dogs, and cats 1 1935 - First described by Hall and O'Toole 2 –Known colonizer of neonates (50% to 60%) 1978 - recognized as cause of antimicrobial- associated pseudomembranous colitis 3 Now regarded as most common cause of antimicrobial-associated diarrhea (20-30% of cases) 1. Brazier JS, al Saif. J Med Microbiol 1996; 45: 133-7 2. Hall I; O'Toole E. Am J Dis Child 1935; 49: 390 3. Larson HE et al. Lancet 1978; 8073: 1063–1066.

4
Clostridium difficile : Pathogenesis Fecal oral transmission Survive gastric acidity Small intestine – spores germinate into vegetative forms Large intestine – normal flora disrupted by antibiotics Diagram: Sunenshine et al Clev Clin J Med 2006 73(2) 187-197
")
5
C. difficile : Pathogenesis (cont) C. difficile can produce 3 toxins –Toxin A – enterotoxin –Toxin B – cytotoxin –(Binary toxin) Toxins cause the disease –Some strains only produce one toxin (A-, B+) 1% in a recent study from Chicago 1 Diagram: Sunenshine, et al. Clev Clin J Med 2006 73: 187-197 1.Geric B, et al. J Med Micro 2004;53:887-94
 Toxins cause the disease –Some strains only produce one toxin (A-, B+) 1% in a recent study from Chicago 1 Diagram: Sunenshine, et al. Clev Clin J Med : Geric B, et al. J Med Micro 2004;53:")
6
C. difficile-Associated Disease (CDAD) Incubation period – not known Diarrhea Pseudomembranous colitis - Has become the hallmark of CDAD 1 - Bloody diarrhea - Raised whitish-yellow plaques - Unexplained leukocytosis (>10,000/cubic mm ) Pseudo- membranous colitis Healthy colon 1. Bartlett JG, et al. Gastroenterology 1978; 75:778-82
 Incubation period – not known Diarrhea Pseudomembranous colitis - Has become the hallmark of CDAD 1 - Bloody diarrhea - Raised whitish-yellow plaques - Unexplained leukocytosis (>10,000/cubic mm ) Pseudo- membranous colitis Healthy colon 1. Bartlett JG, et al. Gastroenterology 1978; 75:")
7
Toxic megacolon Life-threatening acute dilation Characterized by - a dilated colon (megacolon) - Diameter : ≥ 5.5 cm - Fever, abdominal pain, abdominal distension - Radiograph: apparent edema of bowel wall Complications - Perforation of colon - Sepsis, Shock - Death Diagram: http://www.nlm.nih.gov/medlineplus/ency/imagepages/17189.htm
 - Diameter : ≥ 5.5 cm - Fever, abdominal pain, abdominal distension - Radiograph: apparent edema of bowel wall Complications - Perforation of colon - Sepsis, Shock - Death Diagram:")
8
Summary: Pathogenesis of C. difficile Exposed to C. difficile Antibiotic therapy Disturbed colonic microflora Toxin A & Toxin B Diarrhea & colitis

9
C. difficile : Risk Factors Increasing age 1 Exposure to antimicrobials Length of stay in hospital 2 Infected patients/CDAD pressure Immune response – IgG or local IgA against toxin A 3 Severe underlying gastrointestinal diseases –GI procedures or GI surgery PPI/H2 blockers? 1.Brown E et al. Infect Control Hosp Epi 1990;11: 283-90 2. Johnson S, et al Lancet 1990;336:97-100 3. M. Delmee Clin Microbiol Infect 2001; 7: 411-416 Biggest Risks

10
Increasing Age Population based study in Sweden –Rate in those over 65 y.o = 20 times higher than those under 20 y.o Quebec 2002 to 2003 –Rates in >65 y.o increased from 120 to 800 per 100,000 –Rates in under 65 y.o stayed stable (<100 per 100,000 1.Karlstrom et al. Clin Infect Dis 1998;26:141-5 2.Pepin et al. CMAJ 2004;171:466-72

11
Antimicrobial Exposure Major risk factor for disease -Acquisition and growth of C. difficile -Suppression of normal flora of the colon -The risk doubles with longer than three days of antibiotic therapy (risk ratio: 2.28) 1 Clindamycin, penicillins, cephalosporins Fluroquinolones 2 1.Wistrom J et al. J Antimicrob Chemother 2001;47:43-50 2. Pepin J. Clin Infect Dis. 2005 Nov 1;41(9):1254-60
 1 Clindamycin, penicillins, cephalosporins Fluroquinolones 2 1.Wistrom J et al. J Antimicrob Chemother 2001;47: Pepin J. Clin Infect Dis Nov 1;41(9):")
12
Flouroquinolones Quebec 1 –12 hospitals in 2004, OR for quinolones was 3.9 (95%CI 2.3-6.6) –Ciprofloxacin, gatifloxacin and moxifloxacin associated, levofloxacin was not Pittsburgh 2 –Formulary change: ciprofloxacin to levofloxacin –C. diff rate = 2.7/1000 d/c increased to 6.8/1000 d/c OR 2.0 (95% CI 1.2-3.3) 1 Loo VG, et al. NEJM 2005; 353:2442-9 2 Muto CA et al. Infect Control Hosp Epidemiol 1005; 26:273-80
 1 Loo VG, et al. NEJM 2005; 353: Muto CA et al. Infect Control Hosp Epidemiol 1005; 26:")
13
Length of Hospitalization Related to rates of colonization 1,2 Rates increase from <5% at admission to 26% after hospitalization 1.McFarland et al. N Engl J Med 1989;320:204-10 2. Clabots et al. JID 1992;166:561-67

14
Other Risk Factors: CDAD Pressure Number of concurrent inpatients with CDAD on the same ward increases a patient’s risk of developing CDAD = daily exposure to CDAD patients Length of stay at risk

15
CDAD Pressure Dubberke et al. Arch Int Med 2007; 167: 1092-7 VariableRel. Risk95% CI Sum CDAD pressure 1 or lessRef. 2-83.92.8-5.5 More than 89.77.1-13.1 Mean CDAD pressure Less than 0.3Ref. 0.3-1.46.44.6-8.9 More than 1.48.76.3-12.0

16
C. difficile : Laboratory Tests Stool culture: Most sensitive - Requiring 2-3 days for growth - Unable to distinguish between the presence of toxin positive strains or toxin negative strains Cell cytotoxin test – most specific - Cytotoxin B Direct Enzyme immunoassay (EIA) – most common - May detect Toxin A only or Toxin A and B C difficile colonies on agar plate: http://en.wikipedia.org/wiki/Clostridium_difficile
 – most common - May detect Toxin A only or Toxin A and B C difficile colonies on agar plate:")
17
C. difficile: Resolution and Recurrence Resolution: 15 to 23% of patients - Within 2 to 3 days after discontinuation - But most patients require specific treatment C. difficile diarrhea recurs after treatment in ~20% of cases Historically mortality rate was 1 to 2.5 percent

18
Treatment Initial Course of Antibiotics –At least 10 days –Metronidazole (mild/moderate disease) –Oral vancomycin (severe disease) 1 Treatment of Recurrence –Longer course of metronidazole –Vancomycin with a taper –Rifaximin –Nitazoxanide –Vancomycin and rifaximin 2 1. Zar FA, et al. CID 2007; 45: 302-7 2. Johnson S, et al. CID 2007; 44: 846-8

19
Costs Responsible for more than $1 billion annually in excess healthcare costs* - Average of $3,600 excess costs per case - Average of 3.6 extra hospital days * Kyne L, et al. Clin Infect Dis. 2002;34:346-353

20
Increasing Rates of C. difficile-associated Disease (CDAD) in US Hospitals McDonald et al. 14th Annual Scientific Meeting of the Society for Healthcare Epidemiology of America, Philadelphia, PA. 2004

21
McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15 National Estimates of US Short-Stay Hospital Discharges with C. difficile as First-Listed or Any Diagnosis
: National Estimates of US Short-Stay Hospital Discharges with C. difficile as First-Listed or Any Diagnosis.")
22
McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15 Rates of US Short-Stay Hospital Discharges with C. difficile Listed as Any Diagnosis by Age
: Rates of US Short-Stay Hospital Discharges with C. difficile Listed as Any Diagnosis by Age.")
23
United Kingdom, 1994-5 1 -Comparing well-matched C difficile patients and controls – no difference in mortality at d/c, 3 mos. and 6 mos. Pittsburgh, 2000 2 –“Life-threatening disease” from 1.6% to 3.2% from 1989 to 2000 –Colectomies increased from 0.48% to 2.6% –In hospital deaths (attr. to C. difficile) increased from 0.21-1.4% Quebec, Canada, 2004 3 –Attributable mortality of 16.7% in 2005 epidemic in Quebec (in one hospital) –Attributable 30 day mortality 6.9% in 12 Quebec hospital prospective study Increasing Severity of CDAD 1. MacGowan AP, et al. J Antimicrob Chemother 1997;39:537-41 2. Dallal RM, et al. Ann Surg. 2002;235:363-372. Loo VG, et al. NEJM 2005;353:2442-2449 3. Pepin J et al. CMAJ. 2005;173(23):1037-42.
 increased from % Quebec, Canada, –Attributable mortality of 16.7% in 2005 epidemic in Quebec (in one hospital) –Attributable 30 day mortality 6.9% in 12 Quebec hospital prospective study Increasing Severity of CDAD 1. MacGowan AP, et al. J Antimicrob Chemother 1997;39: Dallal RM, et al. Ann Surg. 2002;235: Loo VG, et al. NEJM 2005;353: Pepin J et al. CMAJ. 2005;173(23):")
24
Potential reasons for increased CDAD incidence and severity Changes in underlying host susceptibility Changes in antimicrobial prescribing Changes in infection control practice New strain with increased virulence

25
Hypothesis: C hange in underlying host susceptibility Increase in the average age of the population - Increase in exposure to healthcare facilities - Increase exposure to antimicrobials Possible, but probably not the whole story

26
Hypothesis: Use of alcohol-based hand rubs Hand hygiene - Important prevention strategy - HCWs can transmit C. difficile Traditional: Soap and water hand washing Increased use of alcohol-based hand rub over the last several years

27
Boyce et al. Infect Control Hosp Epidemiol 2006; 27:479-483 No relationship between alcohol-based hand rubs and increasing rates of CDAD

28
Hypothesis: Change in antimicrobial prescribing Quinolones –Popular for the management of CAP 1 –Most common treatment for uncomplicated UTI in women 4 –Increased use by >50% from 2000– 2002 (p<0.001) 2 Multiple antimicrobials and longer course of therapy - Increases risk for C. difficile 3 1. Jones RN, Mandell LA. Diagn Microbiol Infect Dis. 2002;44:69–76 2. MacDougall C et al Emerg Infect Dis. 2005 ; 11(3):380-4 3. Bignardi GE. J Hosp Infect 1998; 40:1–15. 4. Kallen et al. Arch Int Med. 2005
: Bignardi GE. J Hosp Infect 1998; 40:1– Kallen et al. Arch Int Med")
29
Fact: Epidemic C. difficile Strain Characteristics –North American Pulsed Field Type 1 (NAP1) by PFGE –PCR ribotype 027 –Toxinotype III or “BI” by REA Distinct from “J” strain of 1989-1992 1 –Binary toxin as a possible virulence factor In addition to Toxin A&B containing –18 bp deletion in tcdC gene May allow increased toxin production 2 –Increased resistance to fluoroquinolones –No resistance to metronidazole 1 Johnson S, et al. N Engl J Med 1999;341:1645-51 2 Warny M, et al. Lancet 2005; 366: 1079-84
 by PFGE –PCR ribotype 027 –Toxinotype III or BI by REA Distinct from J strain of –Binary toxin as a possible virulence factor In addition to Toxin A&B containing –18 bp deletion in tcdC gene May allow increased toxin production 2 –Increased resistance to fluoroquinolones –No resistance to metronidazole 1 Johnson S, et al. N Engl J Med 1999;341: Warny M, et al. Lancet 2005; 366:")
30
Acute Care Hospitals with CDAD Outbreaks* Between 2001-2004 *Detected by increases in the number of positive routine clinical laboratory tests for C. difficile. McDonald LC, et al. N Engl J Med. 2005;353:2433-2441. 2 1 2 1 1 1

31
Common (Epidemic) Strain by PFGE Maine, Hospital A Pennsylvania Maine, Hospital B Illinois Georgia Maine, Hospital A New Jersey Oregon Historic, 1988-1991 Historic, 1993 Historic, 1990-1991 Historic, 1984-1991 Historic, 1993-2000 Oregon
 Strain by PFGE Maine, Hospital A Pennsylvania Maine, Hospital B Illinois Georgia Maine, Hospital A New Jersey Oregon Historic, Historic, 1993 Historic, Historic, Historic, Oregon")
32
Toxinotype and Potential Virulence Factors of Isolates Characteristic: 1 Epidemic strain n=62 (%) Non-epidemic strain n=36 (%) Toxinotype III62 (100)0202 Binary toxin positive62 (100)2 (6) 18 bp tcdC deletion62 (100)1 (3) 1 Includes 5 historic “BI” isolates 2 32 (89%) were toxinotype 0 or wild type
 Non-epidemic strain n=36 (%) Toxinotype III62 (100)0202 Binary toxin positive62 (100)2 (6) 18 bp tcdC deletion62 (100)1 (3) 1 Includes 5 historic BI isolates 2 32 (89%) were toxinotype 0 or wild type")
33
Increased Toxin A Production in vitro Warny M, et al. Lancet. 2005;366:1079-1084. In vitro production of toxins A and B by C. difficile isolates. Median concentration and IQRs are shown. C. difficile strains included 25 toxinotype 0 and 15 NAP1/027 strains (toxinotype III) from various locations.
 from various locations..")
34
Increased Toxin B Production in vitro Warny M, et al. Lancet. 2005;366:1079-1084. In vitro production of toxins A and B by C. difficile isolates. Median concentration and IQRs are shown. C. difficile strains included 25 toxinotype 0 and 15 NAP1/027 strains (toxinotype III) from various locations.
 from various locations..")
35
Increased Resistance in Epidemic Strain Isolates (After 2000) No. (%) Intermediate or Resistant: Epidemic strain (n=18) Non-epidemic strains (n=18) P Clindamycin16 (89)10 (56)0.06 Fluoroquinolones18 (100)8 (44)<0.001
 Intermediate or Resistant: Epidemic strain (n=18) Non-epidemic strains (n=18) P Clindamycin16 (89)10 (56)0.06 Fluoroquinolones18 (100)8 (44)<")
36
States with the Epidemic Strain of C. difficile Confirmed by CDC and Hines VA labs (N=27), Updated 4/3/2007 DC PR AK HI
, Updated 4/3/2007 DC PR AK HI.")
37
Lethal hospital bug cases rocket, United Kingdom Potentially lethal cases of C. difficile “rocketed” from 1990s to 2004 Cases had increased from 1,000 in 1990 to over 35,000 in 2003 44,488 cases of C. difficile in > 65 year olds in 2004. BBC News. http://news.bbc.co.uk/2/hi/health/4186834.stm

38
NAP1/BI/027 in the Netherlands, 2006 1.Kuiper EJ et al. Emerg Infect Dis 2006;12(5):827-830. 2. Goorhuis A et al. CID 2007; 45: 695-703
: Goorhuis A et al. CID 2007; 45:")
39
Other Places… Canada France Poland Austria Japan Eurosurveillance Weekly Release. http://www.eurosurveillance.org/index.asp

40
Community-associated CDAD: Sentinel Cases of Severe Disease 23 cases of severe community-associated CDAD (CA-CDAD) Generally young and healthy Approximately 1/3 without precedent antimicrobial use
 Generally young and healthy Approximately 1/3 without precedent antimicrobial use")
41
Severe CDAD in Populations Previously at Low Risk—Four States, 2005 (1) Recent reports to the Pennsylvania Department of Health and CDC –Young patients without serious underlying disease –C. difficile toxin-positive by routine diagnostic testing –Responded to CDAD-specific therapy Peripartum –Within 4 weeks of delivery –Reports from PA, NJ, OH, and NH Community-associated –No hospital exposure in prior 3 months –Reports from Philadelphia and 4 surrounding counties CDC. MMWR. 2005;54:1201-1205.

42
Severe CDAD in Populations Previously at Low Risk—Four States, 2005 (2) CDC. MMWR. 2005;54:1201-1205. Characteristic, No. (%) Community (N=23) Peripartum (N=10) Total (N=33) Aged < 18 years11 (48)0 (0)11 (33) Female15 (65)10 (100)25 (76) Antimicrobial exposure15 (65)9 (90)24 (73) Bloody diarrhea6 (26)2 (20)8 (24) Hospitalization necessary 6 (26)4 (40)10 (24) ER visit necessary3 (13)2 (20)5 (15) Relapse8 (35)5 (50)13 (39)
 Community (N=23) Peripartum (N=10) Total (N=33) Aged < 18 years11 (48)0 (0)11 (33) Female15 (65)10 (100)25 (76) Antimicrobial exposure15 (65)9 (90)24 (73) Bloody diarrhea6 (26)2 (20)8 (24) Hospitalization necessary 6 (26)4 (40)10 (24) ER visit necessary3 (13)2 (20)5 (15) Relapse8 (35)5 (50)13 (39).")
43
Recent onset dates –February 26, 2003 – June 28, 2005 –Only 1 case in 2003 Transmission to close contacts in 4 cases 8 cases without antimicrobial exposure –5 children; 3 required hospitalization –3 had close contact with diarrheal illness Another 3 cases with < 3 doses of antimicrobials Clindamycin most common exposure (10 cases) Severe CDAD in Populations Previously at Low Risk—Four States, 2005 (3) CDC. MMWR. 2005;54:1201-1205.

44
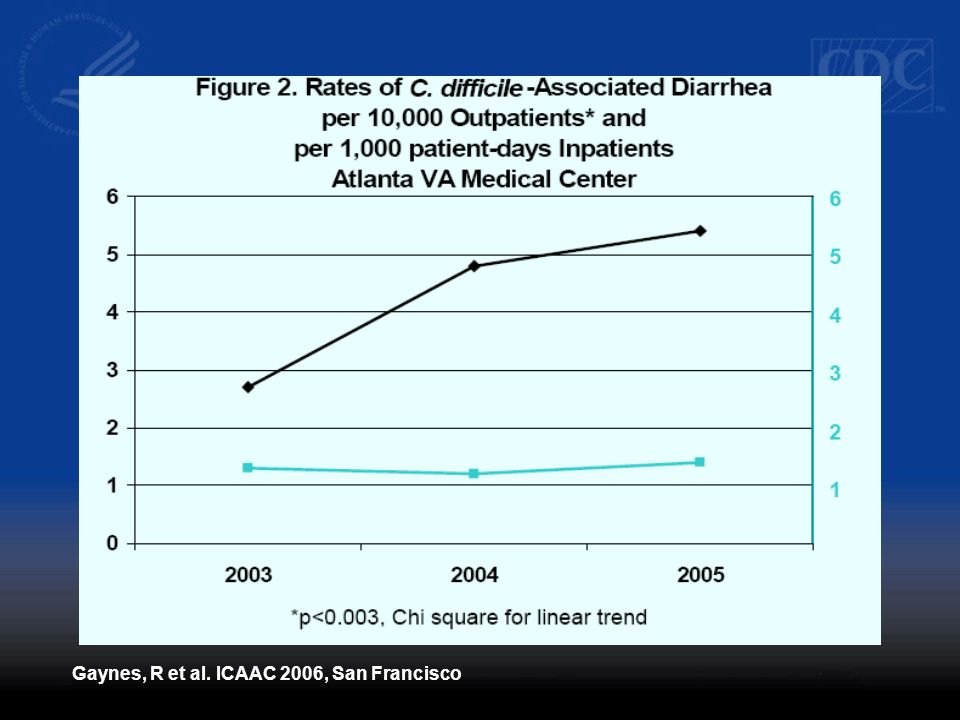
Community-associated CDAD may be Increasing, Atlanta VA Hospital 73 total cases 93 total cases 99 total cases 67 total cases* Through July 31, 2006 Chi-square for trend: P<0.05 Gaynes, R et al. ICAAC 2006, San Francisco

46
Many Patients Develop CDAD without Recent Hospital or Antimicrobial Exposure, Atlanta VA Hospital, 2003-2006 Gaynes, R et al. ICAAC 2006, San Francisco

47
What is the Source? Is it in the food supply? –Pathogen of food animals 1 –C. difficile has been found in retail meat (beef and veal) 2 20% of Canadian convenience sample Only 3 of the 12 isolates found had corresponding isolated that had caused disease in humans C difficile reported to live after being exposed to 71 degrees Celsius for 120 min. –Potential for interspecies transmission 3 Turkey fed to dogs 1 Songer JG, et al. Anaerobe 2006; 12: 1-4 2 Rodriguez-Palacios A, et al. EID 2007; 13: 485-7 3 Arroyo LG, et al. J Med Microbiol 2005; 54: 163-6
 2 20% of Canadian convenience sample Only 3 of the 12 isolates found had corresponding isolated that had caused disease in humans C difficile reported to live after being exposed to 71 degrees Celsius for 120 min. –Potential for interspecies transmission 3 Turkey fed to dogs 1 Songer JG, et al. Anaerobe 2006; 12: Rodriguez-Palacios A, et al. EID 2007; 13: Arroyo LG, et al. J Med Microbiol 2005; 54:")
48
Defining CDAD Below the Waterline Diarrhea in older ambulatory patients +/- chronic conditions Antibiotics? NSAIDS? PPIs? H2 blockers? Dramatic, Severe Disease In Healthy, Young Persons Source: Human-to-Human and ? Antibiotic-associated Inpatient Disease ?

49
C. difficile Surveillance Potential Role –Detect disease trends –Detect outbreaks –Compare CDAD rates between institutions –Guide interventions to control CDAD –Monitor the impact of these interventions

50
CDAD Definitions CDAD –Diarrhea in a patient with a 1.Positive C. difficile laboratory assay or 2.Pseudomembranous colitis on endoscopy or surgery or 3. Pseudomembranous colitis seen on histopathology Recurrent CDAD –An episode of CDAD that occurs 8 weeks or less after the onset of a previous episode As long as the earlier episode resolved

51
Community vs. Hospital Hospitalization AdmissionDischarge 48 h CAHOCO-HCFACAIndeterminate 4 weeks8 weeks McDonald LC, et al. ICHE 2007; 28: 140-45 3 months after Discharge

52
Inpatient rates –Case patients per 10,000 patient-days Community-associated rates –Case patients per 100,000 person-years Expression of Rates McDonald LC, et al. ICHE 2007; 28: 140-45

53
Hospitals should be encouraged to conduct surveillance for CDAD –Track positive lab results (e.g. toxin A or A/B assays) –Consider measures to track outcomes Early diagnosis and treatment is important for reducing severe outcomes and should be emphasized Strict infection control: CDC fact sheet* –Contact precautions for CDAD patients –An environmental cleaning and disinfection strategy –Hand washing with CDAD patients in outbreak Recommendations for Hospitals *See C. difficile fact sheets: http://www.cdc.gov/ncidod/dhqp/
 –Consider measures to track outcomes Early diagnosis and treatment is important for reducing severe outcomes and should be emphasized Strict infection control: CDC fact sheet* –Contact precautions for CDAD patients –An environmental cleaning and disinfection strategy –Hand washing with CDAD patients in outbreak Recommendations for Hospitals *See C. difficile fact sheets:")
54
Hand Hygiene Measures Alcohol-based hand rubs are now widely used for routinely cleaning hands before/after patient care Alcohol-based hand rubs may not be effective against spore-forming organisms 1 –Several studies ongoing If an institution is experiencing an outbreak of C. difficile disease, it is prudent to wash hands with soap and water after caring for patients with CDAD 1 Weber DJ et al. JAMA 2003;289:1274

55
Impact of Hydrogen Peroxide Vapor Room Bio-Decontamination on Environmental Contamination and Nosocomial Transmission by Clostridium difficile John M. Boyce 1, MD, Nancy L. Havill 1, MT, Jonathan A. Otter 2, BSc, L. Clifford McDonald 3, MD Nicholas M.T. Adams 2, BSc, Angela Thompson 3, MSc, Lois Wiggs 3, Judith Noble-Wang 3, PhD Hospital of Saint Raphael 1, New Haven, CT Bioquell PLC 2, Andover, England Centers for Disease Control & Prevention 3, Atlanta, GA

56
Recommendations for CDAD in Previously Low-Risk Populations Further investigation and surveillance in these populations are warranted –Strains responsible for severe CDAD in previously low-risk populations are unknown but under study –May be other toxin variants and/or hospital epidemic strain Clinicians should consider the diagnosis - CDAD in patients without traditional risk factors Antimicrobial exposure is not benign –Continue to emphasize judicious antimicrobial use

57
Recommendations for Clinicians Vaccinate Get the catheters out Target the pathogen Access the experts Practice antimicrobial control Use local data Treat infection, not contamination Treat infection, not colonization Know when to say “no” to vanco Stop treatment when infection is cured or unlikely Isolate the pathogen Break the chain of contagion Campaign to Prevent Antimicrobial Resistance in Healthcare Settings

58
Recommendations for Clinicians Vaccinate Get the catheters out Target the pathogen Access the experts Practice antimicrobial control Use local data Treat infection, not contamination Treat infection, not colonization Know when to say “no” to vanco Stop treatment when infection is cured or unlikely Isolate the pathogen Break the chain of contagion Campaign to Prevent Antimicrobial Resistance in Healthcare Settings Use Antimicrobials Wisely

59
Some CDC References Campaign to Prevent Antimicrobial Resistance: 12 Steps for Healthcare Settings Management of Multidrug-Resistant Organisms in Healthcare Settings, 2006 http//:www.cdc.gov/ncidod/dhqp/index.html

60
dblossom@cdc.gov http//:www.cdc.gov/ncidod/dhqp/index.html Thank You! The information presented here represents the opinion of the presenter and does not necessarily represent the opinion of the US Public Health Service, the Centers for Disease Control and Prevention or the Department of Health and Human Services

Similar presentations





: Fast Facts. What is Clostridium difficile (C. diff)? C. diff is a bacteria that lives in the intestinal tract of about.>")



 surveillance in Colorado Kelly R. Kast, MSPH.>")

 Infections For National Patient Safety Goal 07.03.01 2009.>")





 Nebraska Public Health Laboratory 402-559-7774.>")
 Antibiotic-associated diarrhea 5-30% risk Higher with multiple IV drugs Higher with broad.>")
