Download presentation
Presentation is loading. Please wait.

1
NON-SMALL CELL LUNG CANCER: ADJUVANT AND NEOADJUVANT THERAPIES IN EARLY DISEASE MANAGEMENT Paolo Foa Dipartimento di Oncologia U. O. di Oncologia Medica A.O. San Paolo – Polo Universitario Milano

2
LA SOPRAVVIVENZA A 5 ANNI DEL NSCLC STADIO I RESECATO E’ 16 / 30 Cross-tab label 1.80-90% 2.70-80% 3.60-70% 4.50-60%

3
LA SOPRAVVIVENZA A 5 ANNI DEL NSCLC STADIO II RESECATO è 22 / 30 Cross-tab label 1.75-85% 2.65-75% 3.55-65% 4.45-55%

4
NEL NSCLC LA CHEMIOTERAPIA ADIUVANTE E’ INDICATA 24 / 30 Cross-tab label 1.IN TUTTI I CASI OPERATI 2.SOLO IN STADI DI MALATTIA SPECIFICI 3.SOLO AL DI SOTTO DI 65 ANNI DI ETA’ 4.SOLO IN ASSOCIAZIONE ALLA RADIOTERAPIA

5
IL FARMACO CARDINE NEI REGIMI DI CHEMIOTERAPIA ADIUVANTE PER IL NSCLC E’ 25 / 30 Cross-tab label 1.Carboplatino 2.Cisplatino 3.Vinorelbina 4.Gemcitabina 5.Taxolo

6
LA CHEMIOTERAPIA NEO-ADIUVANTE NEL NSCLC E’ INDICATA 25 / 30 Cross-tab label 1.IN TUTTI I CASI POTENZIALMENTE OPERABILI 2.SOLO IN STADI DI MALATTIA SPECIFICI 3.SOLO AL DI SOTTO DI 65 ANNI DI ETA’ 4.NON E’ UNO STANDARD TERAPEUTICO

7
NON-SMALL CELL LUNG CANCER (NSCLC): SURVIVAL BY STAGE
: SURVIVAL BY STAGE")
8
RESECTED NODE NEGATIVE NSCLC: PATTERN OF FAILURE Sq = squamous cell carcinoma; Non-Sq = non squamous cell carcinoma AuthorStage Patients, No. Distant Only % Feld et alT1 N0 (IA)16217 T2 N0 (IB)19630 Pairolero et alT1 N0 (IA)17015 T2 N0 (IB)15823 Thomas et alT1 N0 (IA) Sq 2267 T1 N0 (IA) Non-sq34617
16217 T2 N0 (IB)19630 Pairolero et alT1 N0 (IA)17015 T2 N0 (IB)15823 Thomas et alT1 N0 (IA) Sq 2267 T1 N0 (IA) Non-sq")
9
RESECTED NODE POSITIVE NSCLC: PATTERN OF FAILURE AuthorStage Patients, No. Distant Only % Feld et alT1 N1 (IIA)3222 Pairolero et alT1 N1 (IIA)1839 Martini et alT1-2 N1 (IIA-B) Sq 9331 T1-2 N1 (IIA-B) Non-sq 11454 T2-3 N2 (IIIA) Sq 4652 T2-3 N2 (IIIA) Non-sq 10361 Sq = squamous cell carcinoma; Non-Sq = non squamous cell carcinoma
3222 Pairolero et alT1 N1 (IIA)1839 Martini et alT1-2 N1 (IIA-B) Sq 9331 T1-2 N1 (IIA-B) Non-sq T2-3 N2 (IIIA) Sq 4652 T2-3 N2 (IIIA) Non-sq Sq = squamous cell carcinoma; Non-Sq = non squamous cell carcinoma.")
10
NON-SMALL CELL LUNG CANCER: EARLY DISEASE MANAGEMENT A SETTING FOR INTEGRATED TREATMENT SURGERY RADIOTHERAPY CHEMOTHERAPY

11
NON-SMALL CELL LUNG CANCER: EARLY DISEASE MANAGEMENT SURGERY AND CHEMOTHERAPY –SURGERY FOLLOWED BY CHEMOTHERAPY ADJUVANT SETTING –CHEMOTHERAPY FOLLOWED BY SURGERY NEO-ADJUVANT SETTING

12
RATIONALE FOR ADJUVANT THERAPY Many patients who have undergone “curative” resections actually have remaining viable tumor cells, either locally, systemically, or both. This residual microscopic tumor will, if no intervention is taken, grow and, after an interval, lead to clinically detectable disease. Treatment of clinically apparent recurrent disease is rarely curative. Survival of most pts with recurrence is short and of impaired quality. The effectiveness of any currently available anticancer treatments is inversely related to tumor burden.

13
Cancer Care Ontario and American Society of Clinical Oncology Adjuvant Chemotherapy and Adjuvant Radiation Therapy for Stages I-IIIA Resectable NSCLC Guideline Pisters K. et al Journal of Clinical Oncology 25, 5506, 2007

14
META-ANALYSIS A systematic method that uses statistical techniques for combining results from different studies with the same design to obtain a quantitative estimate of the overall effect of a particular intervention. Through such a procedure, effects which are hard or impossible to discern in the original studies because of a too small sample size can be made visible, as the meta-analysis is (in the ideal case) equivalent to a single study with the combined size of all original studies.
 equivalent to a single study with the combined size of all original studies..")
15
META-ANALYSIS Publication bias Retrospective analysis Quality of studies non homogeneous

16
Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group BMJ 311, 899, 1995 DESIGNE. Meta-analysis using updated data on 4357 pts from 14 randomised trials. Five trials used long term alkylating agents (2145 pts), mainly cyclophosphamide and nitrosourea; more recent trials (1394 pts) used cisplatin based combination chemotherapy. RESULTS. The results for long term alkylating agents show a 15% increase in the risk of death translates to an absolute detriment of chemotherapy of 4% at two years and 5% at five years. For regimens containing cisplatin most trials favour chemotherapy with a 13% reduction in the risk of death, suggesting an absolute benefit from chemotherapy of 3% at two years and 5% at five years, although on their own these results were not conclusive (p= 0.08). The essential drugs needed to achieve these effects were not identified. CONCLUSION. These results offer hope of progress and suggest that chemotherapy may have a role in treating this disease. Nevertheless, further randomised trials are still needed, especially in early disease.
, mainly cyclophosphamide and nitrosourea; more recent trials (1394 pts) used cisplatin based combination chemotherapy. RESULTS. The results for long term alkylating agents show a 15% increase in the risk of death translates to an absolute detriment of chemotherapy of 4% at two years and 5% at five years. For regimens containing cisplatin most trials favour chemotherapy with a 13% reduction in the risk of death, suggesting an absolute benefit from chemotherapy of 3% at two years and 5% at five years, although on their own these results were not conclusive (p= 0.08). The essential drugs needed to achieve these effects were not identified. CONCLUSION. These results offer hope of progress and suggest that chemotherapy may have a role in treating this disease. Nevertheless, further randomised trials are still needed, especially in early disease..")
17
Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group BMJ 311, 899, 1995 Variables5-Yr Survivalp Value Long-term alkylating agents- 5%0.005 Cisplatin-based regimens+ 5%0.08

18
Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group - BMJ 311, 899, 1995 Survival in trials of surgery versus surgery plus chemotherapy (only trials using regimens based on cisplatin)
.")
19
Chemotherapy for non-small cell lung cancer David P Carbone, John D Minna - BMJ 1995;311:889-890 … These benefits have only modest clinical impact. … The applicability of these findings to current clinical practice outside the context of clinical protocols is not clear. … For patients with early disease treated surgically the evidence does not suggest that postoperative chemotherapy can be recommended.

20
Chemotherapy for non-small cell lung cancer David P Carbone, John D Minna - BMJ 1995;311:889-890 … It is likely that only a subset of patients with non-small cell lung cancer may benefit from chemotherapy. …The toxicities, inconvenience, and expense of chemotherapy are endured by both patients whose tumours do and do not respond. …In this paper there was no evidence that any group specified by age, sex, histological findings, performance status, or stage benefited more or less from chemotherapy. … Any mechanism allowing the identification of this chemotherapy responsive subset could dramatically improve the risk benefit ratio of chemotherapy for the entire population. … Molecular biological characteristics of the tumour (for example, p53 immunostaining, ras mutation, bcl-2, and Her2/neu overexpression or as yet undiscovered markers) may provide the answer.
 may provide the answer..")
21
Adjuvant Chemotherapy for Resected NSCLC: Why We Still Don't Know S. George et al - The Oncologist 3, 35, 1998 A review of 11 cisplatin-based randomized trials addressing this issue was performed. The 11 trials were divided into those that included predominantly node-negative pts (n = 5) and those that included predominantly node-positive pts (n = 6). In the node-negative trials, which included 1,084 evaluable pts, the five-year survival rate for chemotherapy pts was 61% versus 55% for control pts (p = 0.06). In the node-positive trials, which included 880 evaluable pts, the two- year survival rate for CHT pts was 48% versus 40% for control pts (p = 0.06).
 and those that included predominantly node-positive pts (n = 6). In the node-negative trials, which included 1,084 evaluable pts, the five-year survival rate for chemotherapy pts was 61% versus 55% for control pts (p = 0.06). In the node-positive trials, which included 880 evaluable pts, the two- year survival rate for CHT pts was 48% versus 40% for control pts (p = 0.06)..")
22
Adjuvant Chemotherapy for Resected NSCLC: Why We Still Don't Know Suzanne George et al - The Oncologist 3, 35, 1998 Although non definitive, these trials suggest a marginal benefit to postoperative adjuvant CHT in resected NSCLC. However, the trials can be criticized due to: –Inadequate sample size to detect small survival benefit (larger trial 323 pts) –Heterogenous patient populations (I-III stages) –Substandard chemotherapy regimens (CAP) –Inadequate CHT delivery due to surgery more compromising and CHT more toxic than in breast and colon cancer Although current data are suggestive, they do not definitively tell us that adjuvant CHT should be the standard of care
 –Heterogenous patient populations (I-III stages) –Substandard chemotherapy regimens (CAP) –Inadequate CHT delivery due to surgery more compromising and CHT more toxic than in breast and colon cancer Although current data are suggestive, they do not definitively tell us that adjuvant CHT should be the standard of care.")
23
Consensus conference on adjuvant treatment of NSCLC M. Tonato - Lung Cancer 38, 37, 2002 A recent meta-analysis showed that the absolute risk of death was reduced by 3% at 2 yrs and by 5% at 5 yrs for pts who were treated with postoperative CDDP-based CHT. Although suggestion that postoperative CDDP-CHT may result in a slight survival improvement, adjuvant CHT in NSCLC cannot be considered a standard therapy, and it is important that large, carefully conducted, prospective randomized trials are performed. The most important cause for failure of adjuvant CHT is the presence of drug-resistant cells. New agents such as gemcitabine, vinorelbine and taxanes should be tested in the adjuvant setting in properly designed clinical trials. Four such trials are being conducted in Europe. One of them, the ALPI trial, recently completed its accrual with 1200 pts. The IALT, ANITA, and MRC trials are still ongoing.

24
Randomized study of adjuvant chemotherapy for completely resected stage I, II, or IIIA NSCLC. Scagliotti GV et al - J Natl Cancer Inst. 95, 1453, 2003 BACKGROUND: Long-term survival after surgery alone is largely unsatisfactory, and the role of adjuvant CHT has not yet been established. METHODS: 1209 pts with stage I, II, or IIIA NSCLC were assigned to mitomycin C (8 mg/m2 on day 1), VND (3 mg/m2 on days 1 and 8), and CDDP (100 mg/m2 on day 1) every 3 wks for 3 cycles (n = 606) or control (n = 603). Randomization was stratified by the intention to perform RT. The primary endpoint was OS and secondary endpoints were PFS and toxicity. RESULTS: After a median follow-up of 64.5 ms, there was no significant difference between the two groups in overall OS (50 vs 48 ms) or PFS (32 vs 29 ms). 69% of pts received the 3 planned cycles of MVP. Grades 3 and 4 neutropenia occurred in 16% and 12%, respectively, in the MVP arm. CONCLUSION: This randomized trial failed to prospectively confirm a statistically significant role for adjuvant CHT.
, VND (3 mg/m2 on days 1 and 8), and CDDP (100 mg/m2 on day 1) every 3 wks for 3 cycles (n = 606) or control (n = 603). Randomization was stratified by the intention to perform RT. The primary endpoint was OS and secondary endpoints were PFS and toxicity. RESULTS: After a median follow-up of 64.5 ms, there was no significant difference between the two groups in overall OS (50 vs 48 ms) or PFS (32 vs 29 ms). 69% of pts received the 3 planned cycles of MVP. Grades 3 and 4 neutropenia occurred in 16% and 12%, respectively, in the MVP arm. CONCLUSION: This randomized trial failed to prospectively confirm a statistically significant role for adjuvant CHT..")
25
Randomized study of adjuvant chemotherapy for completely resected stage I, II, or IIIA NSCLC. Scagliotti GV et al - J Natl Cancer Inst. 95, 1453, 2003 We collected full details about the MVP treatment received by 508 patients (93% of those randomly assigned to the MVP arm) Of the 350 patients (69%) who completed the MVP treatment, 177 did so with some dose adjustment or with omission of part of the planned regimen (mainly the elimination of vindesine administration on day 8). One hundred ten patients (22%) stopped MVP treatment early because of toxicity (66 patients; 60%) or because of personal choice (44 patients; 40%). Forty-eight patients (9%) never began MVP treatment, primarily because they withdrew their consent to participate.
 Of the 350 patients (69%) who completed the MVP treatment, 177 did so with some dose adjustment or with omission of part of the planned regimen (mainly the elimination of vindesine administration on day 8). One hundred ten patients (22%) stopped MVP treatment early because of toxicity (66 patients; 60%) or because of personal choice (44 patients; 40%). Forty-eight patients (9%) never began MVP treatment, primarily because they withdrew their consent to participate..")
26
Randomized study of adjuvant chemotherapy for completely resected stage I, II, or IIIA NSCLC. Scagliotti GV et al - J Natl Cancer Inst. 95, 1453, 2003

27
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg

28
Chemotherapy for patients with NSCLC cancer: the Big Lung Trial D. Waller et al – Eur. J. Cardio-Thoracic Surgery 26, 173, 2004 Objectives: The aim of the Big Lung Trial was to run a large pragmatic trial to confirm the survival benefits seen in the meta-analysis. Methods: 381 pts were randomised to CHT (192 pts) or control (189 pts). CHT was 3 cycles of CDDP/VND, mitomycin/ifosfamide/CDD, mitomycin/VNB/CDDP or VNR/CDDP. Baseline characteristics were: 48% squamous cell, 93% WHO PS 0-1, 28% stage I, 38% stage II, and 34% stage III. Results: In the CHT group, 13% received no CHT, 21% 1 or 2 cycles, and 64% all 3 cycles. 30% had grade 3/4 toxicity. 198 (52%) of pts have died, and there is currently no evidence of a benefit in overall survival to the CHT group: HR 1.02. Conclusions: This trial has failed to observe a survival benefit with adjuvant chemotherapy following complete resection of stage I–III NSCLC.
 or control (189 pts). CHT was 3 cycles of CDDP/VND, mitomycin/ifosfamide/CDD, mitomycin/VNB/CDDP or VNR/CDDP. Baseline characteristics were: 48% squamous cell, 93% WHO PS 0-1, 28% stage I, 38% stage II, and 34% stage III. Results: In the CHT group, 13% received no CHT, 21% 1 or 2 cycles, and 64% all 3 cycles. 30% had grade 3/4 toxicity. 198 (52%) of pts have died, and there is currently no evidence of a benefit in overall survival to the CHT group: HR Conclusions: This trial has failed to observe a survival benefit with adjuvant chemotherapy following complete resection of stage I–III NSCLC..")
29
Chemotherapy for patients with NSCLC cancer: the Big Lung Trial D. Waller et al – Eur. J. Cardio-Thoracic Surgery 26, 173, 2004

30
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg

31
Cisplatin-based Adjuvant Chemotherapy in Patients with Completely Resected Non–Small-Cell Lung Cancer The International Adjuvant Lung Cancer Trial Collaborative Group NEJM 22, 350, 2004 Background The International Adjuvant Lung Cancer Trial was designed to evaluate the effect of CDDP-based adjuvant CHT on survival after complete resection of NSCLC. Methods Pts were assigned either to 3 or 4 cycles of CDDP-based CHT or to observation. Each center determined the pathological stages to include, its CHT (the dose of cisplatin and the drug to be combined), and its postoperative RT policy. The main end point was O. S. Results 1867 pts were randomized; 36.5 % had stage I, 24.2 % stage II, and 39.3 % stage III. The drug with CDDP was VP-16 in 56.5 % of pts, VNR in 26.8 %, VNB in 11.0 %, and VND in 5.8 %. Of the 932 pts assigned to CHT, 73.8 % received at least 240 mg/sqm of cisplatin. Median duration of follow-up was 56 ms. Pts assigned to CHT had a significantly higher OS (44.5 % vs. 40.4 % at 5 ys P<0.03); they also had a significantly higher DFS (39.4 vs. 34.3 % at 5 ys P<0.003). 7 pts (0.8 %) died of CHT-induced toxic effects. Conclusions Cisplatin-based adjuvant CHT improves survival among pts with completely resected NSCLC.
, and its postoperative RT policy. The main end point was O. S. Results 1867 pts were randomized; 36.5 % had stage I, 24.2 % stage II, and 39.3 % stage III. The drug with CDDP was VP-16 in 56.5 % of pts, VNR in 26.8 %, VNB in 11.0 %, and VND in 5.8 %. Of the 932 pts assigned to CHT, 73.8 % received at least 240 mg/sqm of cisplatin. Median duration of follow-up was 56 ms. Pts assigned to CHT had a significantly higher OS (44.5 % vs % at 5 ys P<0.03); they also had a significantly higher DFS (39.4 vs % at 5 ys P<0.003). 7 pts (0.8 %) died of CHT-induced toxic effects. Conclusions Cisplatin-based adjuvant CHT improves survival among pts with completely resected NSCLC..")
32
Cisplatin-based Adjuvant Chemotherapy in Patients with Completely Resected Non–Small-Cell Lung Cancer The International Adjuvant Lung Cancer Trial Collaborative Group NEJM 22, 350, 2004

33
Cisplatin-based Adjuvant Chemotherapy in Patients with Completely Resected Non–Small-Cell Lung Cancer The International Adjuvant Lung Cancer Trial Collaborative Group NEJM 22, 350, 2004

34
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg IALTNegNegNegPos

35
Adjuvant Chemotherapy for Lung Cancer: A New Standard of Care Ronald H. Blum, M.D. - NEJM 350, 404, 2004 The finding in the IALT that CDDP-based adjuvant CHT confers an absolute increase in OS at 5 yrs of 4.1 % among pts with resected NSCLC is consistent with the benefit achieved with the use of adjuvant therapy for other cancers and represents a new standard of care For individual patients, the potential benefits of adjuvant CHT must be balanced against the risks and the inherent and understandable preferences of physicians and patients. The results of the IALT must be corroborated because this is the only trial showing a significant prolongation of OS with adjuvant CHT Only a continued commitment to well-designed, adequately powered clinical trials will allow us to gather the data necessary to make evidence- based decisions.

36
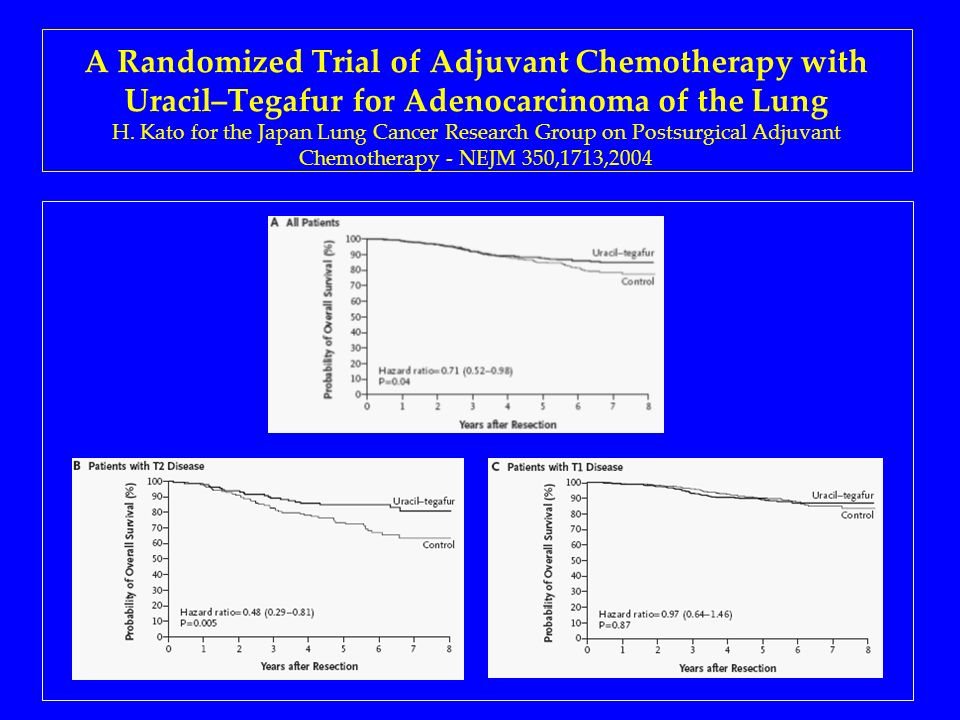
A Randomized Trial of Adjuvant Chemotherapy with Uracil–Tegafur for Adenocarcinoma of the Lung H. Kato for the Japan Lung Cancer Research Group on Postsurgical Adjuvant Chemotherapy - NEJM 350,1713,2004 Background In a previous Phase III trial of adjuvant CHT for NSCLC, a combination of uracil and tegafur (UFT) per os was shown to prolong OS. Methods Pts with completely resected pathological stage I adenocarcinoma were assigned to oral uracil–tegafur (250 mg/m2 of tegafur per day) for two yrs or control. The primary end point was OS Results 999 pts were enrolled; 491 pts received uracil–tegafur and 488 were assigned to observation. Median duration of follow-up was 73 ms. The difference in OS was statistically significant in favor of the uracil– tegafur group (P=0.04 ). The 5 ys OS was 88 % in the uracil–tegafur group and 85 % in the control group. Grade 3 toxic effects occurred in 2% of treated pts. Conclusions Adjuvant chemotherapy with uracil–tegafur improves survival among pts with completely resected pathological stage I adenocarcinoma of the lung.
 per os was shown to prolong OS. Methods Pts with completely resected pathological stage I adenocarcinoma were assigned to oral uracil–tegafur (250 mg/m2 of tegafur per day) for two yrs or control. The primary end point was OS Results 999 pts were enrolled; 491 pts received uracil–tegafur and 488 were assigned to observation. Median duration of follow-up was 73 ms. The difference in OS was statistically significant in favor of the uracil– tegafur group (P=0.04 ). The 5 ys OS was 88 % in the uracil–tegafur group and 85 % in the control group. Grade 3 toxic effects occurred in 2% of treated pts. Conclusions Adjuvant chemotherapy with uracil–tegafur improves survival among pts with completely resected pathological stage I adenocarcinoma of the lung..")
37
A Randomized Trial of Adjuvant Chemotherapy with Uracil–Tegafur for Adenocarcinoma of the Lung H. Kato for the Japan Lung Cancer Research Group on Postsurgical Adjuvant Chemotherapy - NEJM 350,1713,2004

39
Compliance 61%

40
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg IALTNegNegNegPos JLCSGNegPos--------

41
Adjuvant Chemotherapy for Adenocarcinoma of the Lung: Is the Standard of Care Ready for Change? Robert B. Diasio, M.D. Departments of Medicine and Pharmacology and Toxicology, University of Alabama NEJM 350, 1777, 2004 The study by Kato et al. provides compelling evidence that after complete resection, oral administration of uracil–tegafur, given twice daily at a dose of 250 mg of tegafur per square meter of body-surface area per day for two years, can improve survival in patients with pathological stage I adenocarcinoma of the lung. The data point to improvement particularly in patients with T2 disease. Not only was a statistically significant survival benefit shown, but also toxicity was tolerable; grade 3 or higher toxic effects developed in only 2 percent of the patients.

42
Vinorelbine plus Cisplatin vs. Observation in Resected NSCLC Timothy Winton et al for the National Cancer Institute of Canada Clinical Trials Group and the National Cancer Institute of the United States Intergroup JBR.10 New England J Medicine 352, 2589, 2005 Background We evaluated whether adjuvant VNR plus CDDP prolongs OS among pts with completely resected early-stage NSCLC Methods We randomly assigned pts with completely rested stage IB or stage II NSCLC to VNR plus CCDP for 4 cycles or to observation. The primary end point was OS; secondary end points were RFS and toxicity Results 482 pts were randomized to VNR plus CDDP (242 pts) or control (240); 45 % had stage IB and 55 % had stage II disease. Median age was 61 yrs, 65% were men, and 53% had adenoca. CHT caused neutropenia in 88% of pts (including G3 febrile neutropenia in 7%) and death from toxic effects in two pts (0.8%). Nonhematologic toxic effects of CHT were fatigue (81%), nausea (80%), anorexia (55%), vomiting (48%), neuropathy (48 %), and constipation (47%); severe (G 3 or 4) toxic effects were uncommon (<10%). 48% of pts completed cycle 4.
 or control (240); 45 % had stage IB and 55 % had stage II disease. Median age was 61 yrs, 65% were men, and 53% had adenoca. CHT caused neutropenia in 88% of pts (including G3 febrile neutropenia in 7%) and death from toxic effects in two pts (0.8%). Nonhematologic toxic effects of CHT were fatigue (81%), nausea (80%), anorexia (55%), vomiting (48%), neuropathy (48 %), and constipation (47%); severe (G 3 or 4) toxic effects were uncommon (<10%). 48% of pts completed cycle 4..")
43
Vinorelbine plus Cisplatin vs. Observation in Resected NSCLC Timothy Winton et al for the National Cancer Institute of Canada Clinical Trials Group and the National Cancer Institute of the United States Intergroup JBR.10 New England J Medicine 352, 2589, 2005 Median OS was significantly prolonged in the chemotherapy group as compared with control (94 vs. 73 ms; HR 0.69; P=0.04), as was RFS (not reached vs. 46.7 ms; HR 0.60; P<0.001). 5 yrs survival rates were 69% and 54% respectively (P=0.03), with an absolute survival benefit of 15%. Subgroup analysis did not show a significant OS improvement in stage IB disease while in stage II disease median OS was 41 ms in the control group and 80 ms in the CHT group (p= 0.004) Conclusions Adjuvant VNR plus CDDP has an acceptable level of toxicity and prolongs DFS and OS among pts with completely resected early-stage NSCLC.
, as was RFS (not reached vs ms; HR 0.60; P<0.001). 5 yrs survival rates were 69% and 54% respectively (P=0.03), with an absolute survival benefit of 15%. Subgroup analysis did not show a significant OS improvement in stage IB disease while in stage II disease median OS was 41 ms in the control group and 80 ms in the CHT group (p= 0.004) Conclusions Adjuvant VNR plus CDDP has an acceptable level of toxicity and prolongs DFS and OS among pts with completely resected early-stage NSCLC..")
44
Vinorelbine plus Cisplatin vs. Observation in Resected NSCLC New England J Medicine 352, 2589, 2005

45
Vinorelbine plus Cisplatin vs. Observation in Resected NSCLC Timothy Winton et al for the National Cancer Institute of Canada Clinical Trials Group and the National Cancer Institute of the United States Intergroup JBR.10 New England J Medicine 352, 2589, 2005

46
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg IALTNegNegNegPos JLCSGNegPos-------- NCIC----NegPos----

47
Adjuvant Chemotherapy for Non–Small-Cell Lung Cancer The Smoke Clears K. Pisters – New England J Medicine 352, 2640, 2005 This is the first trial to treat all enrolled patients with a “third generation” chemotherapy agent such as VNR On the basis of the data reported by Winton et al the controversy surrounding adjuvant chemotherapy for resectable NSCLC is over. Adjuvant platinum-based chemotherapy should be recommended after complete resection of NSCLC in patients with a good performance status. Additional research will enable us to select those patients most likely to benefit from adjuvant therapy, to customize the therapy on the basis of the biology of the tumor, to lessen toxicity and increase compliance, to identify more effective regimens, and to further improve survival.

48
Adjuvant VNR plus CDDP versus observation in patients with completely resected stage IB–IIIA NSCLC: a randomized trial (Adjuvant Navelbine International Trialist Association) Douillard J. Y. et al – Lancet Oncology 7, 719, 2006 BACKGROUND: We aimed to compare the effect of adjuvant VNR plus CDDP versus observation on survival in pts with completely resected NSCLC. METHODS: 840 pts with stage IB–IIIA NSCLC were assigned to observation (n=433) or to 30 mg/m2 VNR plus 100 mg/m2 CDDP (n=407). Postoperative RT was undertaken according to every centre's policy. The primary endpoint was OS. RESULTS: 90% of pts in the CHT group received CHT. 36% had IB, 24% had II and 39% had IIIA disease. Toxicity: 92% of pts had neutropenia, 9% had febrile neutropenia; 2% toxic deaths were recorded. At a median follow-up of 76 ms median survival was 65.7 ms in the CHT group and 43.7 ms in the control group. Risk for death was significantly reduced in pts assigned to CHT (HR 0·80; p=0·017). OS at 5 yrs with CHT improved by 8.6% (IB 62% vs 64% (HR 1.1); II 52% vs 39% ( HR0.71); IIIA 42% vs 26% (HR0.69) INTERPRETATION: Adjuvant VNR plus CDDP extends survival in pts with completely resected NSCLC
 or to 30 mg/m2 VNR plus 100 mg/m2 CDDP (n=407). Postoperative RT was undertaken according to every centre s policy. The primary endpoint was OS. RESULTS: 90% of pts in the CHT group received CHT. 36% had IB, 24% had II and 39% had IIIA disease. Toxicity: 92% of pts had neutropenia, 9% had febrile neutropenia; 2% toxic deaths were recorded. At a median follow-up of 76 ms median survival was 65.7 ms in the CHT group and 43.7 ms in the control group. Risk for death was significantly reduced in pts assigned to CHT (HR 0·80; p=0·017). OS at 5 yrs with CHT improved by 8.6% (IB 62% vs 64% (HR 1.1); II 52% vs 39% ( HR0.71); IIIA 42% vs 26% (HR0.69) INTERPRETATION: Adjuvant VNR plus CDDP extends survival in pts with completely resected NSCLC.")
49
Adjuvant VNR plus CDDP versus observation in patients with completely resected stage IB–IIIA NSCLC: a randomized trial (Adjuvant Navelbine International Trialist Association) Douillard J. Y. et al – Lancet Oncology 7, 719, 2006

51
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg IALTNegNegNegPos JLCSGNegPos-------- NCIC----NegPos---- ANITA----NegPosPos

52
Adjuvant chemotherapy for resected NSCLC: ANITA takes the stage C. G. Azzoli – Lancet Oncology 7, 701, 2006 The spotlight is now on the prescription of adjuvant treatment for patients with resected NSCLC. Nearly every patient with resectable NSCLC should be referred to a medical oncologist for consideration of adjuvant chemotherapy. Hopefully, many more patients will be enrolled into clinical trials investigating new adjuvant treatments, and will be assigned on the basis of the molecular characteristics of the tumour. In the next few years, the spotlight is likely to move towards targeted drugs and tumour-tissue analysis.

53
Adjuvant Paclitaxel Plus Carboplatin Compared With Observation in Stage IB Non–Small-Cell Lung Cancer: CALGB 9633 Strauss G. M. et al - Journal Clinical Oncology, 26, 5043, 2008 PURPOSE: Utility of adjuvant CHT in resected NSCLC stage IB is yet unclear. Methods: Pts with pT2N0 NSCLC (IB)were assigned to adjuvant CHT (paclitaxel 200 mg/m2 i.v. over 3 hrs and carboplatin at an AUC 6 i.v. over 60 mnts every 3 wks for 4 cycles) or observation. The primary end point was OS. Results 343 pts were enrolled. Median follow-up was 74 ms. Grades 3 to 4 neutropenia were the main toxicity; there were no treatment-related deaths. OS was not different (HR 0.83; P =.12). Exploratory analysis demonstrated a significant OS difference for pts who had tumors > 4 cm in diameter (HR 0.69; P =0.043). Conclusion Adjuvant CHT should not be considered standard care in stage IB NSCLC. A statistically significant survival advantage for pts who had tumors > 4 cm supports consideration of adjuvant paclitaxel/carboplatin for stage IB patients who have large tumors
were assigned to adjuvant CHT (paclitaxel 200 mg/m2 i.v. over 3 hrs and carboplatin at an AUC 6 i.v. over 60 mnts every 3 wks for 4 cycles) or observation. The primary end point was OS. Results 343 pts were enrolled. Median follow-up was 74 ms. Grades 3 to 4 neutropenia were the main toxicity; there were no treatment-related deaths. OS was not different (HR 0.83; P =.12). Exploratory analysis demonstrated a significant OS difference for pts who had tumors > 4 cm in diameter (HR 0.69; P =0.043). Conclusion Adjuvant CHT should not be considered standard care in stage IB NSCLC. A statistically significant survival advantage for pts who had tumors > 4 cm supports consideration of adjuvant paclitaxel/carboplatin for stage IB patients who have large tumors.")
54
Adjuvant Paclitaxel Plus Carboplatin Compared With Observation in Stage IB Non–Small-Cell Lung Cancer: CALGB 9633 Strauss G. M. et al - Journal Clinical Oncology, 26, 5043, 2008

55
Adjuvant Paclitaxel Plus Carboplatin Compared With Observation in Stage IB Non–Small-Cell Lung Cancer: CALGB 9633 Strauss et al – ASCO 2004, Abst 7019 Background: CALGB 9633 was designed to test the effectiveness of adjuvant CHT in pts with stage IB resected NSCLC. Methods: Pts were randomized to adjuvant CHT with paclitaxel 200 mg/m2 over 3 hrs and carboplatin AUC 6 on day 1 every 3 wks for 4 cycles, or to observation. Results: 344 pts were randomized. Median follow-up is currently 34 ms. Adjuvant CHT was well tolerated, and there were no CHT-related toxic deaths. There was a significant advantage in RFS favoring the CHT group (HR=0.69; p=0.035). With regard to lung cancer mortality, there have been 19 deaths in the CHT group and 34 deaths in the control group (HR=0.51; p=0.018). At 4 yrs, lung cancer mortality was 15% and 26% in CHT and control groups, respectively. Conclusions: Adjuvant CHT significantly reduces lung cancer mortality in stage IB NSCLC.
. With regard to lung cancer mortality, there have been 19 deaths in the CHT group and 34 deaths in the control group (HR=0.51; p=0.018). At 4 yrs, lung cancer mortality was 15% and 26% in CHT and control groups, respectively. Conclusions: Adjuvant CHT significantly reduces lung cancer mortality in stage IB NSCLC..")
56
ADJUVANT CHEMOTHERAPY FOR NSCLC IAIBIIIIIA ALPINegNegNegNeg BLTNegNegNegNeg IALTNegNegNegPos JLCSGNegPos-------- NCIC----NegPos---- ANITA----NegPosPos CALGB----Pos--------

57
Adjuvant Chemotherapy for Non–Small-Cell Lung Cancer: A Fading Effect? B. Besse, T. Le Chevalier - Journal of Clinical Oncology 26, 5014, 2008 Is the benefit of adjuvant chemotherapy transient? –Long-term follow-up in all recent randomized adjuvant trials in NSCLC should be carefully considered. Should we propose adjuvant chemotherapy for stage IB patients? –The 4-cm cutoff in tumor size suggested in the subgroup analysis of CALGB 9633 may represent a reasonable limit for an adjuvant treatment. Is the paclitaxel-carboplatin an optimal regimen? –Cisplatin should be the platinum compound of choice in the adjuvant setting, unless there are medical contraindications. Should we wait for biomarkers analysis before our final decision? –Biomarkers may predict for the benefit of selected regimens.

58
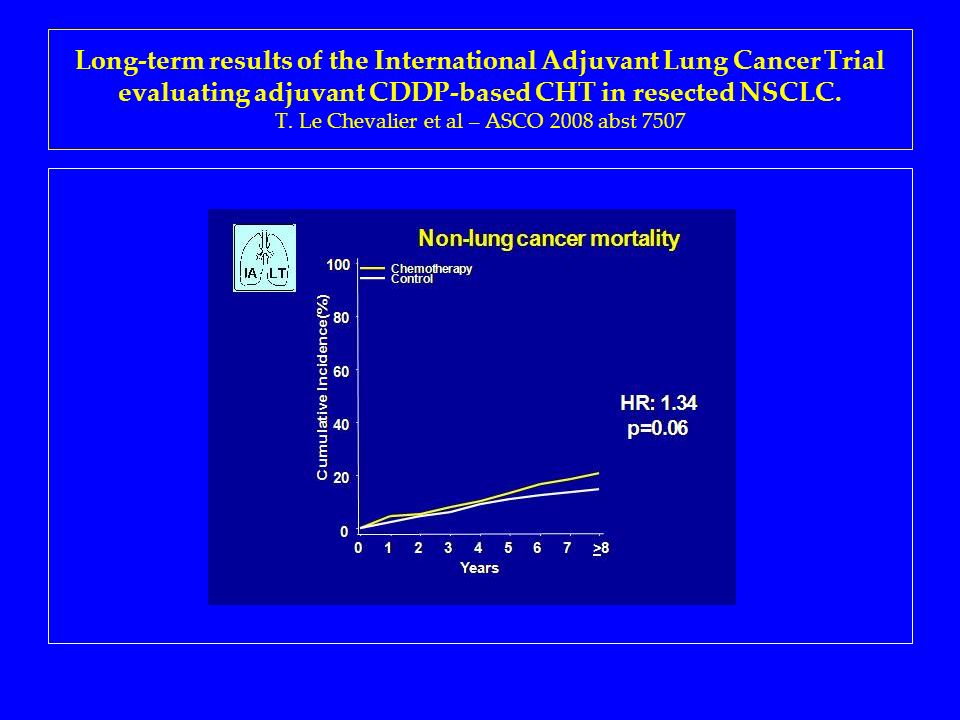
Background: We evaluated the results of the IALT study, initially reported with a 4.7 year follow-up, with 3 additional years of follow-up. Methods: Pts with completely resected NSCLC were assigned to 3 or 4 cycles of CDDP-based CHT or observation. Results: 1,867 pts were included. There was a significant difference between OS benefit before and after 5 years (first 5 yrs HR: 0.86; p = 0.01 versus HR: 0.91; p =0.10). DFS benefit was also different (first 5 yrs, HR=0.85, p=0.006; after 5 yrs, HR=0.88, p=0.02). Conclusions: The difference in results between less than and more than 5 yrs of follow-up may suggest possible late CHT-related over-mortality. This potential effect underscores the need for the long-term follow-up of adjuvant lung cancer trials in order to evaluate results in terms of treatment benefits and long-term hazards. Long-term results of the International Adjuvant Lung Cancer Trial evaluating adjuvant CDDP-based CHT in resected NSCLC. T. Le Chevalier et al – ASCO 2008 abst 7507
. DFS benefit was also different (first 5 yrs, HR=0.85, p=0.006; after 5 yrs, HR=0.88, p=0.02). Conclusions: The difference in results between less than and more than 5 yrs of follow-up may suggest possible late CHT-related over-mortality. This potential effect underscores the need for the long-term follow-up of adjuvant lung cancer trials in order to evaluate results in terms of treatment benefits and long-term hazards. Long-term results of the International Adjuvant Lung Cancer Trial evaluating adjuvant CDDP-based CHT in resected NSCLC. T. Le Chevalier et al – ASCO 2008 abst")
60
CALGB AND IALT STUDIES: OUTCOME BY TIME

61
Surgery and adjuvant CHTcompared to surgery alone in NSCLC: A meta-analysis using individual patient data from RCTs. L. A. Stewart et al for NSCLC Collaborative Group – ASCO 2007 abst 7552 Background: We report on the effectiveness of surgery plus adjuvant CHT compared with surgery alone. Methods: We conducted a systematic search for RCT. Previously included RCT using long-term alkylating agents were excluded. Results: IPD were obtained on 8147 pts from 30 RCTs. 15 RCTs used a CDDP combination without Tegafur/UFT, 8 RCTs used Tegafur/UFT without CDDP and 7 RCTs used Tegafur/UFT and CDDP. This adds 18 trials and 5835 patients to the 1995 analyses. The results show a highly significant benefit of CT on survival (HR=0.86, p<0.000001), with an absolute benefit of 4% (from 60% to 64%) at 5 years. There was no difference in effect by type of CT, age, sex or histology. There was a suggestion of a trend in effect by stage (p=0.047); this will be explored further. Conclusion: The results demonstrate conclusively and consistently a benefit of adjuvant CHT in resected NSCLC.
, with an absolute benefit of 4% (from 60% to 64%) at 5 years. There was no difference in effect by type of CT, age, sex or histology. There was a suggestion of a trend in effect by stage (p=0.047); this will be explored further. Conclusion: The results demonstrate conclusively and consistently a benefit of adjuvant CHT in resected NSCLC..")
62
Surgery and adjuvant CHTcompared to surgery alone in NSCLC: A meta-analysis using individual patient data from RCTs. L. A. Stewart et al for NSCLC Collaborative Group – ASCO 2007 abst 7552 Outcome Hazard Ratio (95% CI)p-valueNumber of trials Overall Survival 0.86 (0.81–0.93)<0.00000130 Recurrence free survival 0.83 (0.77–0.91)0.0000114 Local recurrence free interval 0.76 (0.66–0.87)0.0000612 Distant recurrence free interval 0.83 (0.74–0.93)0.00112
p-valueNumber of trials Overall Survival 0.86 (0.81–0.93)< Recurrence free survival 0.83 (0.77–0.91) Local recurrence free interval 0.76 (0.66–0.87) Distant recurrence free interval 0.83 (0.74–0.93)")
63
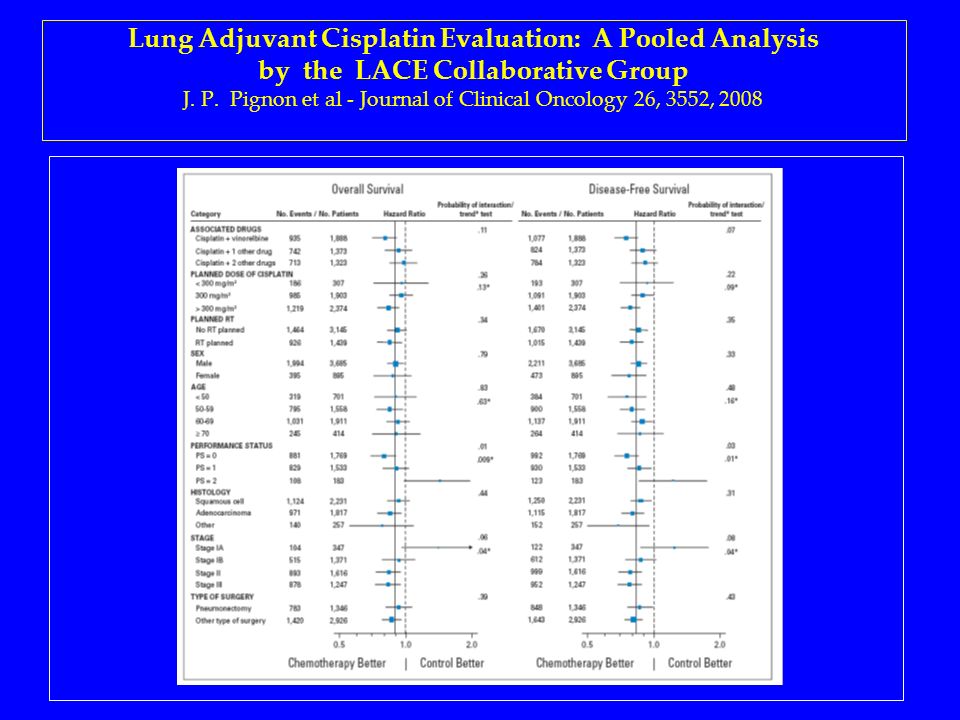
Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group J. P. Pignon et al - Journal of Clinical Oncology 26, 3552, 2008 PURPOSE: The aim of the LACE study was to identify treatment options associated with a higher benefit or groups of pts who particularly benefit from postoperative CHT. PATIENTS AND METHODS: Individual pts data were pooled from the 5 largest trials (4,584 pts) of CDDP-based CHT in completely resected pts after the 1995 NSCLC meta-analysis. RESULTS: With a median follow-up time of 5.2 yrs, the overall HR of death was 0.89 (P =.005), corresponding to a 5-year absolute benefit of 5.4% from CHT. The benefit varied with stage (HR for stage IA = 1.40; for stage IB = 0.93; for stage II = 0.83; for stage III = 0.83). The effect of CHT did not vary significantly with the associated drugs, including vinorelbine (HR = 0.80), etoposide or vinca alkaloid (HR = 0.92), or other (HR = 0.97). CHT effect was higher in pts with better PS. There was no interaction between CHT effect and sex, age, histology, type of surgery, planned RT, or planned total dose of CDDP. CONCLUSION: Postoperative CDDP-based CHT significantly improves survival in patients with NSCLC.
 of CDDP-based CHT in completely resected pts after the 1995 NSCLC meta-analysis. RESULTS: With a median follow-up time of 5.2 yrs, the overall HR of death was 0.89 (P =.005), corresponding to a 5-year absolute benefit of 5.4% from CHT. The benefit varied with stage (HR for stage IA = 1.40; for stage IB = 0.93; for stage II = 0.83; for stage III = 0.83). The effect of CHT did not vary significantly with the associated drugs, including vinorelbine (HR = 0.80), etoposide or vinca alkaloid (HR = 0.92), or other (HR = 0.97). CHT effect was higher in pts with better PS. There was no interaction between CHT effect and sex, age, histology, type of surgery, planned RT, or planned total dose of CDDP. CONCLUSION: Postoperative CDDP-based CHT significantly improves survival in patients with NSCLC..")
64
Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group J. P. Pignon et al - Journal of Clinical Oncology 26, 3552, 2008

66
Cancer Care Ontario and American Society of Clinical Oncology Adjuvant Chemotherapy and Adjuvant Radiation Therapy for Stages I-IIIA Resectable Non–Small-Cell Lung Cancer Guideline Pisters K. et al - Journal of Clinical Oncology 25, 5506, 2007

67
A LOOK AT THE FUTURE

68
ADJUVANT CHEMOTHERAPY FOR RESECTED NSCLC: A TARGETED APPROACH THE TUMOR THE DRUG

69
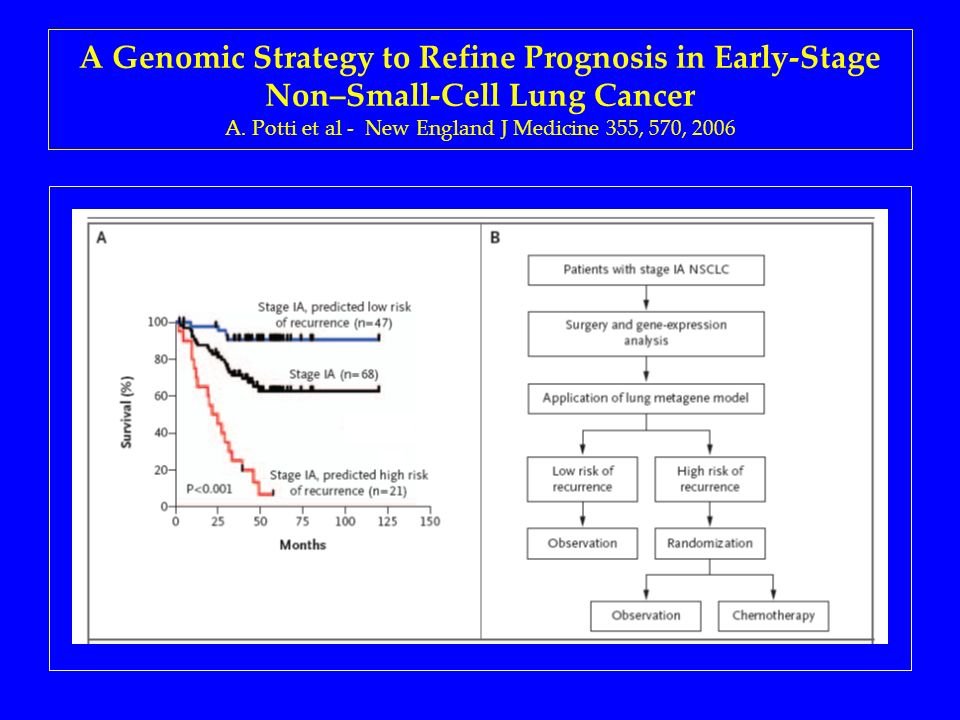
A Genomic Strategy to Refine Prognosis in Early-Stage Non–Small-Cell Lung Cancer A. Potti et al - New England J Medicine 355, 570, 2006 Background Adjuvant CHT benefits pts with stage IB, II, or IIIA but not stage IA NSCLC. Indeed 25 % of pts with stage IA disease have a recurrence after surgery, suggesting the need for more effective therapy. Methods We identified gene-expression profiles predicting the risk of recurrence in a cohort of 89 pts with early-stage NSCLC. We evaluated the predictor in 25 pts from the ACOSOG Z0030 and 84 pts from the CALGB 9761 study. Results The model predicted recurrence significantly better than did clinical prognostic factors and was consistent across all early stages. Applied to the ACOSOG Z0030 trial and the CALGB 9761 trial had an overall predictive accuracy of 72 % and 79 % respectively. It also identified a subgroup of pts with stage IA disease at high risk for recurrence who might benefit from adjuvant CHT. Conclusions The model provides a potential mechanism to refine the estimation of a pnt's risk of recurrence and, in principle, to alter decisions regarding the use of adjuvant CHT in early-stage NSCLC.

70
A Genomic Strategy to Refine Prognosis in Early-Stage Non–Small-Cell Lung Cancer A. Potti et al - New England J Medicine 355, 570, 2006

72
DNA Repair by ERCC1 in Non–Small-Cell Lung Cancer and Cisplatin-Based Adjuvant Chemotherapy Ken A. Olaussen et al – New England J Medicine 355, 983, 2006 Background Adjuvant CDDP-based CHT improves survival in pts with resected NSCLC but there is no validated predictor for benefit of CHT. Methods We used immunohistochemical analysis to determine the expression of the excision repair cross-complementation group 1 (ERCC1) protein in operative specimens of pts enrolled in the IALT trial. Results ERCC1 expression was positive in 44% of cases. A benefit from CDDP-based adjuvant CHT was associated with the absence of ERCC1. Adjuvant CHT, as compared with control, significantly prolonged OS among pts with ERCC1-negative tumors (HR 0.65; P=0.002) but not among pts with ERCC1-positive tumors (HR 1.14; P=0.40). Conclusions Pts with resected NSCLC and ERCC1-negative tumors appear to benefit from adjuvant CDDP-based CHT, whereas pts with ERCC1-positive tumors do not
 protein in operative specimens of pts enrolled in the IALT trial. Results ERCC1 expression was positive in 44% of cases. A benefit from CDDP-based adjuvant CHT was associated with the absence of ERCC1. Adjuvant CHT, as compared with control, significantly prolonged OS among pts with ERCC1-negative tumors (HR 0.65; P=0.002) but not among pts with ERCC1-positive tumors (HR 1.14; P=0.40). Conclusions Pts with resected NSCLC and ERCC1-negative tumors appear to benefit from adjuvant CDDP-based CHT, whereas pts with ERCC1-positive tumors do not.")
73
DNA Repair by ERCC1 in Non–Small-Cell Lung Cancer and Cisplatin-Based Adjuvant Chemotherapy Ken A. Olaussen et al – New England J Medicine 355, 983, 2006

74
Cell cycle regulators and outcome of adjuvant cisplatin-based chemotherapy in completely resected non-small-cell lung cancer. M. Filipits – J Clin Oncol 25, 2735, 2007 PURPOSE: To determine whether cell cycle regulators are of prognostic and/or predictive value in pts enrolled in the IALT trial. PATIENTS AND METHODS: Expression of p27Kip1, p16INK4A, cyclin D1, cyclin D3, cyclin E, and Ki-67 was immunohistochemically assessed in tumor specimens. RESULTS: There was a relationship between p27Kip1 status and benefit of CDDP-based CHT (test for interaction, P =.02). Among pts with p27Kip1-negative tumors a longer OS in treated compared with control pts was recorded (HR 0.66; P =.006). In pts with p27Kip1-positive tumors, OS was not different (HR 1.09; P =.54). The other cell cycle regulators and Ki-67 did not predict benefit of adjuvant cisplatin-based chemotherapy. CONCLUSION: NSCLC pts with p27Kip1-negative tumors benefit from adjuvant CDDP-based CHT. p27Kip1 downregulation may contribute to CHT sensitivity by the following two ways: cell cycle transition delay and increased susceptibility to apoptosis.
. Among pts with p27Kip1-negative tumors a longer OS in treated compared with control pts was recorded (HR 0.66; P =.006). In pts with p27Kip1-positive tumors, OS was not different (HR 1.09; P =.54). The other cell cycle regulators and Ki-67 did not predict benefit of adjuvant cisplatin-based chemotherapy. CONCLUSION: NSCLC pts with p27Kip1-negative tumors benefit from adjuvant CDDP-based CHT. p27Kip1 downregulation may contribute to CHT sensitivity by the following two ways: cell cycle transition delay and increased susceptibility to apoptosis..")
75
Cell cycle regulators and outcome of adjuvant cisplatin-based chemotherapy in completely resected non-small-cell lung cancer. M. Filipits – J Clin Oncol 25, 2735, 2007

76
NEO-AADIUVANT CHEMOTHERAPY: RATIONALE DOWNSTAGING EARLY TREATMENT OF MICROMETASTASES BETTER TOLERABILITY

77
NEO-AADIUVANT CHEMOTHERAPY A systemic review and meta-analysis of the literature: chemotherapy and surgery versus surgery alone in NSCLC Burdett S. et al - MRC Clinical Trials Unit J Thorac Oncol 1, 612, 2006

78
A systemic review and meta-analysis of the literature: chemotherapy and surgery versus surgery alone in NSCLC Burdett S. et al - MRC Clinical Trials Unit – J Thorac Oncol 1, 612, 2006 BACKGROUND: The effectiveness of preoperative CHT in the treatment of NSCLC has remained unclear despite the conduct of several RCTs METHODS: A systematic review and meta-analysis was carried out. RESULTS: 7 RCTs, including 988 patients could be combined. Preoperative CHT improved survival with a HR of 0.82 (p = 0.02), equivalent to an absolute benefit of 6%, increasing OS across all stages of disease from 14% to 20% at 5 yrs. CONCLUSIONS: This analysis shows a significant benefit of preoperative CHT, but this is based on a small number of trials and pts. This current analysis was unable to address important questions such as whether particular types of pts may benefit more or less from preoperative CHT or whether the early stopping of a number of RCTs impacted on the results.
, equivalent to an absolute benefit of 6%, increasing OS across all stages of disease from 14% to 20% at 5 yrs. CONCLUSIONS: This analysis shows a significant benefit of preoperative CHT, but this is based on a small number of trials and pts. This current analysis was unable to address important questions such as whether particular types of pts may benefit more or less from preoperative CHT or whether the early stopping of a number of RCTs impacted on the results..")
79
A systemic review and meta-analysis of the literature: chemotherapy and surgery versus surgery alone in NSCLC Burdett S. et al - MRC Clinical Trials Unit – J Thorac Oncol 1, 612, 2006

80
A randomized trial comparing perioperative chemotherapy and surgery with surgery alone in resectable stage IIIA non-small-cell lung cancer. J. A. Roth et al - J Natl Cancer Inst 86, 673, 1994 We performed a prospective, randomized study of pts with previously untreated, potentially resectable clinical stage IIIA non-small-cell lung cancer to compare the results of perioperative chemotherapy and surgery with those of surgery alone. In total, 60 pts were randomly assigned to receive either six cycles of perioperative chemotherapy (cyclophosphamide, etoposide, and cisplatin) and surgery (28 patients) or surgery alone (32 patients). After three cycles of preoperative chemotherapy, the rate of clinical major response was 35%. Patients treated with perioperative chemotherapy and surgery had an estimated median survival of 64 ms compared with 11 ms for pts who had surgery alone (P <.008).
 and surgery (28 patients) or surgery alone (32 patients). After three cycles of preoperative chemotherapy, the rate of clinical major response was 35%. Patients treated with perioperative chemotherapy and surgery had an estimated median survival of 64 ms compared with 11 ms for pts who had surgery alone (P <.008)..")
81
A randomized trial comparing perioperative chemotherapy and surgery with surgery alone in resectable stage IIIA non-small-cell lung cancer. J. A. Roth et al - J Natl Cancer Inst 86, 673, 1994 The estimated 2- and 3-year survival rates were 60% and 56% for the perioperative chemotherapy patients and 25% and 15% for those who had surgery alone, respectively. This clinical trial strengthens the validity of using perioperative chemotherapy in the management of patients with resectable stage IIIA non-small-cell lung cancer. Further investigation of the perioperative chemotherapy strategy in earlier stage lung cancer is warranted.

82
Chemotherapy for resectable stage IIIA NSCLC: can that dog hunt? D. H. Johnson et al – J Natl cancer Inst 86. 650, 1994 Data must be interpreted with caution The magnitude of survival advantage exceeds what one might realistically expect according to the response rate Reservation has to be raised concerning the early termination of the study The earlier a trial is terminated, the larger a bias can be Uneven distribution of unrecognized biological prognostic factors Larger confirmatory trials are necessary before this approach is adopted

83
Preoperative Chemotherapy Followed by Surgery Compared With Primary Surgery in Resectable Stage I (Except T1N0), II, and IIIa NSCLC A. Depierre et al - J Clin Oncol 20, 247, 2002 PURPOSE: To evaluate whether PCT could improve survival in resectable stage I (except T1N0), II, and IIIA NSCLC. PATIENTS AND METHODS: The trial compared PCT to PRS. PCT consisted of 2 cycles of mitomycin (6 mg/m2, day 1), ifosfamide (1.5 g/m2, days 1 to 3) and CDDP (30 mg/m2, days 1 to 3), and 2 additional postoperative cycles for responding patients. In both arms, patients with pT3 or pN2 disease received thoracic radiotherapy. RESULTS: 355 pts were randomized. Overall response to PCT was 64%. There were two preoperative toxic deaths. Postoperative mortality was 6.7% in the PCT arm and 4.5% in the PRS arm (P =.38). Median survival was 37 ms for PCT and 26.0 ms for PRS (P =.15). Survival differences between arms increased from 3.8% at 1 year to 8.6% at 4 years. A quantitative interaction between N status and treatment was observed, with benefit confined to N0 to N1 disease. The effect of PCT was significantly favorable on OS (HR 0.74; P =.044). DFS was significantly longer in the PCT arm (P =.033). CONCLUSION: Although impressive differences in median, 3-year, and 4-year survival were observed, they were not statistically significant, except for stage I and II disease.
, II, and IIIA NSCLC. PATIENTS AND METHODS: The trial compared PCT to PRS. PCT consisted of 2 cycles of mitomycin (6 mg/m2, day 1), ifosfamide (1.5 g/m2, days 1 to 3) and CDDP (30 mg/m2, days 1 to 3), and 2 additional postoperative cycles for responding patients. In both arms, patients with pT3 or pN2 disease received thoracic radiotherapy. RESULTS: 355 pts were randomized. Overall response to PCT was 64%. There were two preoperative toxic deaths. Postoperative mortality was 6.7% in the PCT arm and 4.5% in the PRS arm (P =.38). Median survival was 37 ms for PCT and 26.0 ms for PRS (P =.15). Survival differences between arms increased from 3.8% at 1 year to 8.6% at 4 years. A quantitative interaction between N status and treatment was observed, with benefit confined to N0 to N1 disease. The effect of PCT was significantly favorable on OS (HR 0.74; P =.044). DFS was significantly longer in the PCT arm (P =.033). CONCLUSION: Although impressive differences in median, 3-year, and 4-year survival were observed, they were not statistically significant, except for stage I and II disease..")
84
Preoperative Chemotherapy Followed by Surgery Compared With Primary Surgery in Resectable Stage I (Except T1N0), II, and IIIa NSCLC A. Depierre et al - J Clin Oncol 20, 247, 2002

85
A phase III trial of surgery alone or surgery plus preoperative (preop) paclitaxel/carboplatin (PC) in early stage NSCLC. Pisters K. Et al – ASCO 2005, Abst 7012 Background: SWOG-9900 was undertaken to determine whether preop PC could improve survival compared to surgery alone. Methods: Pts with clinical stage T2N0, T1-2N1, and T3N0-1 NSCLC were randomized to preop PC (P:225 mg/m2 over 3 hrs, AUC=6) on day 1, every 3 wks x 3 or surgery alone. Results: 354 pts were accrued; 174-surgery alone, 180-preop PC. 70% IB/IIA, 30% IIB/IIIA. PFS: median 29 mo vs 20 mo, HR 0.85, p=0.26. OS: 42 vs 37 mo, HR 0.88, p=0.47. Conclusions: This study is one of the largest randomized trials examining preop chemotherapy in ES NSCLC. PFS and OS trends favor preop PC, supporting role of chemotherapy in ES NSCLC. Randomized trials comparing preop to adjuvant chemotherapy are warranted.
 on day 1, every 3 wks x 3 or surgery alone. Results: 354 pts were accrued; 174-surgery alone, 180-preop PC. 70% IB/IIA, 30% IIB/IIIA. PFS: median 29 mo vs 20 mo, HR 0.85, p=0.26. OS: 42 vs 37 mo, HR 0.88, p=0.47. Conclusions: This study is one of the largest randomized trials examining preop chemotherapy in ES NSCLC. PFS and OS trends favor preop PC, supporting role of chemotherapy in ES NSCLC. Randomized trials comparing preop to adjuvant chemotherapy are warranted..")
86
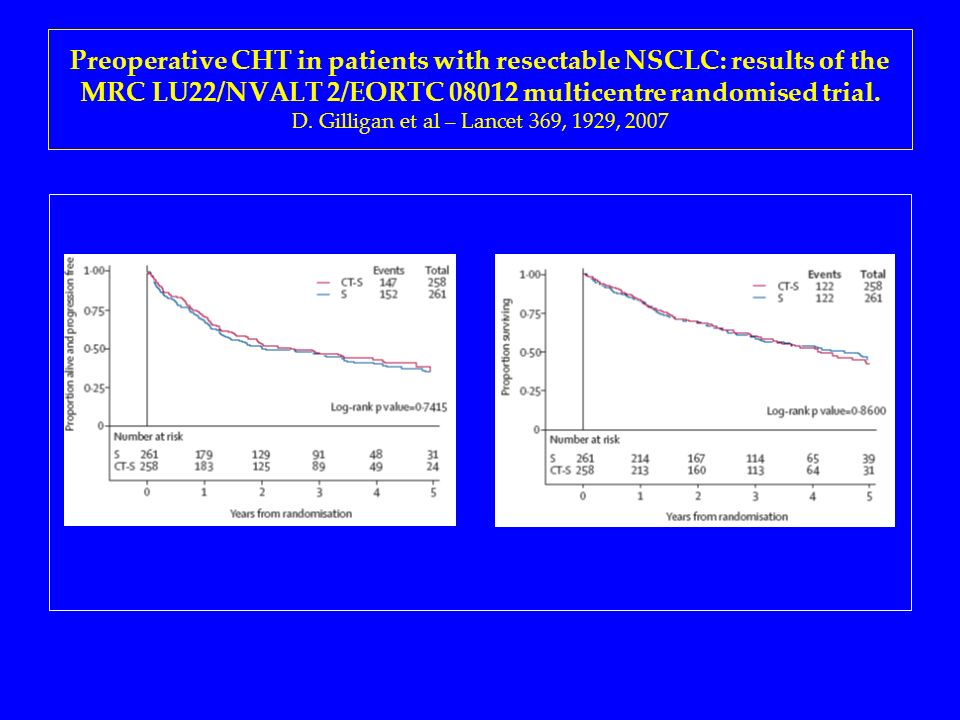
Preoperative CHT in patients with resectable NSCLC: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial. D. Gilligan et al – Lancet 369, 1929, 2007 BACKGROUND: Our intergroup randomized trial was designed to investigate whether in pts with operable NSCLC of any stage outcomes could be improved by CDDP-based CHT. METHODS: Pts were randomised to receive either surgery alone (S), or three cycles of CHT followed by surgery surgery. RESULTS: 519 pts were randomised. 61% were clinical stage I, 31% stage II, and 7% stage III. 75% of pts received all 3 cycles of CHT with a RR of 49% and down-staging of 31%. However, there was no evidence of a benefit in terms of OS (HR 1.02, p=0.86). INTERPRETATION: Although there was no evidence of a difference in OS with neo-adjuvant CHT, the result is statistically consistent with previous trials.
, or three cycles of CHT followed by surgery surgery. RESULTS: 519 pts were randomised. 61% were clinical stage I, 31% stage II, and 7% stage III. 75% of pts received all 3 cycles of CHT with a RR of 49% and down-staging of 31%. However, there was no evidence of a benefit in terms of OS (HR 1.02, p=0.86). INTERPRETATION: Although there was no evidence of a difference in OS with neo-adjuvant CHT, the result is statistically consistent with previous trials..")
87
Preoperative CHT in patients with resectable NSCLC: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial. D. Gilligan et al – Lancet 369, 1929, 2007

89
Chemotherapy and surgery for operable NSCLC P A Bradbury, F A Shepherd - Lancet 369, 1903, 2007 While a systematic review indicates a potential benefit from preoperative chemotherapy, the body of evidence to date favours postoperative chemotherapy. We recommend that surgery, the most important component of combined modality treatment for early-stage NSCLC, not be delayed, and that systemic treatments should be administered postoperatively

90
The Neo-Adjuvant Taxol Carboplatin Hope Trial (NATCH-TRIAL) E Felip et al – ASCO 2007, 7578 Background: The NATCH trial was designed to address whether neoadjuvant or adjuvant paclitaxel (P)/carboplatin (C) improves DFS compared to surgery alone in early-stage NSCLC. Methods: Pts with stage I (>2 cm), II, T3N1 NSCLC are randomized to surgery alone or 3 cycles of neoadjuvant PC, or surgery followed by 3 cycles of adjuvant PC. Sample size is 628 pts. Results: 616 pts have been accrued, 7% stage IA, 64% IB, 2% IIA, 24% IIB, 2.5% T3N1. Neoadjuvant CHT has been well tolerated. Major radiographic response has been observed in 59% of pts and progression during chemotherapy occurred in 6%. At surgery, 9% pts had pathologic complete response, 75% N0-1 disease with persistent T tumor, and 15% pathologic N2 disease. Conclusion: Neoadjuvant chemotherapy in early NSCLC has proven feasible and safe in this large multicenter sample. Mature survival results of the NATCH trial are expected in 2009.
, II, T3N1 NSCLC are randomized to surgery alone or 3 cycles of neoadjuvant PC, or surgery followed by 3 cycles of adjuvant PC. Sample size is 628 pts. Results: 616 pts have been accrued, 7% stage IA, 64% IB, 2% IIA, 24% IIB, 2.5% T3N1. Neoadjuvant CHT has been well tolerated. Major radiographic response has been observed in 59% of pts and progression during chemotherapy occurred in 6%. At surgery, 9% pts had pathologic complete response, 75% N0-1 disease with persistent T tumor, and 15% pathologic N2 disease. Conclusion: Neoadjuvant chemotherapy in early NSCLC has proven feasible and safe in this large multicenter sample. Mature survival results of the NATCH trial are expected in")
91
LA SOPRAVVIVENZA A 5 ANNI DEL NSCLC STADIO I RESECATO E’ 23 / 30 Cross-tab label 1.80-90% 2.70-80% 3.60-70% 4.50-60%

92
LA SOPRAVVIVENZA A 5 ANNI DEL NSCLC STADIO II RESECATO è 22 / 30 Cross-tab label 1.75-85% 2.65-75% 3.55-65% 4.45-55%

93
NEL NSCLC LA CHEMIOTERAPIA ADIUVANTE E’ INDICATA 25 / 30 Cross-tab label 1.IN TUTTI I CASI OPERATI 2.SOLO IN STADI DI MALATTIA SPECIFICI 3.SOLO AL DI SOTTO DI 65 ANNI DI ETA’ 4.SOLO IN ASSOCIAZIONE ALLA RADIOTERAPIA

94
IL FARMACO CARDINE NEI REGIMI DI CHEMIOTERAPIA ADIUVANTE PER IL NSCLC E’ 23 / 30 Cross-tab label 1.Carboplatino 2.Cisplatino 3.Vinorelbina 4.Gemcitabina 5.Taxolo

95
LA CHEMIOTERAPIA NEO-ADIUVANTE NEL NSCLC E’ INDICATA 22 / 30 Cross-tab label 1.IN TUTTI I CASI POTENZIALMENTE OPERABILI 2.SOLO IN STADI DI MALATTIA SPECIFICI 3.SOLO AL DI SOTTO DI 65 ANNI DI ETA’ 4.NON E’ UNO STANDARD TERAPEUTICO

Similar presentations

 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")

 Baselga.>")



 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")



 - Surrogate end points - Quality of the performed.>")








