Download presentation
Presentation is loading. Please wait.

1
Role of MRI in TOF follow-up TOF symposium October 25, 2013 Dr Edythe Tham

2
Outline Quantification of RV size & function Quantification of pulmonary regurgitation Pulmonary stenosis Branch pulmonary arteries Conduits and artificial valves

3
Goals of cardiac MRI Quantification of RV & LV volumes and function (RVEF) Quantification of pulmonary regurgitant fraction (RF) Anatomy of the RVOT & branch pulmonary arteries (and aorta) Assessment of myocardial fibrosis
 Quantification of pulmonary regurgitant fraction (RF) Anatomy of the RVOT & branch pulmonary arteries (and aorta) Assessment of myocardial fibrosis")
4
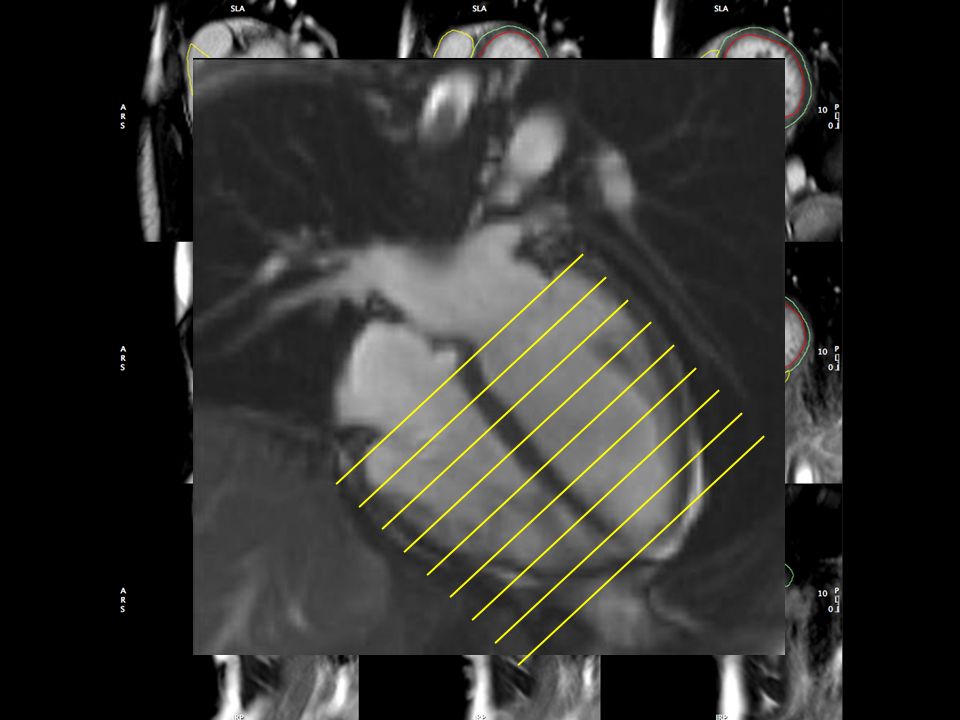
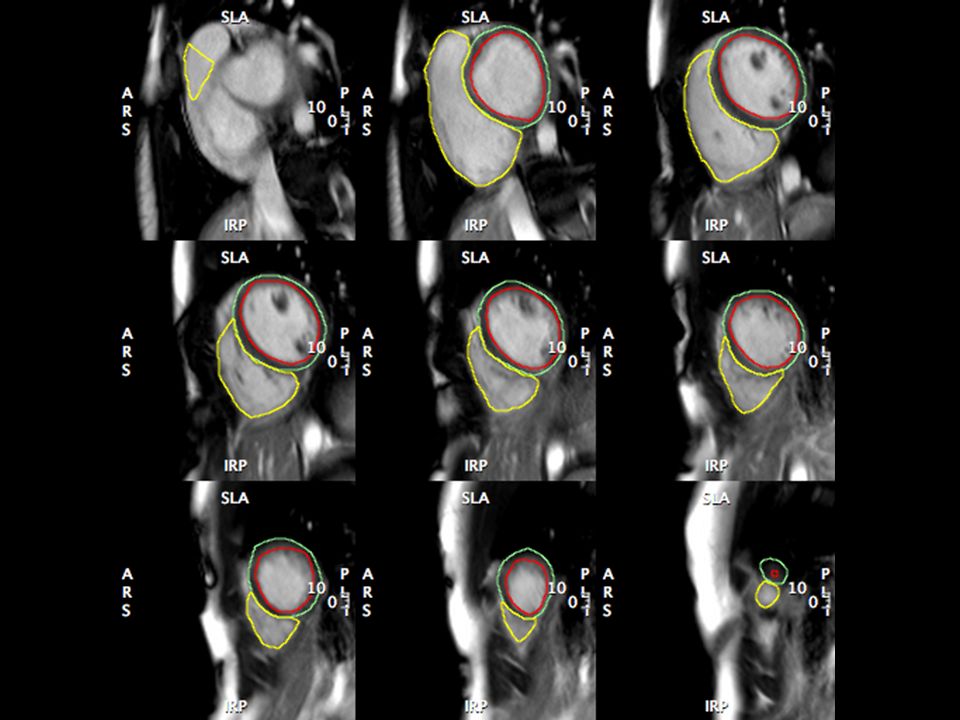
RV volumes

8
Pulmonary regurgitation Transannular patch

9
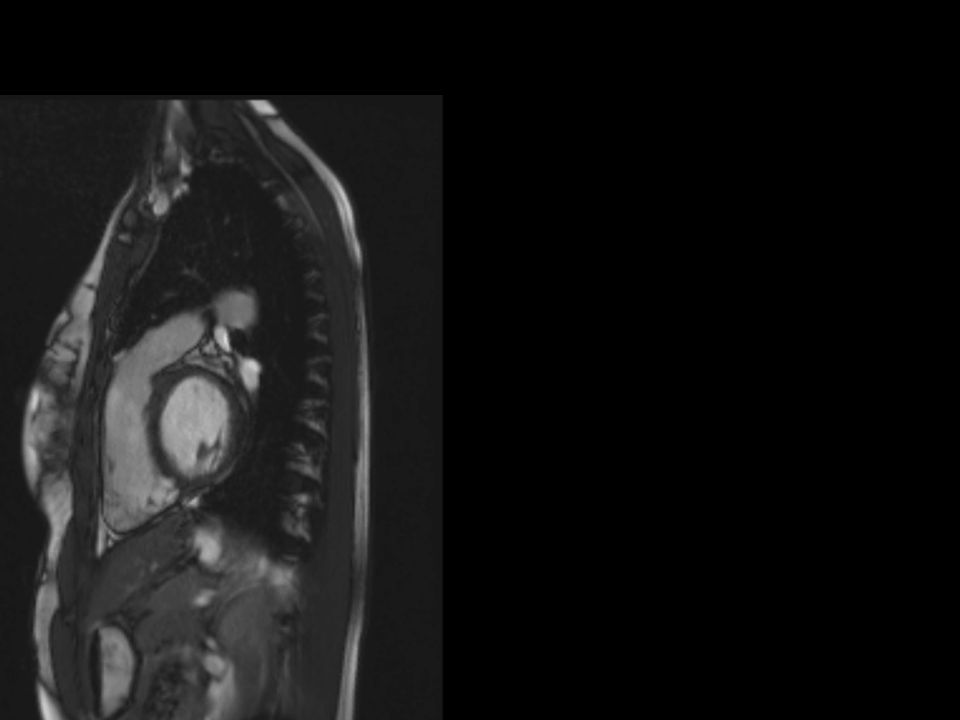
RVOT

10
Flow Quantification: Phase contrast imaging

11
Pulmonary Regurgitation Region of interest

12
Regurgitant fraction

13
Criteria for pulmonary valve replacement RVEDV >170 ml/m 2 RVESV > 85 ml/m 2 RVEF < 45% Regurgitant Fraction >30% Therrien et al, AJC 2005

14
Relationship between RV volume and pulmonary regurgitation Samyn et al, JMRI 2007

15
Relationship between RV ESV & RVEF Geva et al, JACC 2004

16
RVEDVi 111 ml/m2 RVESVi 56 ml/m2 RVEF 50% LVEF 60% 17 year female, S/P TAP

18
Regurgitant Fraction 43%

19
RVEDVi 178 ml/m2 RVESVi 150 ml/m2 RVEF 16% LVEF 28% 11 year female with TOF/PA S/P RV-PA conduit

20
Normal septal curvature TOF

21
Regurgitant fraction 57% Peak velocity 2 m/s = Peak gradient 16 mmHg

22
Pulmonary stenosis

24
10 year female S/P TAP Mixed disease – Mild PS: 20 mmHg Moderal PR: 34%

25
Magnetic Resonance Angiography Branch pulmonary arteries

28
21 year male S/P TOF repair RPA 56%: LPA 44% Mild proximal LPA stenosis, PG 25 mmHg

29
18 year old S/P TOF repair – bilateral branch PA stenosis RPA 75%: LPA 25% Peak gradients: RPA: 38 mmHg LPA: 29 mmHg

30
12 year female with branch PA stenosis From MRI RPA 82%: LPA 18%

31
Right pulmonary artery Left pulmonary artery

32
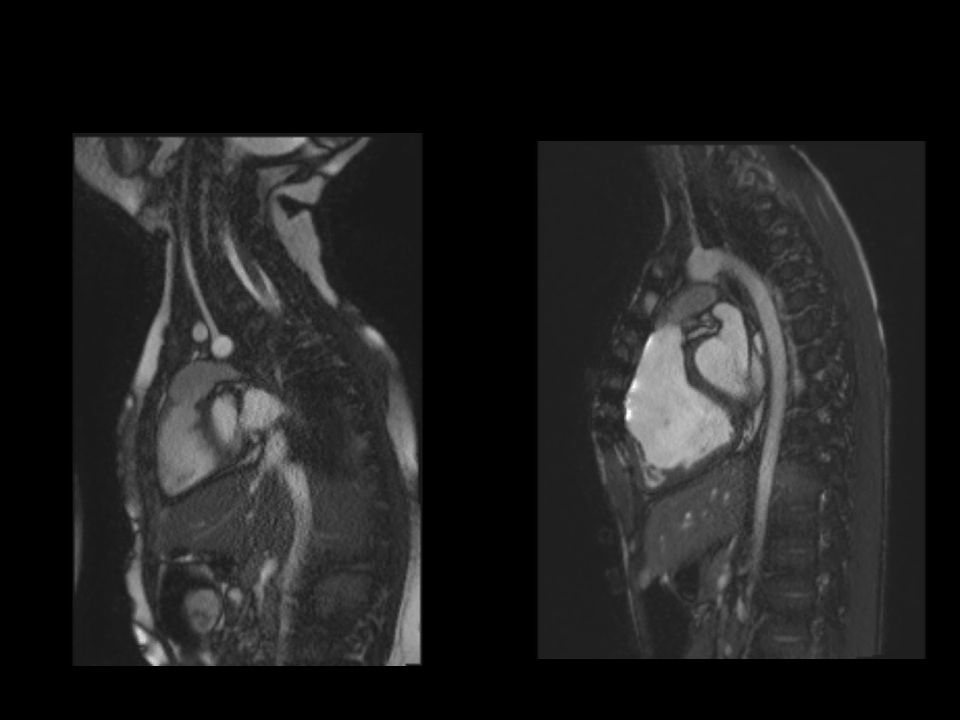
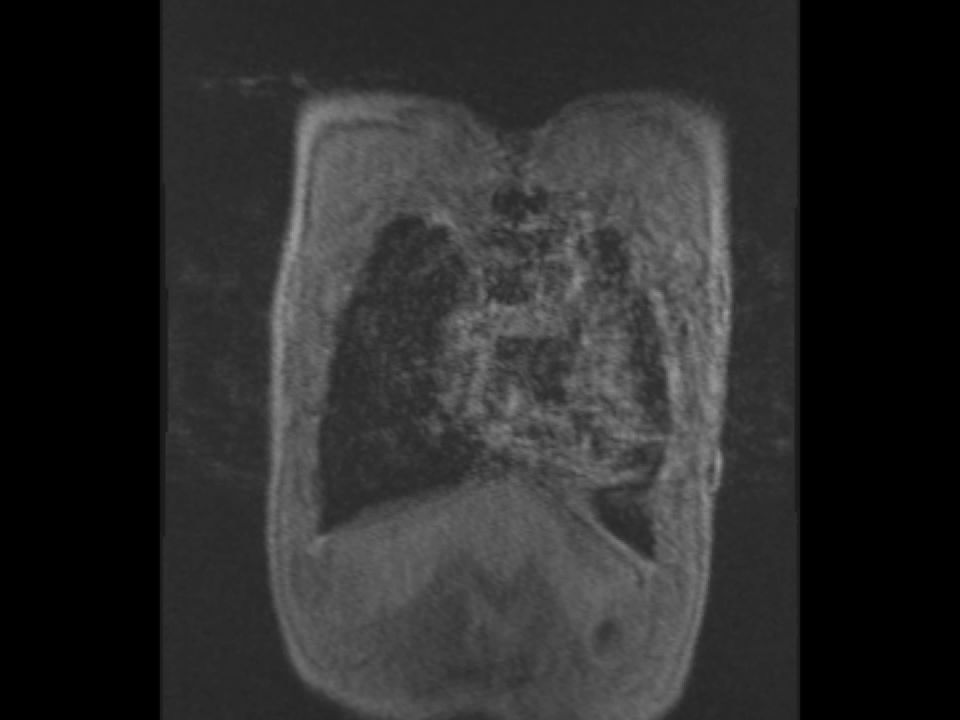
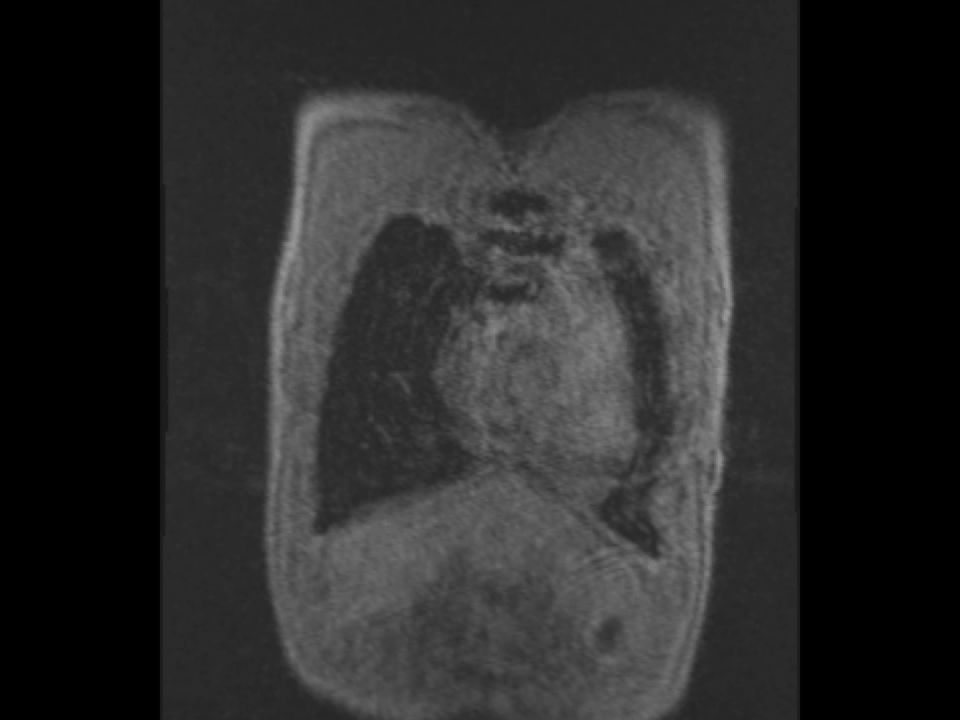
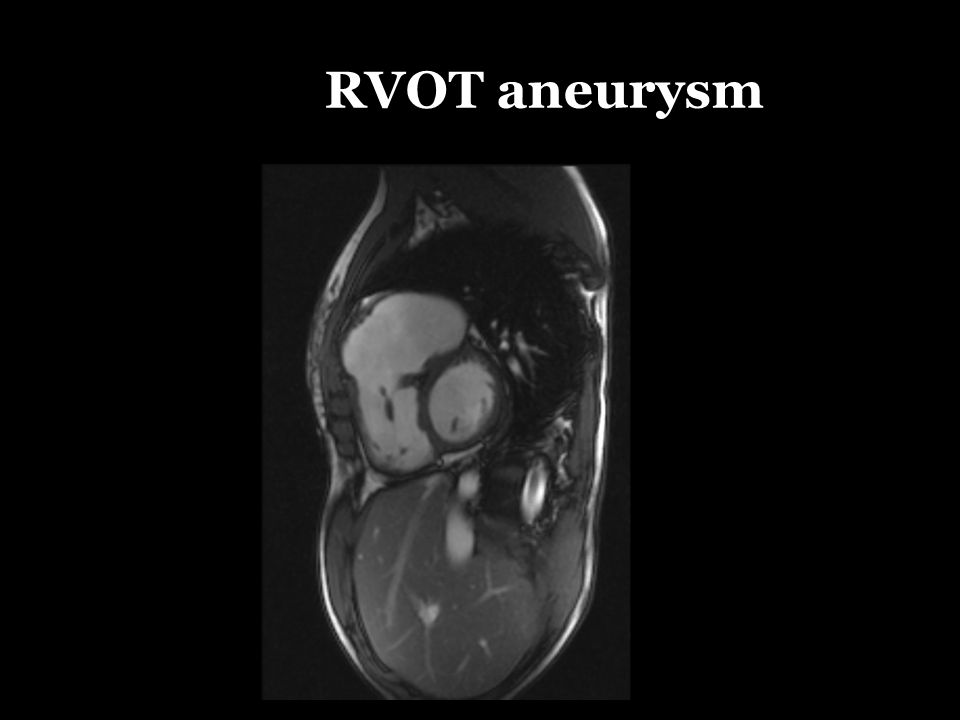
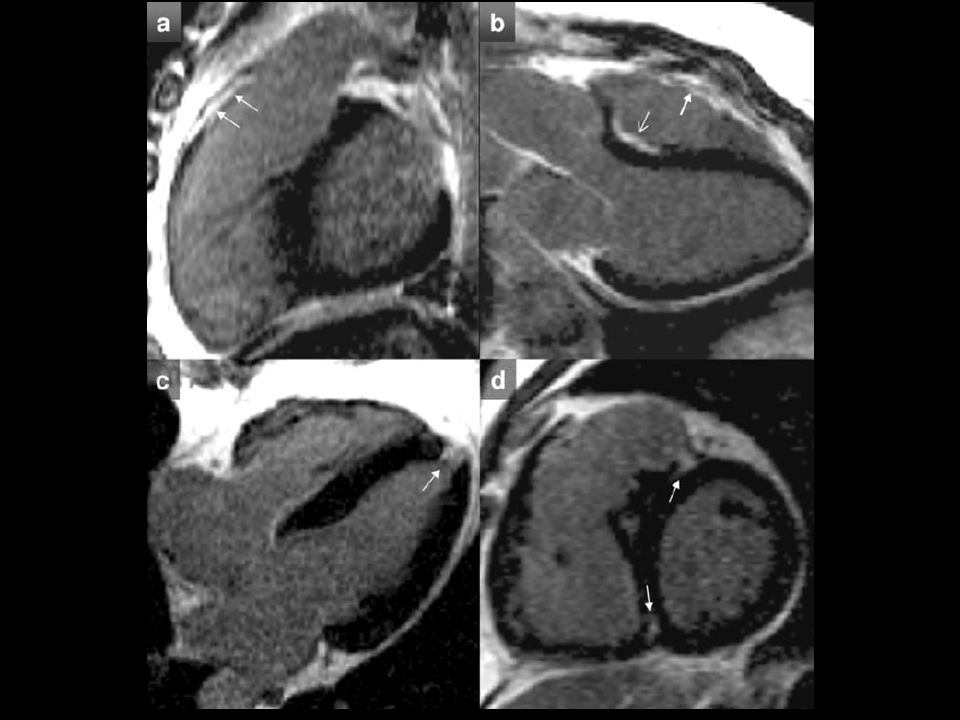
RVOT aneurysm

34
Conduits & artificial valves

35
Artifact from prosthetic valve 12 year female Prosthetic pulmonary valve Melody valve

42
38 year male S/P 29 mm Hancock valve RVEDVi 170 ml/m2 RVESVi 98 ml/m2 RVEF 42% RF 20% Peak velocity 3 m/s = PG 36 mmHg

43
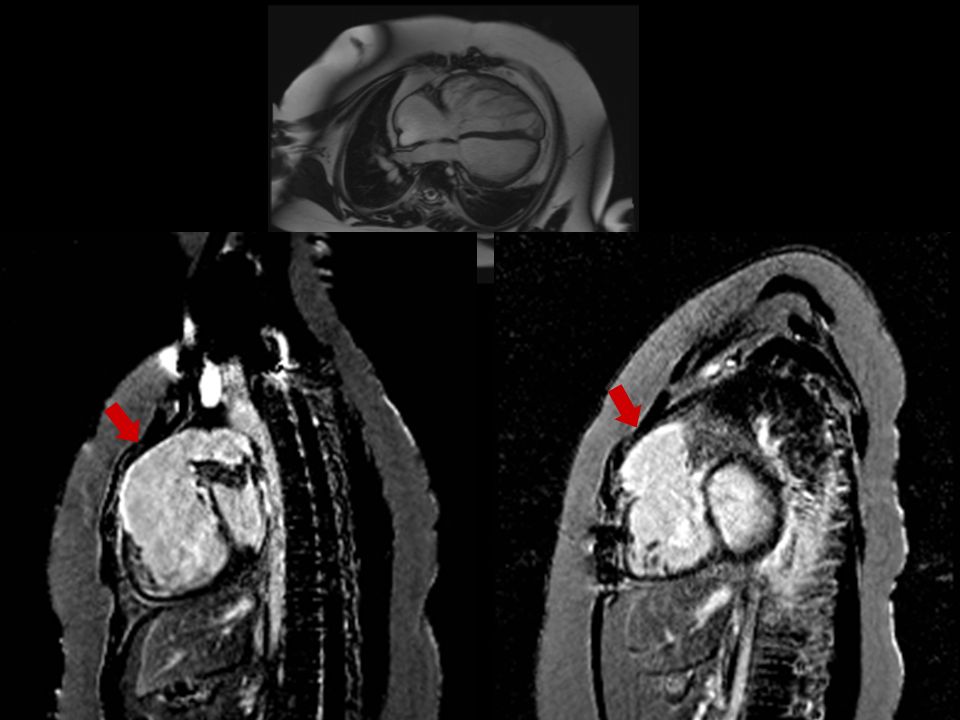
Melody valve

44
Circulation, 2006;113:405-413

47
RVEF 33%

48
Indications for cardiac MRI Baseline post-TOF repair at 7-10 years (no sedation required) Follow up every 1-3 years depending on clinical status Yearly MRI if: symptomatic or evidence of RV dysfunction
 Follow up every 1-3 years depending on clinical status Yearly MRI if: symptomatic or evidence of RV dysfunction")
49
Cardiac MRI: Disadvantages Not portable Contraindications: pacemaker/AICD Affected by metallic artifacts eg prosthetic valves, stents

50
Advantages of MRI No radiation Does not require sedation in older children Independent of acoustic windows Capability for 3D reconstruction Quantifies ventricular function Flow quantification

Similar presentations
















>")


