Download presentation
Presentation is loading. Please wait.

1
Infarction Yiran Ni M.D Department of pathology CTGU Mail: 401761415@qq.com Tel: 15997529140 Office room: S-2623

2
Water Blood Trunk Vessel Leaves fall Tissue necrosis Question 1 What is infarction?

4
Definition An infarct is an area of ischemic necrosis caused by occlusion of either the arterial supply or the venous drainage in a particular tissue.

5
Common sites Infarction involving different organs is a common and extremely important cause of clinical illness. Myocardia infarction causes 17 million death world-wide annually(1million in China). Cerebral infarction causes 5 million death world-wide annually (1.5million in China).
. Cerebral infarction causes 5 million death world-wide annually (1.5million in China)..")
6
Pulmonary infarction Bowel infarction Ischemic necrosis of the extremities (gangrene)
")
7
Question 2: What are the common causes of infarction?

8
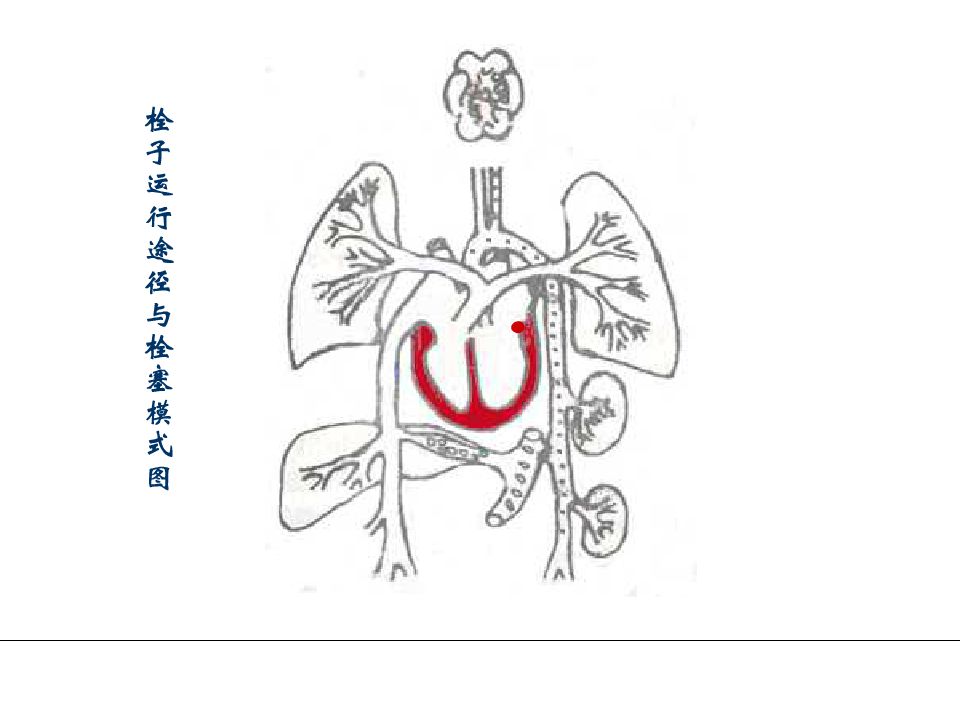
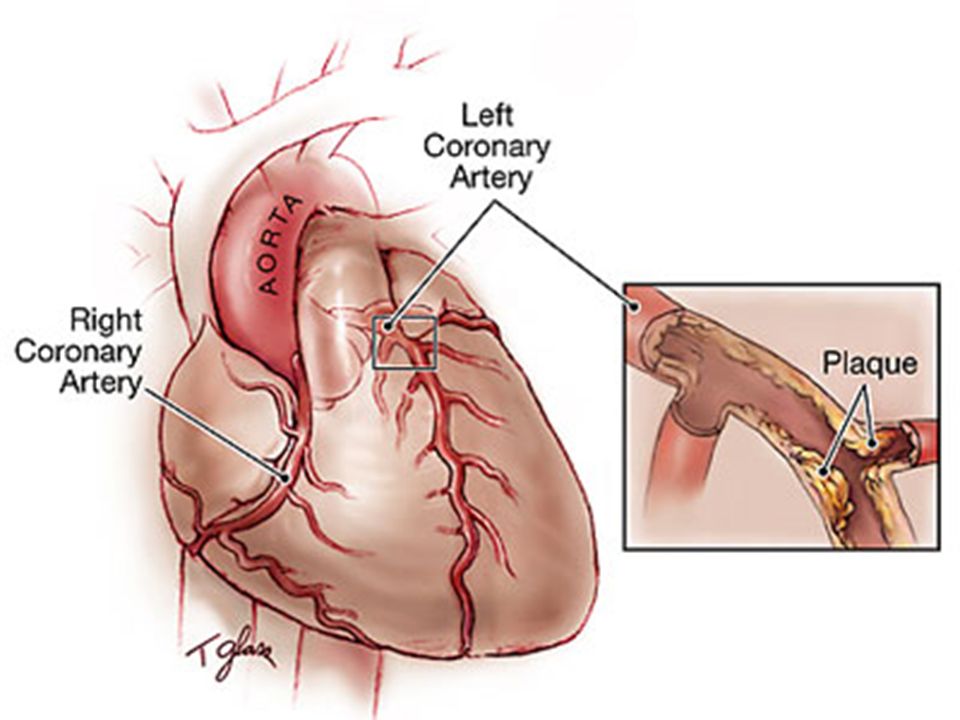
Common causes Commonest cause: thrombotic or embolic events lead to arterial occlusion.

16
Expansion of an atheroma secondary to intraplaque hemorrhage Extrinsic compression of a vessel (e.g., by tumor). Local vasospasm Vessel twisting (e.g., in testicular torsion or bowel volvulus). Vascular compression by edema or entrapment in a hernia sac. Traumatic vessel rupture. venous obstruction(e.g., testis and ovary).
. Vascular compression by edema or entrapment in a hernia sac. Traumatic vessel rupture. venous obstruction(e.g., testis and ovary)..")
17
Question 3: What are factors that influence development of an infarct ?

18
Factors that influence development of an infarct The major determinants include: (1) the nature of the vascular supply; (2) the rate of development of the occlusion; (3) the vulnerability of a given tissue to hypoxia; (4) the blood oxygen content.
 the nature of the vascular supply; (2) the rate of development of the occlusion; (3) the vulnerability of a given tissue to hypoxia; (4) the blood oxygen content.")
19
(1)The nature of the vascular supply The availability of an alternative blood supply is the most important factor in determining whether occlusion of a vessel will cause damage.
The nature of the vascular supply The availability of an alternative blood supply is the most important factor in determining whether occlusion of a vessel will cause damage.")
20
Capillary network bronchia PA BA PV BV The changes of the blood circulation when embolism of pulmonary arteries occur

23
(2)The rate of development of the occlusion Slowly developing occlusions are less likely to cause infarction because they provide time for the development of alternative perfusion pathways.
The rate of development of the occlusion Slowly developing occlusions are less likely to cause infarction because they provide time for the development of alternative perfusion pathways.")
25
(3)The vulnerability of a given tissue to hypoxia The susceptibility of a tissue to hypoxia influences the likelihood of infarction. Neurons undergo irreversible damage when deprived of their blood supply for only 3 to 4 minutes.

27
(4)The blood oxygen content The partial pressure of oxygen in blood also determines the outcome of vascular occlusion. Partial flow obstruction of a small vessel in an anemic or cyanotic patient might lead to tissue infarction, whereas it would be without effect under conditions of normal oxygen tension. In this way, congestive heart failure, with compromised flow and ventilation, could cause infarction in the setting of an otherwise inconsequential blockage.

28
Question 4: What are the typical morphologic changes of an infarct ?

29
Morphology of infarcts (1 ) Shapes : depends on vascular distribution of the organ pyramid shaped infarct: kidney, lungs, and spleen irregular, map shaped infarct: heart, brain
 Shapes : depends on vascular distribution of the organ pyramid shaped infarct: kidney, lungs, and spleen irregular, map shaped infarct: heart, brain")
30
pyramid shaped infarct: kidney, lungs, and spleen

31
Irregular, map shaped infarct: heart, brain

32
(2) Texture : depends on pathological changes in different organs Coagulative necrosis – solid organs (kidenys, spleen), lungs and intestine etc Liquefactive necrosis – brain(cerebral malacia)-cyst formation
 Texture : depends on pathological changes in different organs Coagulative necrosis – solid organs (kidenys, spleen), lungs and intestine etc Liquefactive necrosis – brain(cerebral malacia)-cyst formation")
33
(3)Color of an infarct Infarcts are classified on the basis of their color (reflecting the amount of hemorrhage). Therefore, infarcts may be either red (hemorrhagic) or white (anemic).
 or white (anemic)..")
34
Anemic infarcts (White infarcts) Anemic infarcts (White infarcts) White (anemic) infarcts occur with arterial occlusions in solid organs with end-arterial circulation (such as heart, spleen, and kidney), where the solidity of the tissue limits the amount of hemorrhage that can seep into the area of ischemic necrosis from adjoining capillary beds.
 Anemic infarcts (White infarcts) White (anemic) infarcts occur with arterial occlusions in solid organs with end-arterial circulation (such as heart, spleen, and kidney), where the solidity of the tissue limits the amount of hemorrhage that can seep into the area of ischemic necrosis from adjoining capillary beds.")
35
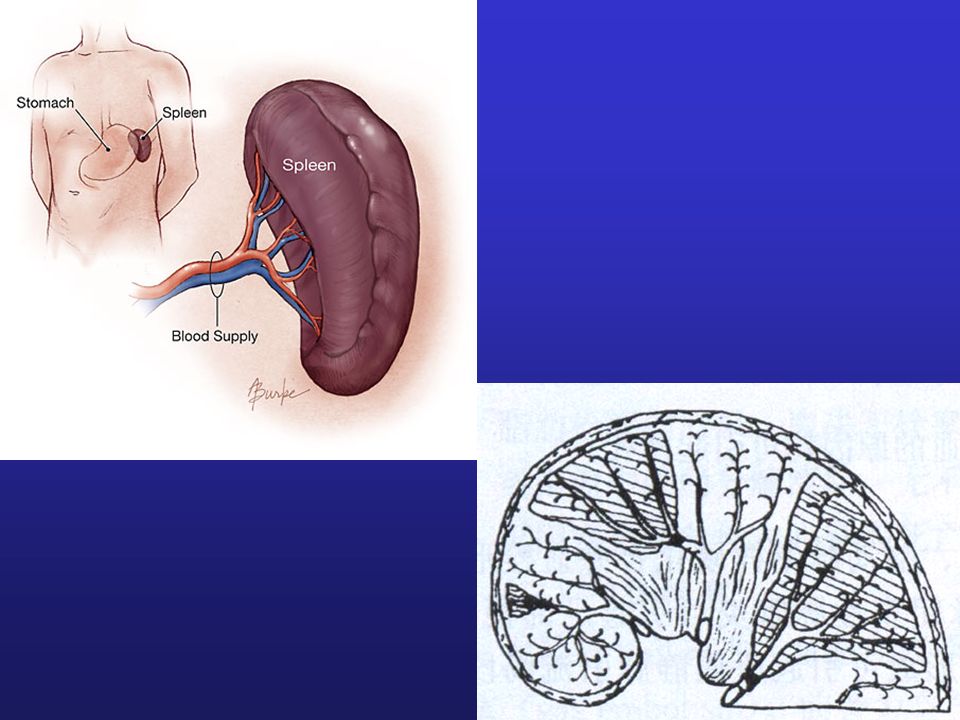
Morphology of anemic infarcts (White infarcts) Organ involved: solid organs with deficient collateral circulation of arteries (heart, kidneys, spleen, etc.) Grossly: wedge-like or triangular necrotic foci with peripheral hemorrhagic zone
 Organ involved: solid organs with deficient collateral circulation of arteries (heart, kidneys, spleen, etc.) Grossly: wedge-like or triangular necrotic foci with peripheral hemorrhagic zone")
36
Anemic infarcts of spleen

37
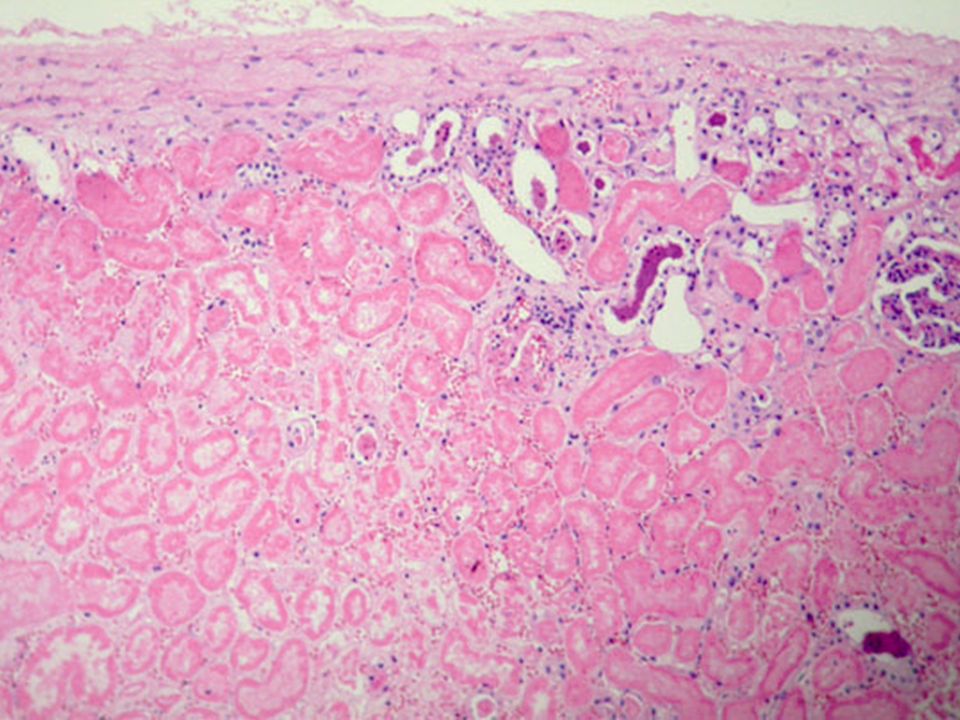
Anemic infarcts of kidney

38
Anemic infarcts of heart

39
Microscopically: ischemic coagulative necrosis The outline of tissue structure remains Nuclear changes: pyknosis, karyorrhesix, or karyolysis Leucocytic reaction at peripheral margin

40
Anemic infarcts of heart muscle

41
Anemic infarcts of kidney

43
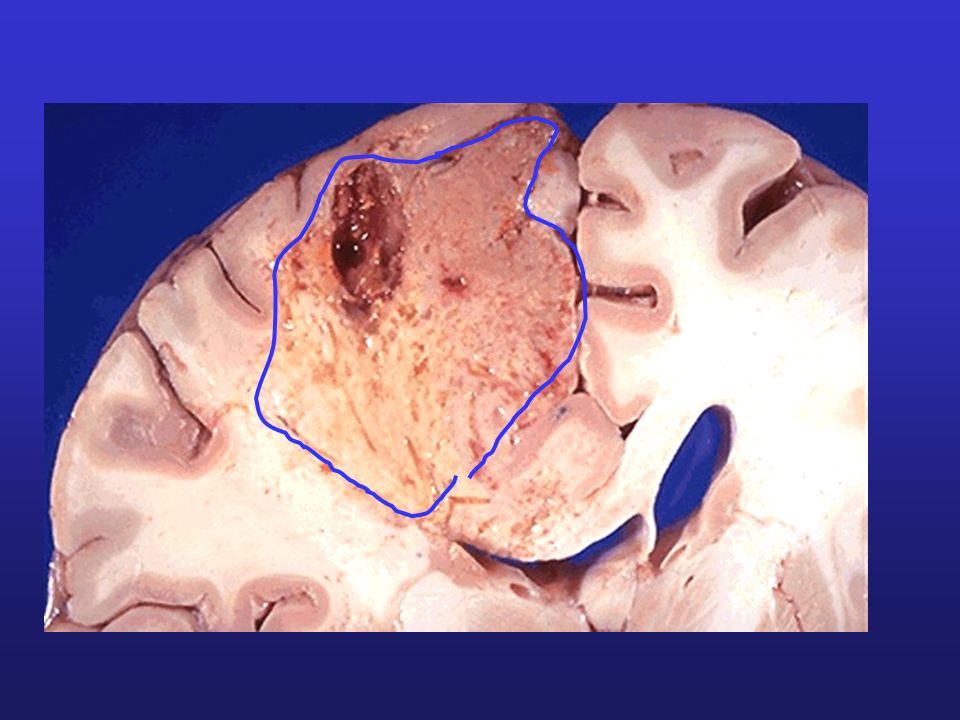
Anemic infarcts of brain Irregular shaped Liquefactive necrosis -cerebral malacia -cyst formation

47
Hemorrhagic infarcts (Red infarcts) Hemorrhagic infarcts (Red infarcts) Red (hemorrhagic) infarcts occur (1) with venous occlusions
 Hemorrhagic infarcts (Red infarcts) Red (hemorrhagic) infarcts occur (1) with venous occlusions")
48
(2) in loose tissues (such as lung), which allow blood to collect in the infarcted zone
 in loose tissues (such as lung), which allow blood to collect in the infarcted zone")
49
(3) in tissues with dual circulations (e.g., lung and small intestine), permitting flow of blood from the unobstructed vessel into the necrotic zone (obviously such perfusion is not sufficient to rescue the ischemic tissues);
 in tissues with dual circulations (e.g., lung and small intestine), permitting flow of blood from the unobstructed vessel into the necrotic zone (obviously such perfusion is not sufficient to rescue the ischemic tissues);")
50
(4) in tissues that were previously congested because of sluggish venous outflow;
 in tissues that were previously congested because of sluggish venous outflow;")
51
(5) when flow is re-established to a site of previous arterial occlusion and necrosis
 when flow is re-established to a site of previous arterial occlusion and necrosis")
52
Question 5:The fate of an infarct

53
Key points 1. Definiton 2. Causes 3. Determinants 4. Morphology

Similar presentations















, fibrous material and.>")









>")




