Download presentation
Presentation is loading. Please wait.

1
Hospitalizations and the Patient Discharge: Has Society Overlooked Quality in Favor of Efficiency? (and what if anything can we, as individuals do about it?) Eric E. Howell, M.D. Associate Professor of Medicine Johns Hopkins University, School of Medicine Johns Hopkins Bayview Medical Center
 Eric E. Howell, M.D. Associate Professor of Medicine Johns Hopkins University, School of Medicine Johns Hopkins Bayview Medical Center.")
2
Disclosures Co-Investigator of BOOST (better outcomes for older adults through safe transitions) an SHM/Hartford foundation funded project Lecture on transitions of care No off label medication discussions No device discussions
 an SHM/Hartford foundation funded project Lecture on transitions of care No off label medication discussions No device discussions")
3
Objectives Review national LOS and readmissions data Review data on the hospital discharge process Provide an overview of studies that Improved DC efficiency Improved DC quality Provide examples of resources available

4
Background: It was 1983 The DRG payment system instituted Goals: Reduced LOS Increase efficiency Reduce cost Some concern about quality (readmissions) Little done to monitor Until recently, not studied
 Little done to monitor Until recently, not studied")
5
Background: 2009 Health care reform front & center Goals: Increase efficiency Reduce cost Improve quality

6
DeFrances et al, Adv data, 2007 Jul 12;(385):1-19 Average LOS: US Hospitals 1970-2005 >65 yo: 12.6 to 5.5 days
:1-19 Average LOS: US Hospitals >65 yo: 12.6 to 5.5 days")
7
Lower LOS Value The Commonwealth Fund, 2006

8
Hospitalists $50 more per DC Much of cost due to readmission Also more NH discharges And more ED visits

9
Jencks S, Williams MV, Coleman EA. N Engl J Med 2009;360:1418-1428 Rates of Rehospitalization within 30 Days after Hospital Discharge

10
20% rehospitalization rate @ 30 days $17Billion in costs Wide variability in rehospitalization by state (13-23%)
")
11
What is the relationship between LOS and hospital readmissions?

12
90 Day Readmission Rate (%) Elderly Pts with CHF Rich, et al. Am J Public Health. 1988 June; 78(6): 680–682. CONCLUSION in 1988: “shorter hospital stays under the DRG system are not necessarily associated with a rebound increase in readmission frequency”
: 680–682. CONCLUSION in 1988: shorter hospital stays under the DRG system are not necessarily associated with a rebound increase in readmission frequency .")
13
90 Day Readmission Rate (%) 20th vs 21 st Century
 20th vs 21 st Century")
14
Medicare 60 Day Readmission Rates Jencks et al, N Engl J Med 2009 Discussion: “…difference is more likely to indicate an actual increase in rehospitalization rates over time, perhaps owing to a shorter duration of index hospitalization…”

15
LOS & Readmission 59 hospitals, >100,000 pts Hospitals with shorter LOS found to be at risk for increased readmissions Better staffing ratios mitigated risk somewhat Norwegian study Health Serv Res. 2002;37:647-665

16
LOS & Readmission 1913 patients, single Academic Medical Center 31% of readmitted pts had “too short hospital stay” Sicker patients had same LOS as all pts 50% of reahospitalized patients had LOS < 2 days Done in Israel Medicine. 2008 Sep;87(5):294-300.
:")
17
I Love Lucy

18
Length Of Stay Readmission Rate How to go from this…. You are here

19
Length Of Stay Readmission Rate …to this You are here

20
Re-engineer the “J-curve” Appropriately focus on LOS & keep short! Follow rehospitalization rate “engineer” systems to improve quality of DC process Align reimbursement to focus on quality & efficiency

21
Efficiency Quality Current reward systemIdeal Reward system

22
Hospital Discharge “Random events connected to highly variable actions with only a remote possibility of meeting implied expectations.” © 2006 Institute for Healthcare Improvement “Steal shamelessly, share senselessly”

23
A lot of Evidence Emerging that DC Process is Broken

24
Discharge Communication Poor Hospitalist-PCP communication documented 3-20% of time Phone notification of D/C 31% of time Less than 1/3 of PCPs do not receive D/C summary by f/u appointment! Hruby, how do patients view the role of the primary care physician in inpatient care? Pantilat, primary care physician attitudes regarding communication with hospitalists Van Walraven, dissemination of discharge summaries. Not reaching follow-up physicians (Can Fam Physician. 2002 Apr;48:737-42.) Kripalani, Deficits in communication and information transfer between hospital-based and primary care physicians, JAMA 2007 Feb 28;297(8):831-41
 Kripalani, Deficits in communication and information transfer between hospital-based and primary care physicians, JAMA 2007 Feb 28;297(8):")
25
Discharge Summary Quality Poor No diagnostic test results (33-63%) No hospital course/treatment (7-22%) No discharge meds (2-40%) Pending tests not listed (65%) Lack of follow-up plan listed (2-43%) Kripalani, JAMA 2007 Feb 28;297(8):831-41
 No hospital course/treatment (7-22%) No discharge meds (2-40%) Pending tests not listed (65%) Lack of follow-up plan listed (2-43%) Kripalani, JAMA 2007 Feb 28;297(8):831-41")
26
The Dangers of DC 41% of patients discharged with pending test results 9.4% could require action Of the 9.4% 37.1% “actionable”- change in plan of car needed 12.6% “urgent” - action required MDs unaware 61% of time Roy, 2005;143(2):121-128
:")
27
The Dangers of DC ¼ of discharged patients require outpatient workup More than one third not done (35.9%) Discharge summaries improved work up rate Increased time from D/C to F/U appointment decrease work up rate Moore, arch int med, 2007;167:1305-1311
 Discharge summaries improved work up rate Increased time from D/C to F/U appointment decrease work up rate Moore, arch int med, 2007;167:")
28
The Dangers of DC 1 in 5 (23%) discharges with adverse event 72% of adverse events due to medications 16% due to “therapeutic errors” Half of events for preventable or ameliorable Forster, (CMAJ 2004;170(3):345-9
 discharges with adverse event 72% of adverse events due to medications 16% due to therapeutic errors Half of events for preventable or ameliorable Forster, (CMAJ 2004;170(3):345-9")
29
Better Efficiency Does not Always = Reduced Quality Tufts Hospitalist managed pts for 6 weeks LOS Reduced from 3.45 to 2.19 266 increased admissions annually Cost reduced from $2,332 to $1,775 No change in readmission Health Serv Res. 2003 Jun;38(3):905-18
:")
30
Better Efficiency Does not Always = Reduced Quality Urban community teaching hospital 5308 patients cared for by hospitalists LOS shorter by 0.61 days Cost lower ($822) Lower mortality rate in hospital & at 30 & 60 days Readmission rate similar at 10 days Ann Intern Med. 2002 Dec 3;137(11):859-65
:")
31
Better Efficiency Does not Always = Reduced Quality Review of hospitalist studies 1996-2001 JAMA. 2002;287(4):487-94 …hospitalists improve inpatient efficiency without harmful effects on quality…
: …hospitalists improve inpatient efficiency without harmful effects on quality….")
32
Multiple Studies Show Discharge Quality can be Improved

33
30,000 Patients 2003-2006 Readmission rate 23.3% for “low follow up” (<~33%) 20.5% for “higher follow up” rate (>~33%) May 2010
 20.5% for higher follow up rate (>~33%) May 2010")
34
RCT of 749 hospitalized adults Nurse Discharge Advocate F/U appt, Medication Reconciliation Patient education Individualized instruction booklet Pharmacist call 2-4 days post-discharge Review medications Jack, B. W. et. al. Ann Intern Med 2009;150:178-187

35
Project RED Outcomes Intervention (n = 370) Control (n = 368) ER Visits* 16.5%24.5% Rehospitalization** 15%21% PCP f/u in 30 days* 62%44% Prepared for Discharge* 65%55% *p < 0.05 **p = 0.09
 Control (n = 368) ER Visits* 16.5%24.5% Rehospitalization** 15%21% PCP f/u in 30 days* 62%44% Prepared for Discharge* 65%55% *p < 0.05 **p = 0.09")
36
Coleman’s Transition Coach Eric Coleman and others (n=750): “Transition coach” Hospital Home Phone Empowerment Self management Patient owned health record Timely follow-up A list of “red flags” and what to do Coleman, Arch Int Med. 2006;166:1822-1828

37
Coleman’s Transition Coach Eric Coleman and others (n=750): Reduced readmissions 30 days 90 days Reduced readmission for same dx 90 days 180 days Reduced Cost ~ $300k a year Adopted by over 135 leading health care organizations nationwide Coleman, Arch Int Med. 2006;166:1822-1828

38
237 elderly patients at 3 hospitals Academic, community 5 component intervention Admission form with geriatric cues Fax to PCP Interdisciplinary worksheet Pharmacist-Physician Med Rec Pre-Discharge Planning Appointments J Am Geriatr Soc. 2009 Aug 18

39
Safe STEP Data Pre-InterventionIntervention Colman CTM > 7268%89% ED Visit 3 days10%3% ED Visit 30 days21%14% Readmission22%14% Feel Better71%84%

40
Post discharge - follow-up by RN or MD Naylor et al: RN visit post d/c for geriatric medical patients decreased rehospitalizations 10% vs. 23% (p = 0.04) @ 6 wks N/S by 12 weeks Anderson et al: MD visit post d/c for stroke decreased rehospitalizations 26% vs. 44% @ 6 months Ann Intern Med 1994;120(12):999-1006. Stroke 2000;31:1038-48.
: Stroke 2000;31:")
41
Pharmacists & Transitions of Care Pharmacist medication reconciliation Counseling at DC and 3 day f/u Helpful with adverse drug events (ADEs) Decreased preventable medication ED visits No difference in total ADEs, health care utilization, pt satisfaction, med compliance Schnipper, Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006 Mar 13;166(5):565-71
:")
42
Pharmacists & Transitions of Care Pharmacist post discharge phone call Higher patient satisfaction 19% pts had medication problems resolved 15% of pts had new problems identified Lower 30 day ED visits Trend towards lower re-admission rate Dudas, The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001 Dec 21;111(9B):26S-30S
:26S-30S.")
43
Pharmacists & Transitions of Care HOMER trial- home visits by pharmacists 2 & 8 weeks post DC Higher hospital readmission rate No improvement in QOL or death Holland, Does home based medication review keep older people out of hospital? The HOMER randomised controlled trial. BMJ. 2005 Feb 5;330(7486):293
:293.")
44
Your participation can transform… …This……into This!!

45
Tools for Improving the Discharge Process

46
NQF Safe Discharge Practice (project RED)
")
47
National Transitions of Care Coalition (NTOCC)
")
48
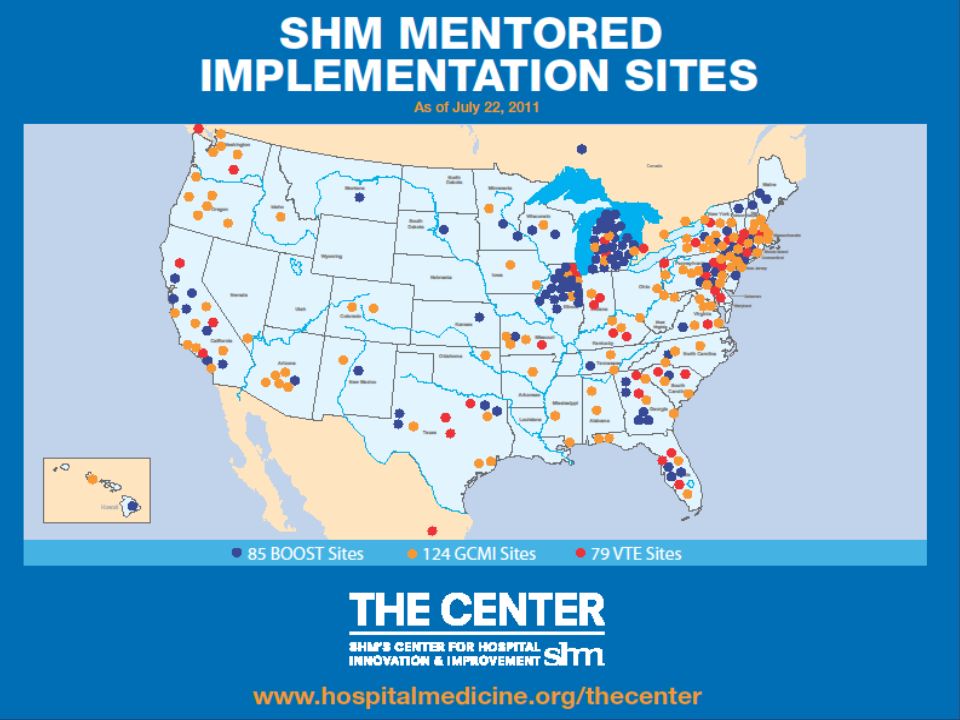
Initial BOOST Hartford Foundation-SHM Collaborative 30 hospitals Web resources Resource guide Interdisciplinary Teaches QI Leadership info Sample letters to hospital leaders http://www.hospitalmedicine.org/BOOST

50
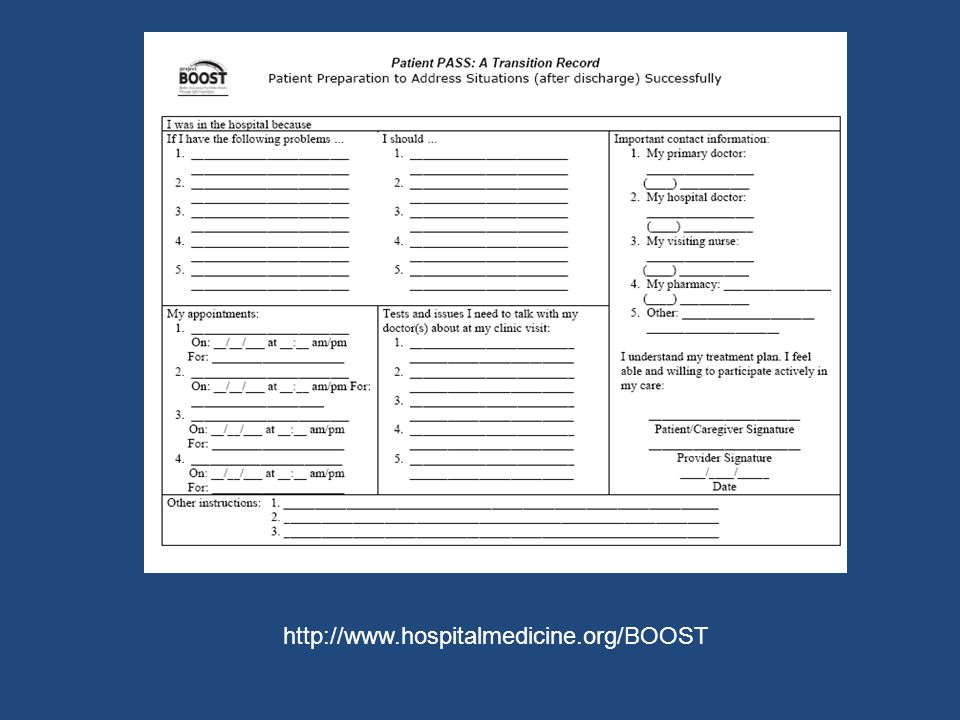
BOOST Hartford Foundation-SHM Collaborative Dedicated mentors Meet with hospital Call at min 1, 3, 6, 9 months Site visit Implementation toolkit Risk assessment (TARGET) Patient friendly DC (PASS, GAP) http://www.hospitalmedicine.org/BOOST
 Patient friendly DC (PASS, GAP)")
52
Web Resources

53
http://www.hospitalmedicine.org/BOOST
54
Summary The discharge process is broken Current system outdated Readmission rates high: 1 in 5 patients return Incentives focus only on LOS (for now) There is associated cost ($17B)
 There is associated cost ($17B)")
55
Summary Possible to improve the DC process Project Red Safe STEP Coleman’s Care Transition Coach Improvement projects (BOOST) available Readmission reduction by 1/3 could save billions and is feasible
 available Readmission reduction by 1/3 could save billions and is feasible")
56
Eric E. Howell M.D. ehowell@jhmi.edu

Similar presentations




 A Community Collaboration.>")
 A Community Collaboration.>")













 Supporting Patients and Practitioners in Optimizing Health.>")