Download presentation
Presentation is loading. Please wait.

1
Kristi McIntyre M.D. Resident’s lecture
Breast Cancer Kristi McIntyre M.D. Resident’s lecture

2
Breast cancer Risk factors Hereditary breast cancer Detection Staging
Surgical intervention Prognostic factors Management of early stage breast cancer

3
Breast cancer risk factors
Age/race Reproductive issues/Estrogen-related factors Breast histology Life style factors Family history/Genetic factors

4
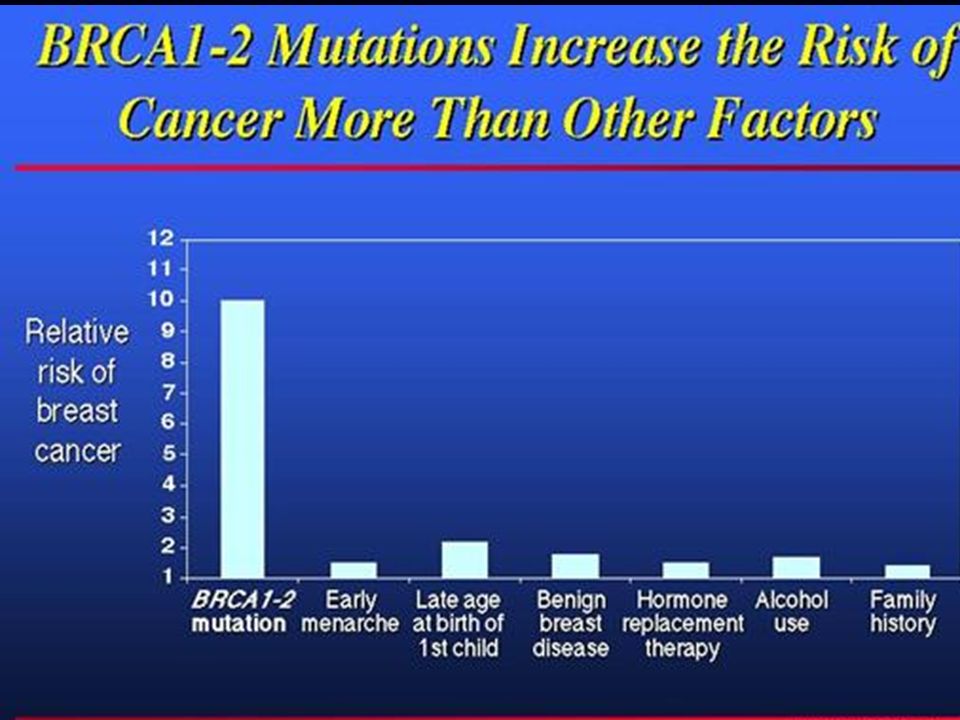
Breast Cancer Risk Factors

5
Breast Cancer Incidence

6
Race/Ethnicity and Breast Cancer Risk
Annual incidence Caucasian African Americans Hispanic Asian American Indian SEER results: age adjusted only Jemal CA:Cancer J.Clin ;2003,53:5

7
Race/Ethnicity and Breast Cancer Risk
“Adjusted Hazard Ratios” 0.4 0.6 0.8 1.0 1.2 African American .72 Hispanics American Indian Asian Only African Americans had lower breast cancer risk (p=o.oo6) than Caucasians Cheblowski JNCI ;March 2005
 than Caucasians. Cheblowski JNCI ;March")
8
Race/Ethnicity and Breast Cancer Risk
Combined Grade III and ER negative by race Cheblowski JNCI ;March 2005

9
Race/Ethnicity and Breast Cancer Risk
Differences in breast cancer incidence rates between most ethnic groups can largely be explained by control of risk factors African American women are at significantly reduced risk African American women have a higher proportion of unfavorable features suggesting cause for higher mortality rates Cheblowski JNCI ;March 2005

10
Reproductive Factors and Breast Cancer
Menarche < 16 Menopause >50 Menarche < OR 1.2 Menopause > OR 1.5 Null parity OR 2.0 Breastfeeding 4.3% decrease risk/yr First live birth< OR 0.5 First live birth > OR 1.5

11
WHI Trial of Estrogen plus Progestin
E+P placebo p-value Invasive Breast cancers SEER high stage % % Abnormal Mammograms More breast cancers diagnosed at more advanced stage and increased abnormal mammograms More breast cancers diagnosed at more advanced stage and increased abnormal mammograms Chlebowski JAMA 2003;

12
Breast histology and breast cancer risk
Benign breast disease RR Fibrocystic disease Atypical ductal hyperplasia Atypical ductal hyperplasia and family history

13
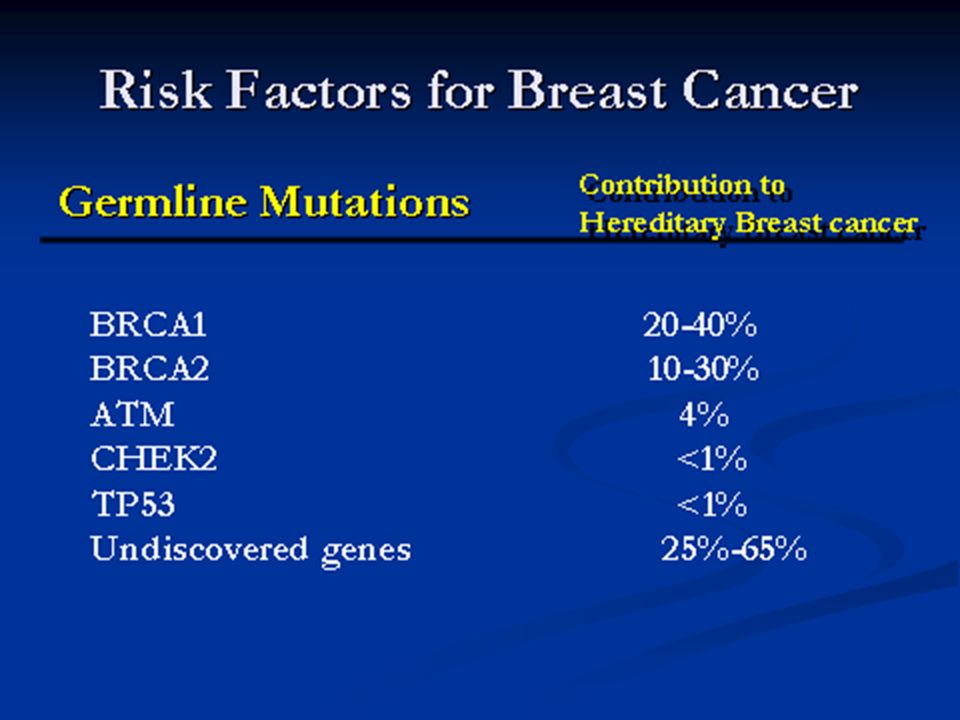
Risk Factors for Breast Cancer
Family History Risk First Degree relative Premenopausal diagnosis Bilateral disease Premenopausal diagnosis and bilateral disease Postmenopausal diagnosis Second Degree relative Premenopausal diagnosis Postmenopausal diagnosis

14
Hereditary

15
Family history and breast cancer risk
Most hereditary breast cancers arise from mutations in BRCA1 and BRCA2 Autosomal dominant , tumor suppressor gene

19
BRCA mutations and lifetime cancer risk
50-85% breast cancer 50% Second breast cancers 15-45% ovarian cancer risk Other malignancies: prostrate pancreatic male breast cancer

20
Founder mutations and Breast cancer
Ethnic background should be considered in risk assessment for breast cancer “ Founder” gene mutations discovered in individuals of Ashkenazi Jewish descent 50-90 % have gene susceptibility with positive family history Founder mutations have been found in populations of Iceland,Finland, France, Holland , Russia,and Sweden

21
Models for risk assessment
Gail model Claus model Age Age first live birth Age first menses FH-maternal only; no age # prior breast biopsies/ADH race Family history Age at diagnosis Both models inadequate : not useful for mutation carriers or individual risk www3.utsouthwestern.edu/cancergene/

22
Lifestyle factors and breast cancer risk
Body mass index: postmenopausal women >30% excess BMI increased risk Dietary fat intake: increased risk NSAID use: decreases risk Physical activity: 1.25 to 2.5/hrs week brisk walking had 18 % decrease risk Smoking : increased risk Alcohol use: increased (dose dependent)
")
23
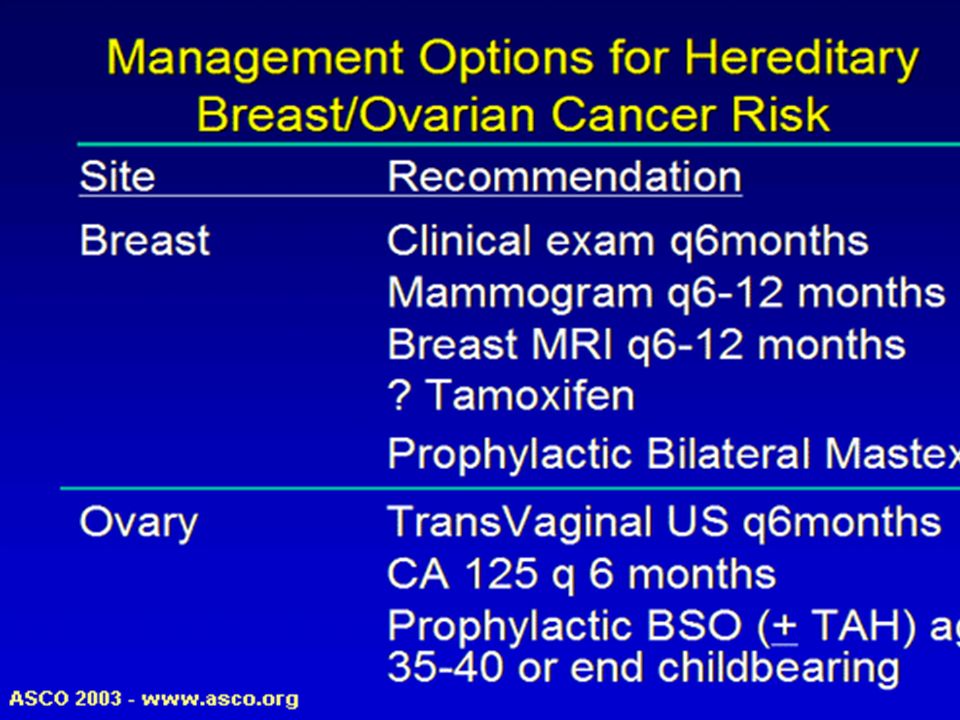
Risk Reduction Strategies
Average Risk Moderate Risk Early childbirth Exercise Maintain normal weight Avoid smoking/alcohol Avoid prolonged HRT Chemoprevention

28
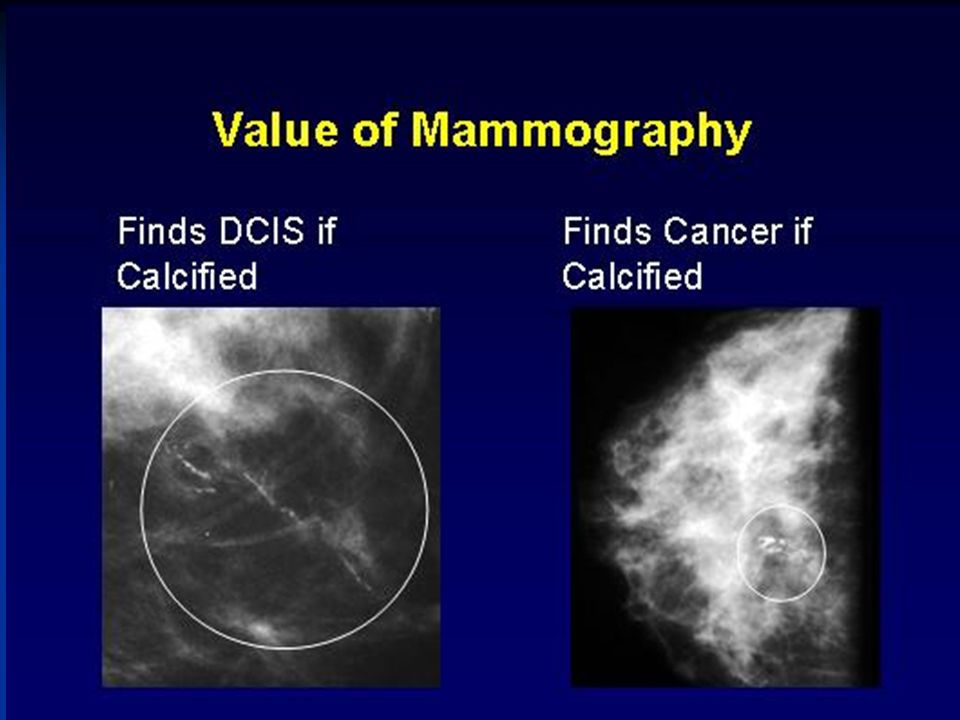
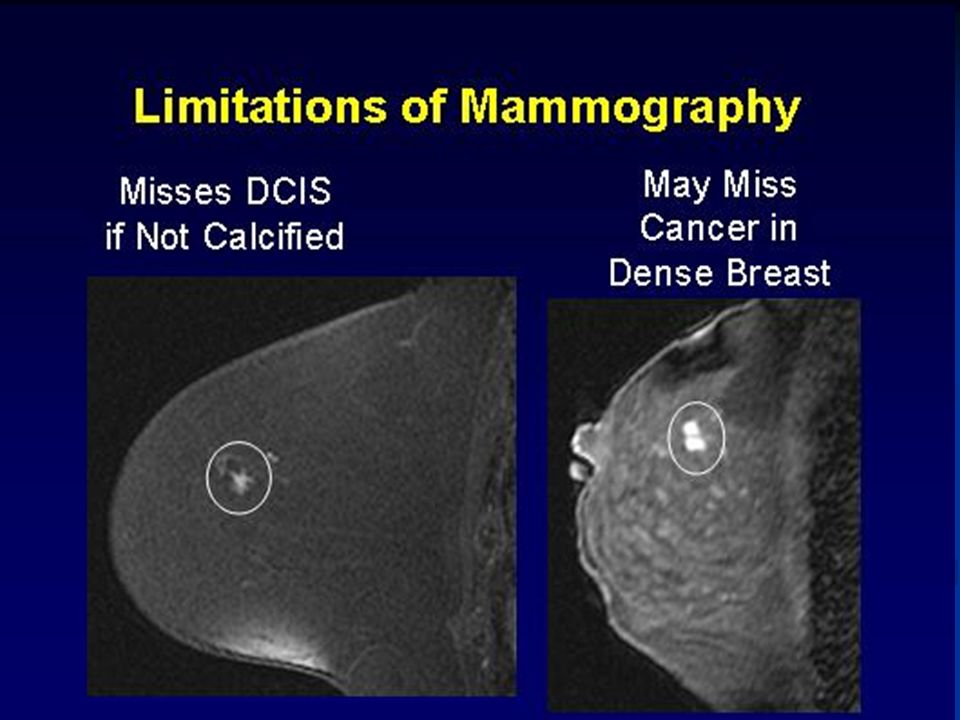
Most breast cancers are non palpable masses discovered only on screening mammograms
Malignant breast densities have irregular borders, are stellate and distort surrounding architecture

29
Breast Cancer Detection
United States Preventive Services Task Force Mammogram every 1-2 years for female age 40-49(average risk) Age > 50 annual mammography and clinical exam Age > 70 debatable Mammography detects only 85% of biopsy proven breast cancer hence not a substitute for tissue sampling of palpable mass
 Age > 50 annual mammography and clinical exam. Age > 70 debatable. Mammography detects only 85% of biopsy proven breast cancer hence not a substitute for tissue sampling of palpable mass.")
30
Breast Cancer Screening
There is almost universal agreement that randomized controlled trials of screening have demonstrated death rate from breast cancer can be reduced by periodic screening with mammography

32
MRI Breast Implant evaluation Axillary adenopathy ?occult primary
Breast cancer patients (extent of disease, response to neoadjuvant therapy) Screening evaluation for high risk patient Further evaluation of mammographic abnormality
 Screening evaluation for high risk patient. Further evaluation of mammographic abnormality.")
33
Staging of breast cancer
Estimate extent of disease Determine prognosis Guide therapy

34
Staging of breast cancer
Stage 0 (DCIS) Stage I node negative Stage II node positive Stage III advanced node Stage IV distant metastasis 2003 AJCC staging change Distinction between micrometastasis and isolated tumor cells Identifiers for sentinel nodes #number of positive LN
 Stage I node negative. Stage II node positive. Stage III advanced node. Stage IV distant metastasis AJCC staging change. Distinction between micrometastasis and isolated tumor cells. Identifiers for sentinel nodes. #number of positive LN.")
37
Management of Early stage breast cancer
1950 Halsted “radical mastectomy” “breast cancer spreads in an orderly fashion” 12% 10 year survival 20-30% node negative breast cancer patients will develop metastatic disease Micrometastatic disease paradigm

38
Management of Early stage breast cancer
Radical Mastectomy Whole breast radiation Axillary dissection Lumpectomy Partial breast radiation Sentinel node biopsy MORE LESS

39
Surgical intervention for Breast Cancer
NSABP B-04 Total Mastectomy + Axillary dissection Lumpectomy + Breast radiation Lumpectomy alone No difference in Overall Survival or Disease Free Survival (20 year follow-up) Fisher et al.NEJM2002;347:
 Fisher et al.NEJM2002;347:")
40
Surgical Intervention of Breast Cancer
NSABP B-04 Cumulative incidence of ipsilateral breast cancer Standard of care: lumpectomy+ Xrt 39% 14%

41
Surgical intervention for Breast Cancer
NSABP B-04 Fisher,et al.NEJM(2002):347;
:347;")
42
Surgical Staging of Axilla
Axillary dissection= removal of level I and Level II lymph nodes Morbidity : wound infection motion restriction arm stiffness pain lymphedema

44
Sentinel node mapping

45
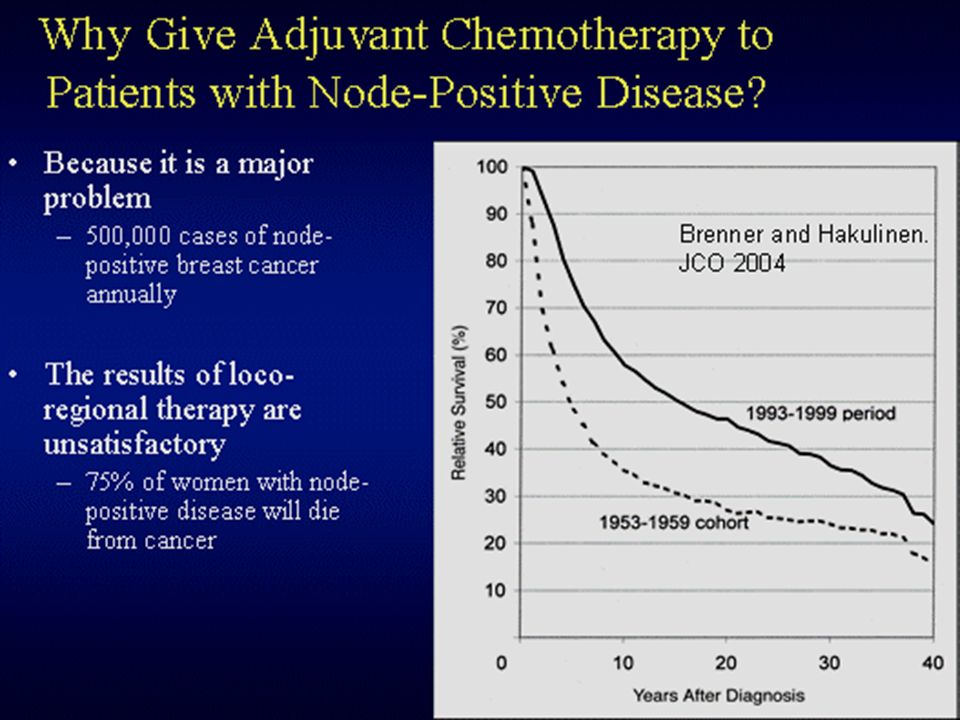
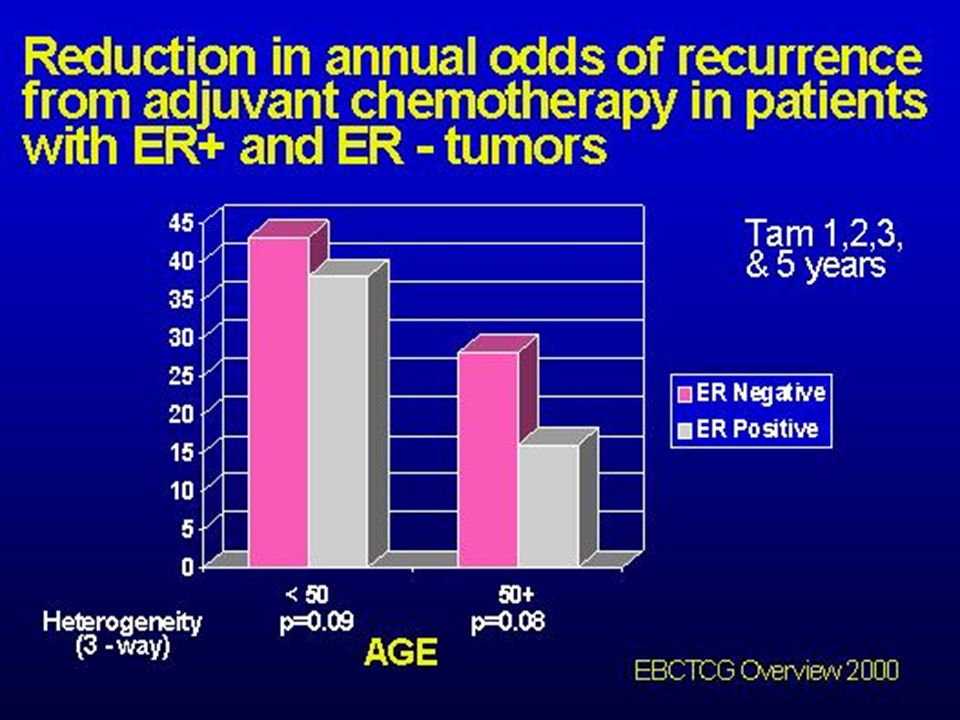
Chemotherapy for early stage breast cancer

49
Prognostic factors in Breast cancer
Recognized Factors Potential factors Proliferative index Tumor grade Vascular invasion Her- 2 Gene microarray Nodal status Tumor size Histologic type ER/PR

50
Prognostic factors in Breast cancer
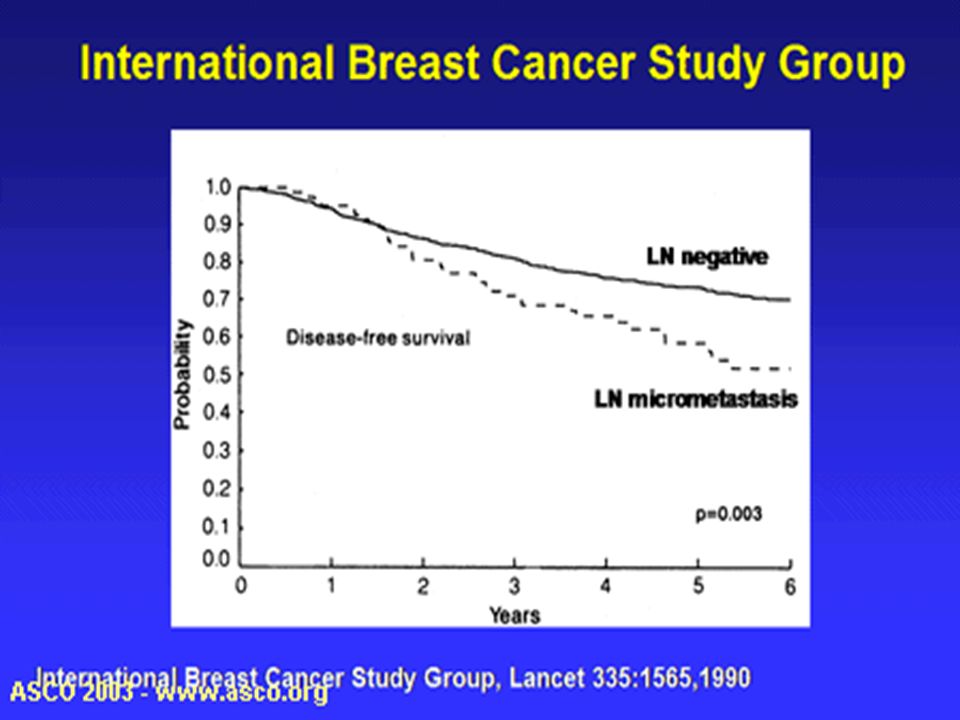
The most significant prognostic indicator for patients with early stage breast cancer is the presence or absence of axillary lymph node involvement.

52
Prognostic factors in Breast cancer
Recognized Factors Potential factors Proliferative index Tumor grade Vascular invasion Her- 2 Gene microarray Nodal status Tumor size Histologic type ER/PR

53
Prognostic factors in breast cancer
Multigene assay: Paik et al.NEJM 2004;351:

54
Gene Microarray

55
Multigene assay to predict recurrence in node negative breast cancer

56
HER- 2/neu Her-2/neu oncogene encodes for transmembrane receptor belonging to EGFR family Amplified in 25-30% breast cancer Overexpression associated with tumor aggressiveness and increased rates of recurrence

57
Her-2/neu Basis for molecular targeted therapy with Herceptin

58
NCI clinical alert –April 25,2005
NSABP B-31 Operable breast cancer Her 2 +, node + Randomization 52% decrease in disease recurrence AC x4cycles Taxol x4 cycles + Herceptin AC x4cycles Taxol x4 cycles

59
Thank you !

Similar presentations








: Department.>")








>")





