Download presentation
Presentation is loading. Please wait.

1
Botulinum toxin EUROPIAN JORNAL OF NEUROLOGY 2006,13 (suppl. 1)
")
2
Pharmacology of botulinum toxin : difference between type A preparation

3
Pharmacological difference between botulinum toxin types at molecular level It acts by blocking the docking and fusion of SNARE proteins at neuromuscular junction The SNARE proteins targeted by different BoNT vary : BoNTA and BoNTE cleave synapsomal –associated protein SNAP-25 BoNTB, BoNTD, BoNTF, BoNTG cleave synaptobrevin or vesicle associated membrane protein BoNTC1 uniqelly cleave both SANP-25 and syntaxin The duration of action is longest for BoNTA BoNT has heavy and light chain domains Heavy chain is binding domain Light chain act as a catalytic domain

4
Pharmacological difference between botulinum toxin types at molecular level The receptor type that it acts upon are Cholinergic endings of neuromuscular junction and the autonomic pre and post –ganglionic synapses Synapse–rich areas of the hippocampus, cerebellum and Renshaw cells BoNT is more effective when it is injected in activated muscle BONT does not cross BBB rather is transported by retrograde axonal transport to the spinal cord and cranial motor nuclei

6
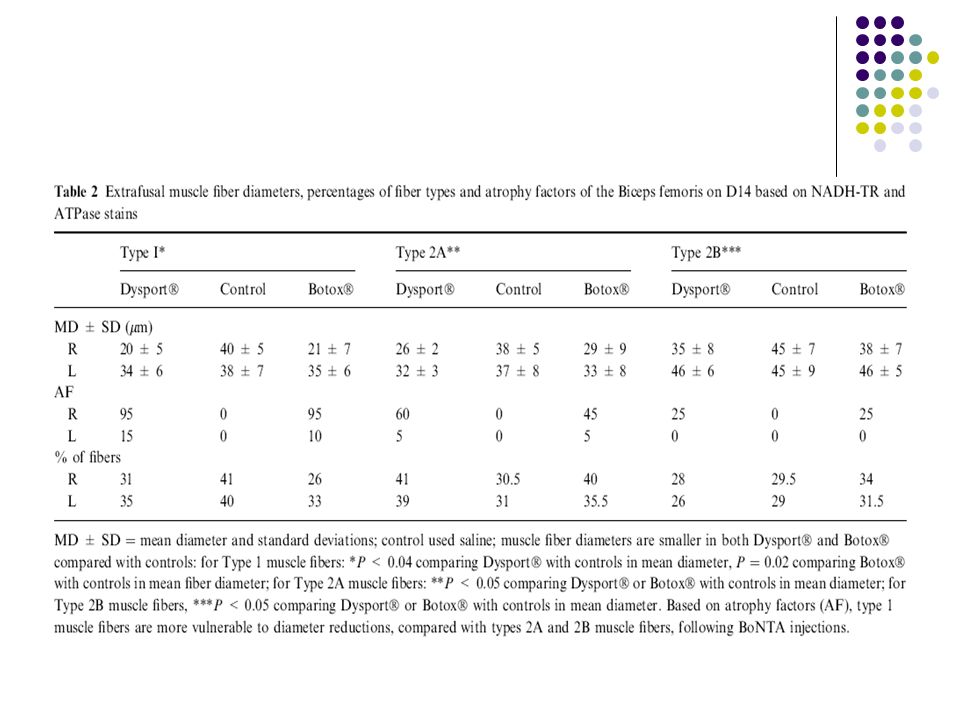
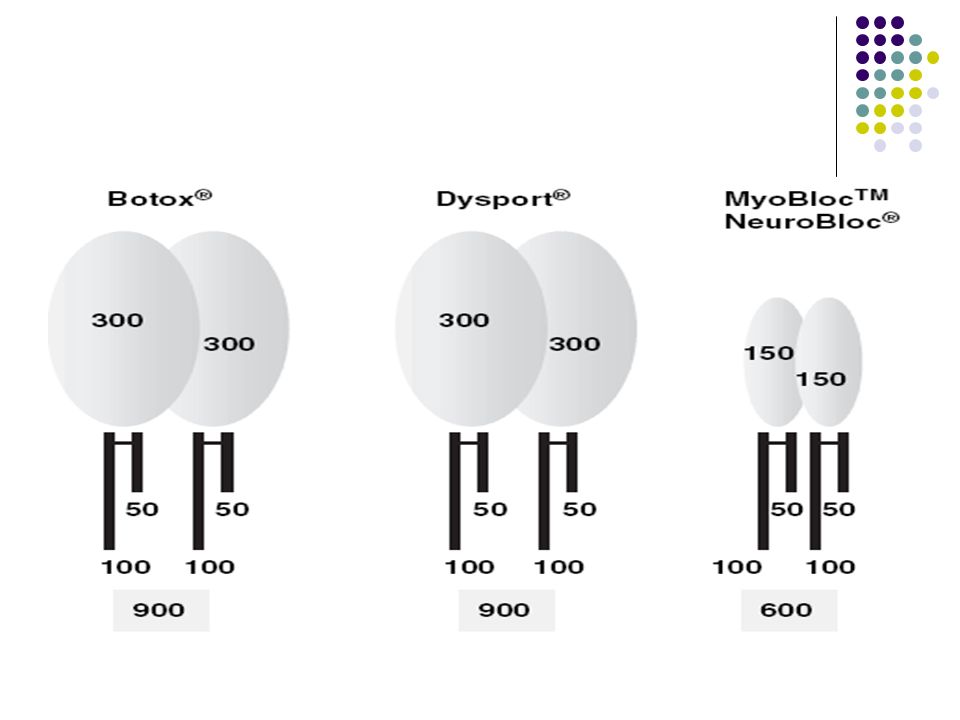
Comparison between Botox and Dysport at the experimental level

10
Conclusion Pharmacological differences between BoNT preparation are influenced by : Properties intrisic to the drug eg. protein load Muscle selection eg. Muscle activity pattern,muscle architecture and fascial planes Injection technique eg. Volume, dilutions and doses Botox to Dysport dose conversion ratio of 1 : 2.5 -3 is workable At therapeutic doses Dysport seems to produce more adverse effects

11
Immunological aspect of Botox,dysport and Myobloc/neurobloc

12
Treatment parameters as risk factor for botulinum toxin antibody formation Short inter injection interval High BoNT dosages at each injection series Higher cumulative BoNT dosage Booster injections (with inter injection interval less than 2 weeks ) Female gender
 Female gender")
13
Patient characteristics as risk factor for botulinum toxin antibody formation The overall reactivity of the patients immune system Priming of BT antibodies by structurally similar environmental agent Although formal studies have not been performed in special patient characteristics, Allergies seem to play minor role in BT antibody formation

14
Botulinum toxin preparation as risk factor for botulinum toxin antibody formation

18
Conclusion Corrected specific biological activities are measure of antigenicity The lower the corrected specific biological activities the higher the antigenicity and hence antibody induced therapy failure Testing for neutralizing antibody against BTB revealed BT antibodies in 9.6 % of patients at 1 year 18.2% of patients at 18 months 22.6% of patients after 610 days It may produce antibody-induced treatment failure in as many as 44% of patients For BTA preparations the rate of antibody induced therapy failure is in the range of 5%

19
Treatment of cervical dystonia with botulinum toxin

20
Introduction Cervical dystonia is due to asymmetric contractions of neck and shoulder muscles Anterocollis Retrocllis Laterocollis Rotational Pain is present in up to 60% of patients and is the most disabling feature A variety of medications have been used to treat CD Anticholinergic Baclofen Benzodiazepins BoNT is the treatment of choice providing 85% improvement in CD

21
Botulinum toxin treatment for CD - efficacy and safety Both BoNTA and BoNTB are safe and effective Technical aspect of BoNT have not been adequately studied Number of muscles to inject Optimal dosing Number of injection sites for specific muscles Best means of muscle selection and injection Botullinum toxin injection technique Anatomy of neck muscles include >26 muscle pairs CD may be simple with two muscle activation or complex with multidirectional activation Selecting muscles for injection requires knowledge of the major neck muscles and their primary and secondary actions

22
Botulinum toxin treatment for CD - efficacy and safety Botulinum toxin doses for CD Dysport starting dose 500 units Botox dose range from 100 – 300U Myobloc /Neurobloc doses range from 2500 to 10 000 Publish recommendations for the doses of Botox and Dysport are available for individual muscles SCM 20U of Botox SCM 100U of Dysport

23
Target muscle selection for CD The role of EMG has not been defined Investigators using EMG guidance have reported increased benefit and the potential to use smaller doses The number of injection sites into cervical muscles range from one site in smaller muscles to eight sites in larger muscles

24
Duration of benefit CD The mean duration of benefit assessed to time of retreatment in randomized double blind study was 83.9 +/- 13.6 days for Dysport 80.7+/-14.4 days for Botox Duration of benefit tend to last longer in patients with moderate symptoms The greatest degree of improvement was after the first injection

25
Treatment failures in CD Primary non–responders 15-30% of CD patients Anterocollis is the major head posture Secondary failure in approximately 10 -15% patients Due to neutralizing antibody Common side effects following treatment include Dysphagia Dry mouth Neck weakness

26
Botulinum toxin in blepharospsm and oromandibular dystonia: comparing different toxin preparations

27
Oromandibular Dystonia

28
OMD FORM OF FOCAL DYSTONIA INVOLVES MASTICATORY, LOWER FACIAL, LAIBIAL AND LINGUAL MUSCULATURES Uncommon representing 5% all forms of dystonia Cranial dystonia OMD plus blepharospsm the second most common form of dystonia Etiology Idiopathic most patients Blepharospsm, cervical dystoina, and spasmodic dysphonia are more commonly associated with idiopathic OMD Tardive dystonia the most common cause of secondary OMD Neurodegenerative neuroacanthocytosis

31
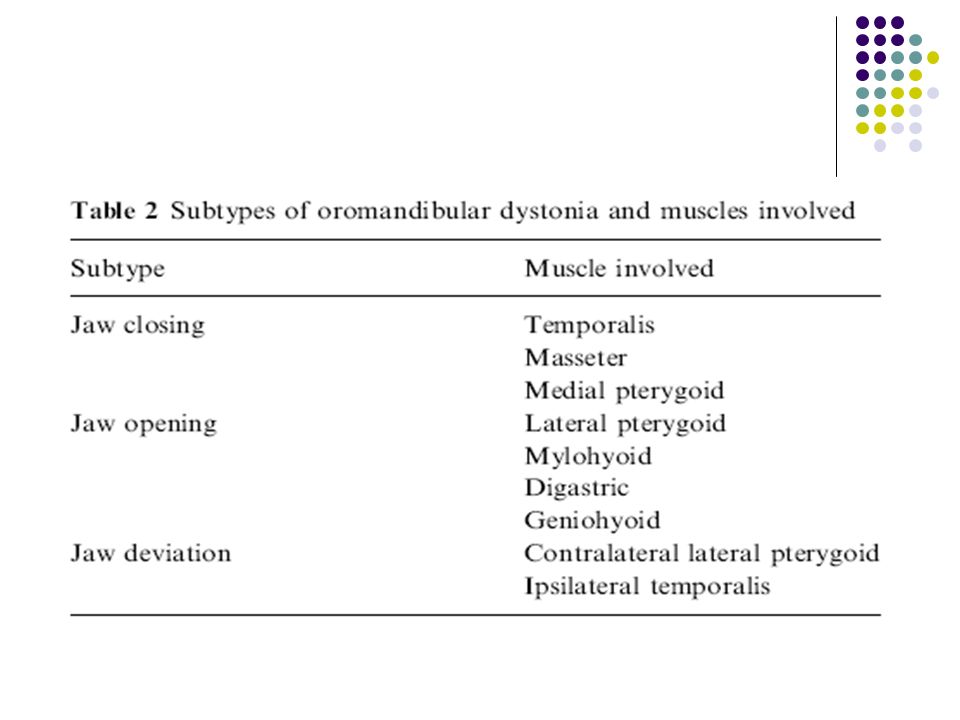
Treatment options for OMD OMD responds poorly to oral medications Anticholinergics Tetrbenzine Baclofen Clonazepam Muscle afferent block helpful but needs further evaluation Lidocaine and alcohol Pallidial deep brain stimulation Botullinum toxin the therapy of choice Jaw opening Jaw closing Jaw deviation Mean total duration of response 16.4+/-7/1 weeks The best response obtained with jaw closing

32
Injection techniques Jaw closing Masseter the initial muscle to be denervated Botox 50U Dysport 100U Medial pterygiod Approached intra orally or from below EMG verification needed when approached from below Botox 20U Dysport 30U Temporalis muscle Three to four injections should be given Butox 40U Dysport 100U

33
Injection techniques Jaw opening dystonia Lateral pterygoid Approached intra orally or laterally EMG recommended in the lateral approach Botox 20 -40 U Dysport 60 U Digastric muscle Injection should be given on the anterior belly Mylohyoid 1 cm from the mandibular tip and lateral to the midline Botox 20U Dysport 90U platysma

34
Injection techniques Lingual OMD Exrinsic muscles of the tongue Genioglossus Hypoglossus Styloglossus Palatoglossus Tongue trusting is the most common movement in OMD Posterior fibers of Genioglossus Botox 10U Dysport 30U The treatment of lingual dystonia is often difficult and the success rate is usually low

35
Injection techniques Pharyngeal OMD Pharyngeal muscles Three constrictor muscles Stylo-, salpingo-,and palatopharyngie muscles Patient often complain of choking and swallowing difficulty Often occurs with spasmodic dysphonia Constrictor pharynges invariably involved with dysphagia For Dysport 30U

36
Blepharospasm

37
Clinical features Focal dystonia with involuntary closure of the eyes Due to spasm of the orbicularis occuli Begins 5 th to 6 th decade of life Females are affected more Apraxia of the eye lids Due to failure to activate levator palpebra muscle Does not respond well to botulinum toxin Blepharospasm and apraxia of eye opening may coexist together

38
Etiology Psychogenic Idiopathic Secondary in only 10% Reflex due to local conditions Neurodegenerative disorders PD,HD, WILSON’S,CJ,PSP

39
TREATMENT OPTIENS Conservative treatment Sun glasses Benzodiazpines Anticholinergic Botulinum toxin injection Superficially over the orbicularis oculli The corrugator muscle injected intramuscularly orbicularis oculli is injected at five sites with total dose of 12.5-20 for Botox Avoiding injection of the medial 2/3 of the eye lid is important Effect lasts for up to 12 weeks

41
Botulinum toxin therapy of hemifacial spasm

42
Introduction Involuntary irregular clonic or tonic movements of the muscles innervated by the 7 th nerve on one side Most often the result of vascular compression of the VII nerve Typical HFS Compress the non-facicular portion of facial nerve Anterior aspect Caudal aspect Atypical HFS Compress the posterior or rostral portion Initiate at orbicularis oris,businator And spread to involve the orbicularis oculli Prevalent in females and in those 40-79 Facial weakness can develop Symptoms tend to persist during sleep Occurs usually unilaterally Non vascular causesof HFS :neuroma,cystic tumor

43
Ddx Blepharospsm Facial myokymia OMD Facial tic Masticatory spasm Post –Bell’s palsy synkinesis Focal seizure

44
Treatment Medications Baclofen Clonazepam Carbamazepine Gabapentin Phenytoin Microvascular decompression 88-97%sucess rate Doxorubicin Botulinum toxin

48
Botulinum toxin therapy of laryngeal muscle hyperactivity syndromes : comparing different toxin preparations

49
Introduction Spasmodic dysphonia is focal dystonia characterized by task specific, action induced spasm of the vocal cord First described in 1871 by Traube It can occur independently or as part of Meige’s syndrome or in other disorders like Tardive dyskinesia There are three types of SD: the adductor type,the abductor type and the mixed type The adductor type is characterized by strain-strangled voice quality and intermittent voice stoppage or breaks due to over adduction of the vocal folds Abductor spasmodic dysphonia is characterized by intermittent breathy breaks,associated with prolonged abduction folds Patients with mixed type have features of both It affect patient in their mid forties and is more common in females

50
Treatment options for ADSD Surgery Botulinum toxin 97%improvment 35%mild breathiness Choking in 15% Muscles injected Thyroarytenoid muscle Lateral cricoarytenoid muscle Injection protocols Unilateral decrease side effects Bilateral increase side effect/prolonged duration of benefit Injection technique Percutaneous approach ( EMG between cricoid and thyroid cartilage ) Trans oral approach indirect laryngoscopy Trans nasal approach Point touch injection through thyroid cartilage half way b/n notch and lower border
 Trans oral approach indirect laryngoscopy Trans nasal approach Point touch injection through thyroid cartilage half way b/n notch and lower border")
53
Botulinum toxin therapy for writers cramp

54
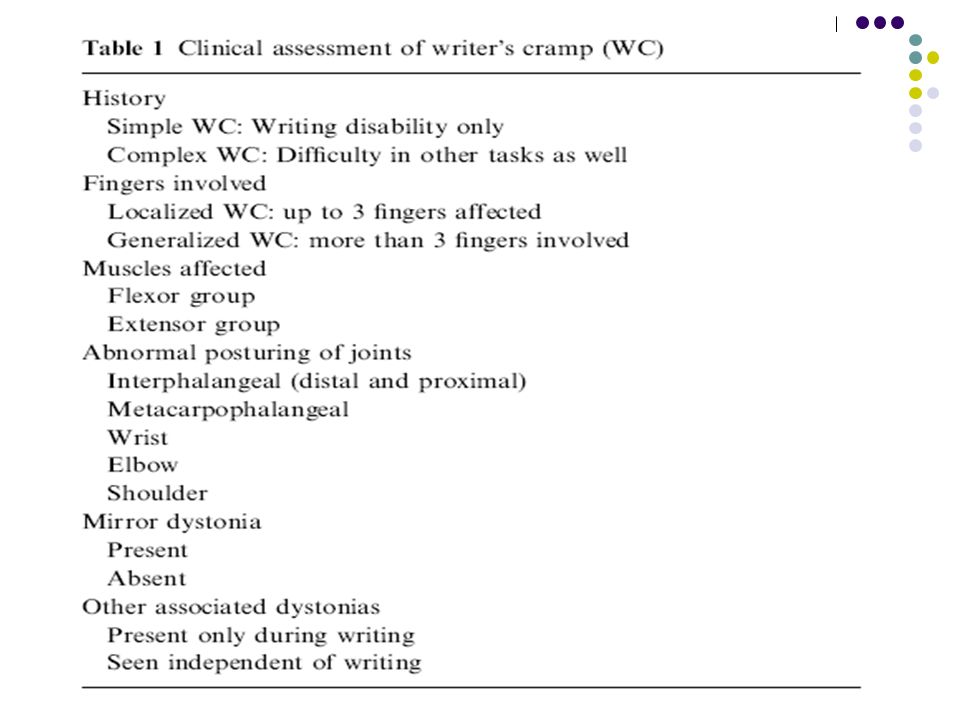
Introduction First reporeted in the 18 th century under the title ‘occupational palsy ‘ disabling spasm only when they write On other tasks requiring the same hand muscles they perform normally Incidence 14per 1 000 000in Europe Contrary to other dystonias WC is more frequently seen in males

55
Etiology Unknown Deficient activation of the premotor cortex Loss of inhibition during generation of muscle command Excessive activation of antagonist Over flow into synergist Prolongation of muscle activation Decreased level of GABA In the contralateral sensory motor cortex In the contralateral lentiform nucleus There is evidence that dystonia is a sensory disorder as well as a disorder of movement preparation Functional MRI showed impairerd activation of Primary sensorimotor cortex Supplementary motor cortex Persistent increase of Basal Ganglia activity after cessation of task

57
Treatment of WC Limb immobilization by plastic splint for 4-5 weeks Sensory training by Braille reading 30 minutes /day for 1 year cooling of the hand and forearm muscles Low frequency and low dose transcranial magnetic stimulation Botulinum toxin Effective in 80% Benefit starts at 1 week and peaks at the 2 nd week improvement last for 3 months

59
Other indications of botulinum toxin therapy Cranial application other than dystonia Strabismus Protective ptosis Bruxism Rhinitis Lacrimation wrinkles Others Foot dystonia Axial dystonia Tourettet’s disorder Hyperhidrosis urologic disorder Achalasia Anal fissure

60
Thank you !

Similar presentations
















>")
 in Drake et al.>")







 BoNT A and BoNT B are essentially the same and interchangeable B)>")






