Download presentation
Presentation is loading. Please wait.

1
How Well is SCHIP Meeting Children’s Primary Health Care Needs?: Findings From A Congressionally Mandated Study Genevieve Kenney The Urban Institute Jamie Rubenstein Cornell University Anna Sommers University Of Maryland Baltimore County Grace Ko Gunderson Dettmer Stough Villeneuve Franklin and Hachigian, LLP Academy Health Annual Research Meeting Washington, DC June 10, 2008 Funding for this research was provided under a Congressionally- mandated evaluation for ASPE

2
Background on the State Children’s Health Insurance Program SCHIP was created in August 1997 to allow states to extend public health insurance coverage to uninsured children not eligible for Medicaid All states chose to expand eligibility for children under SCHIP: Eligibility thresholds vary from 140% in North Dakota to 350% in New Jersey, but most states set eligibility levels at 200% FPL States can expand Medicaid, create a separate SCHIP program, or use a combination approach Over two-thirds of states adopted separate programs, either alone or in combination with smaller Medicaid expansions Separate programs’ benefits approach breadth of Medicaid and are broader than most private insurance, covering: –Preventive services in accordance with AAP guidelines –Dental, hearing, and vision screening

3
Research Questions How do access and use outcomes and parental perceptions about being able to meet their child’s health care needs vary across groups of enrollees, including: –The Race/ethnicity of the child and primary language spoken –Highest education level of the parents –Child’s health status How do these measures vary across the 10 states studied? Do these differences persist when controlling for other socioeconomic and demographic characteristics?

4
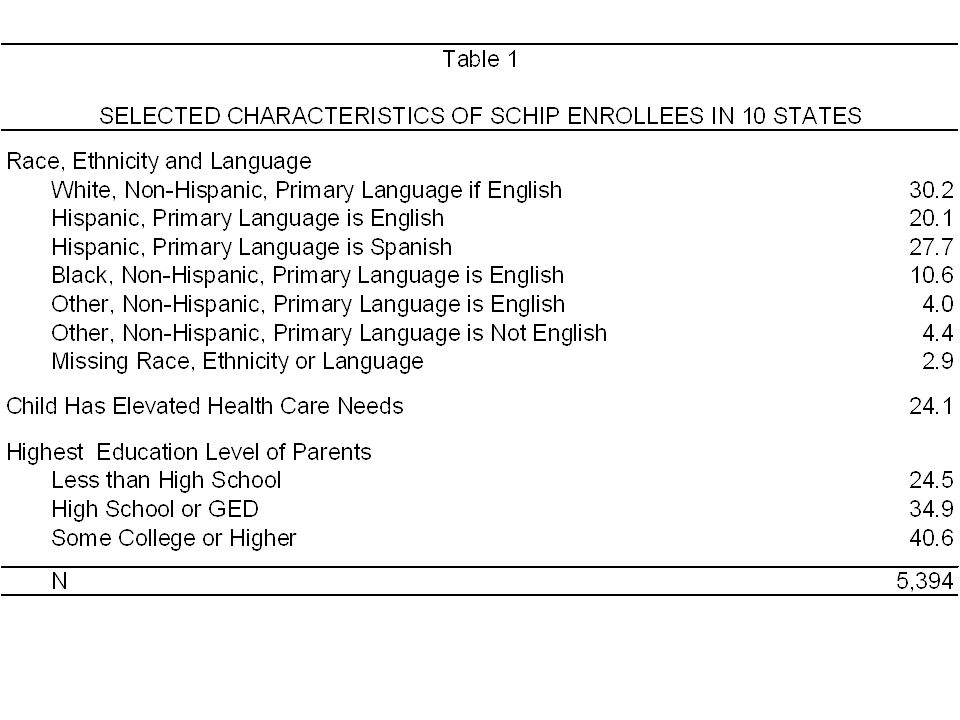
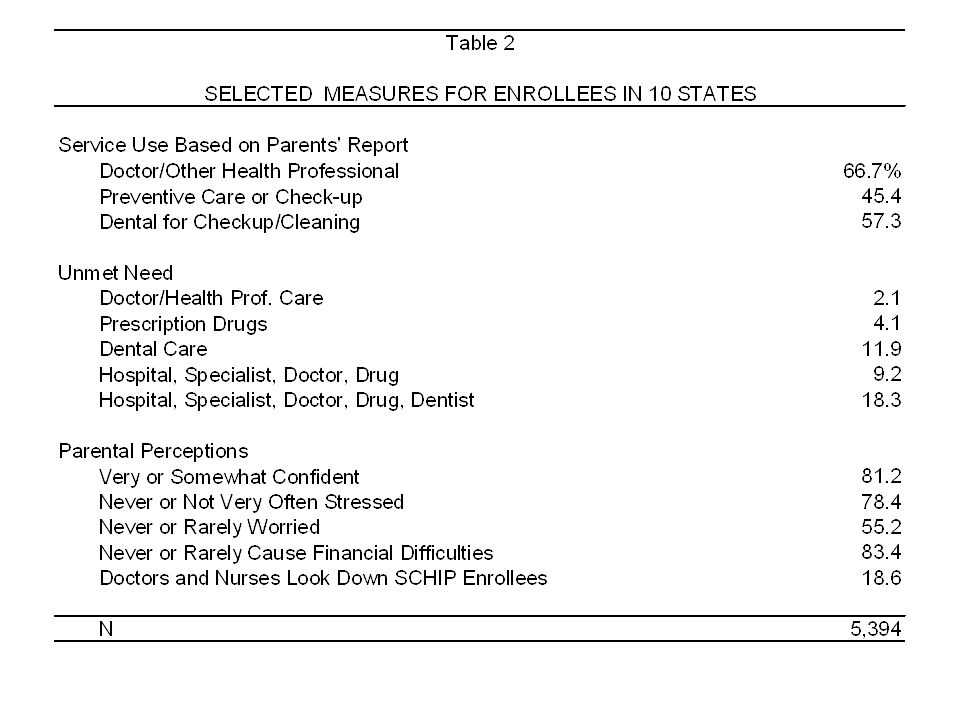
Data Data analyzed comes from the “2002 congressionally mandated survey of SCHIP enrollees and disenrollees in 10 states.” SCHIP enrollees surveyed in 10 states (CA, CO, FL, IL, LA, MO, NC, NJ, NY, TX) containing 60% of SCHIP enrollees nationally and representing all 3 program types. Analysis includes 5,394 SCHIP enrollees who had been in the program six months or longer. Outcomes examined include: –Service Use –Unmet Need –Attitudes and Worry –Presence/Type of Usual Source of Care –Provider Communication and Accessibility as Reported by Parent All measures refer to experiences over the past 6 months.

5
States Included in the Evaluation

6
Methods I will talk primarily about raw/unadjusted means. Adjusted and unadjusted means almost always show substantively similar results. However, when results differ substantively between raw and regression adjusted means, I will highlight these differences. Regression adjusted means control for –Child’s age, sex, health status, race/ethnicity, and interview language –Household income and size –Educational attainment/work status of parents –Parental attitudes toward efficacy of medical care –County of residence

14
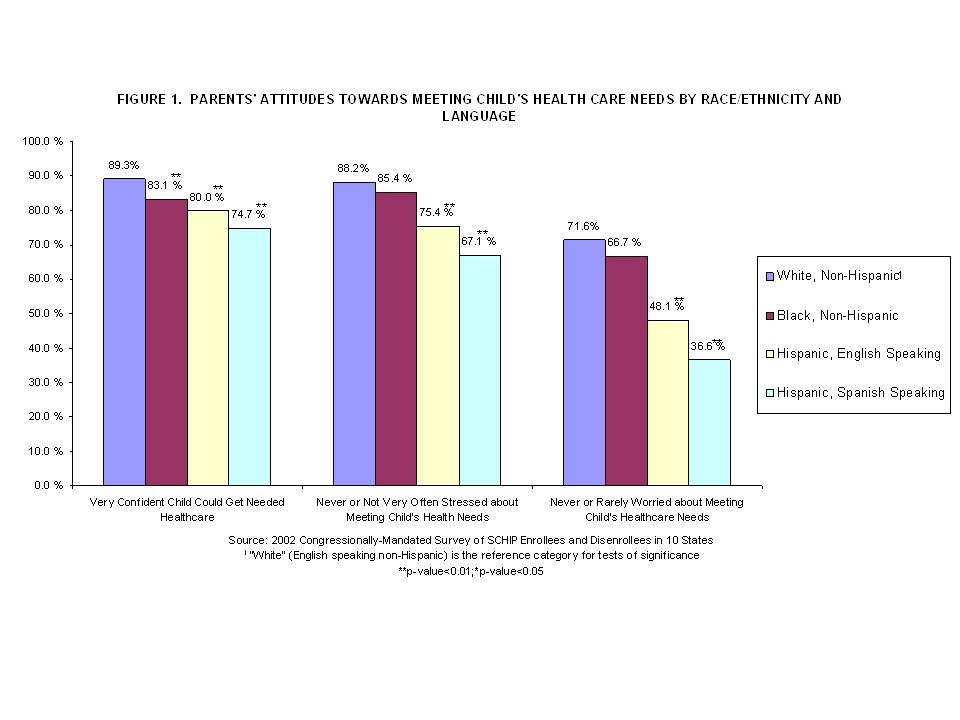
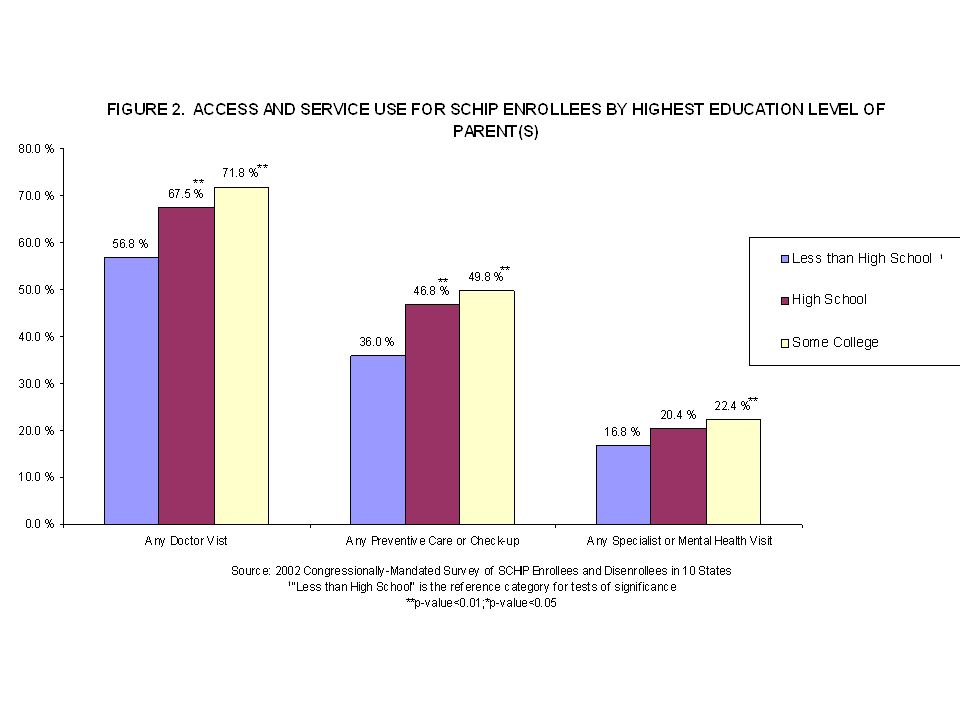
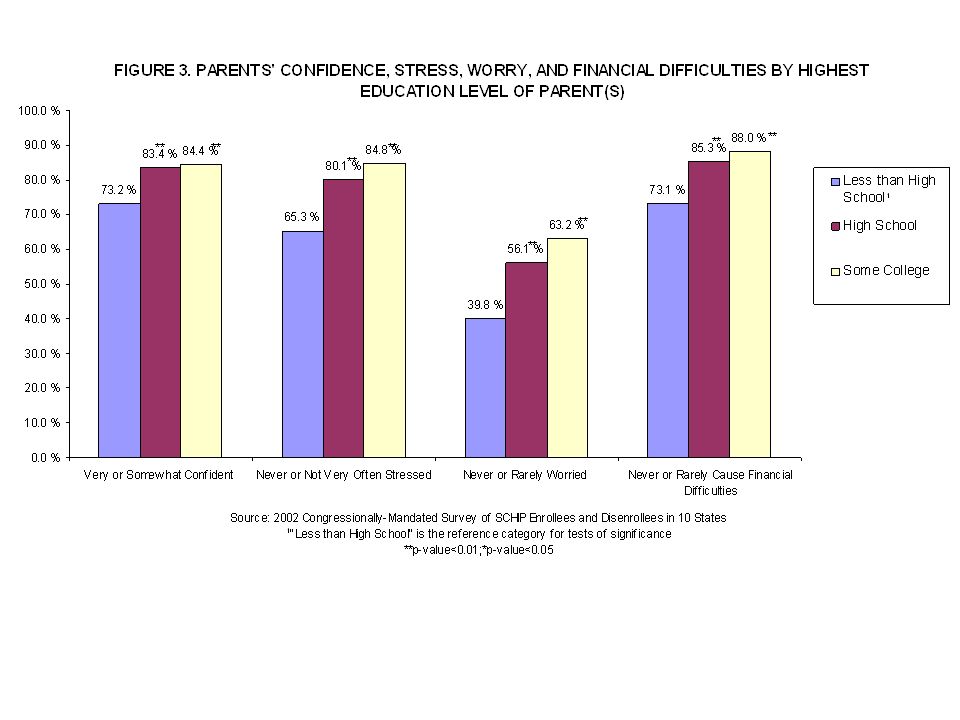
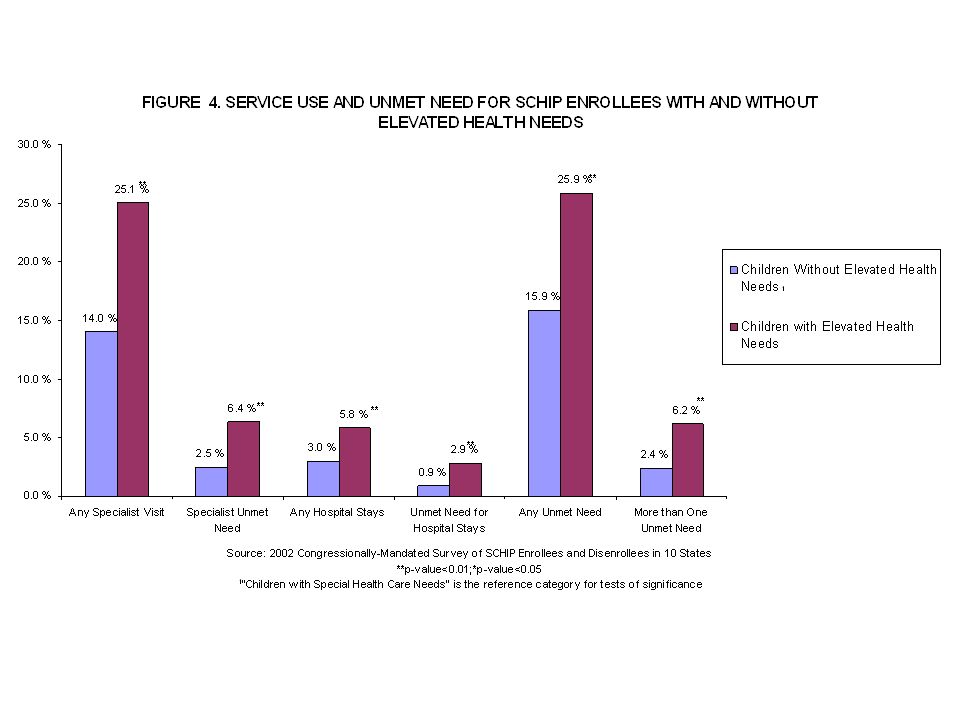
Conclusions Overall, SCHIP programs provide high levels of access to care. However, some groups of enrollees fared better than others. SCHIP enrollees whose parents have more education tend to receive more care, and their parents have fewer concerns about meeting their children’s health needs. SCHIP enrollees with elevated health care needs receive more care but have more unmet needs. In addition, their parents report greater levels of worry and financial difficulty associated with meeting their children’s health care needs. Hispanic enrollees, especially those whose primary language is Spanish, have parents who experience greater stress and worry, have lower confidence, and are more likely to experience financial difficulty.

15
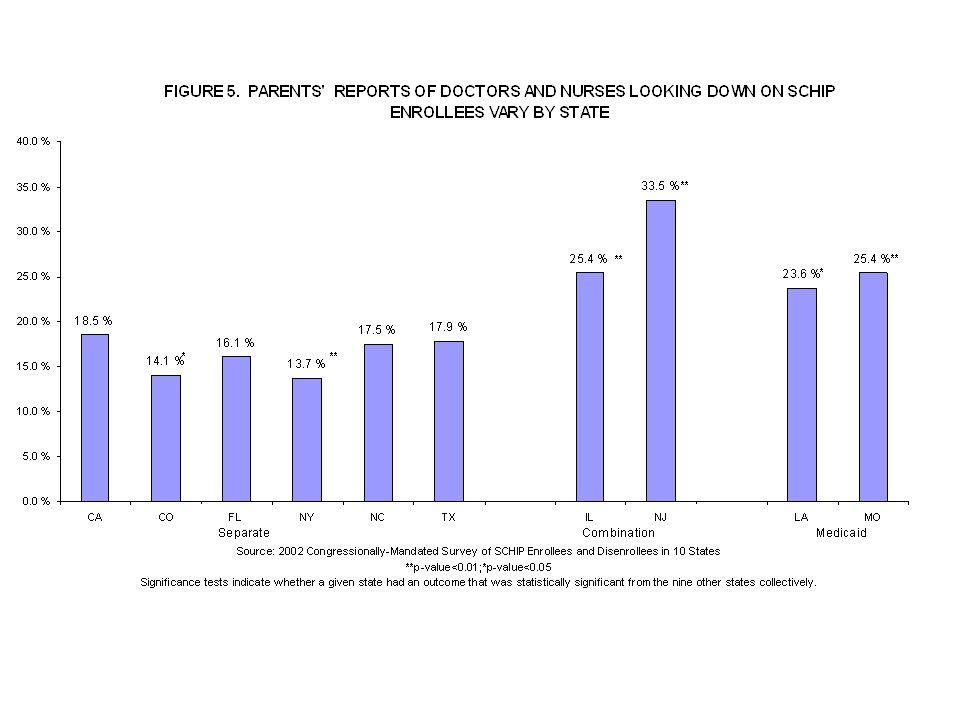
Conclusions (2) There was little cross state variation in access and use measures studied, though some differences do exist, including for dental care and type of usual source of care. Another difference is that families in states with Medicaid expansion or combination programs were more likely to feel providers “look down on” SCHIP enrollees, though it is unclear whether this is can be generalized to all 50 states.

16
Policy Implications Given that some groups of SCHIP enrollees experience greater difficulty accessing health care, states may have to target more resources at children of parents with lower education levels, Hispanic children, and children with elevated health care needs to help them make better use of the services available to them. These findings also suggest a need to develop policies that improve how providers treat public clients, particularly in combination and Medicaid expansion programs. In light of the differences that are found across subgroups, as Congress debates changes in SCHIP for its reauthorization, it will be important to consider how the state and federal governments could strengthen the monitoring and reporting of quality and access to care for SCHIP and Medicaid enrollees, particularly for vulnerable subgroups.

Similar presentations