Download presentation
Presentation is loading. Please wait.

1
WHO Public Health Strategies for developing palliative NCCP Barcelona, March 2011 Jan Stjernswärd MD PhD FRCP (Edin)
")
2
Ethics begins in the opening that freedom provides- the thought that things should be other than they are and the confidence to make that future concrete

3
Highest stage of moral reasoning is not ruled by self-interest, the opinion of others, fear of punishment but live according to self imposed universal principles such as those of justice and respect for the dignity of persons

4
All humans’ beings share a condition that requires a range of common responses – this week – deal with the threat of mortality, un-nessecary pain and suffering and wish for a good quality of life as well as death

5
Value pluralism. Some cultures values autonomy and individuality many others value social cohesion, community and tradition more highly

7
Do it Your own way death of parents in law Sri Lanka vs USA overmedicalised, commercialised vs Nordic Countries

8
Georgia (pain, no drugs, priests) Uganda (morphine free, PC Nurses can give morphine) Mongolia (incurable 80%, PC NCI,40 liver cancer, Vaccination, NCCP Referral polices, 39 million) USA (Disney land)
 Uganda (morphine free, PC Nurses can give morphine) Mongolia (incurable 80%, PC NCI,40 liver cancer, Vaccination, NCCP Referral polices, 39 million) USA (Disney land)")
9
Socio-economic and cultural solutions will be as important-if not more- than the medical efforts in achieving palliative care coverage

10
1986

14
Catalonia WHO Demonstration Project, started 1989 globally is the first having documented a comprehensive coverage (> 80%) in its population (> 6 million) for all in need of palliative care regardless of cause.
 in its population (> 6 million) for all in need of palliative care regardless of cause.")
15
“Socio-economic and cultural solutions will be as important- if not more, than the medical efforts in achieving palliative care coverage” “A medical Institutionalized approach will not reach all in need of palliative care in a society, nor will the usual hospice approach” “…Catalonia serves as a brilliant model, for the importance of an integrated GOV and community NGO approach. Each one in isolation, will not achieve much”

17
Wisconsin WHOCC (first, oldest) Oxford WHOCC (NPCP, Education) London WHOCC (latest) Catalonia WHOCC (Rolls Royce ) Kerala WHOCC (community approach)
 Oxford WHOCC (NPCP, Education) London WHOCC (latest) Catalonia WHOCC (Rolls Royce ) Kerala WHOCC (community approach)")
19
Kerala NNPC Succeeded making PC a peoples movement Established high ethical standards covering most terminally ill Demonstrated an alternative to present over medicalised, over specialized and in long run unaffordable care of the dying Shown financial sustainability Shown that social support, psychological support, nursing care and partially medical management can be done by the community Stjernsward: Indian J Pall Care. December 2005

20
Palliative Medicine – The Global Perspective: Closing the Know-Do Gap Jan Stjernswärd and Xavier Gómez-Batiste

21
Ministry of Health Officials Other Ministries e.g. Social Affairs, Higher Education, Women’s Affairs International GOV organizations and NGO (e.g. WHO, EU, IAHPC, UICC) Directors Cancer Centers, AIDS, Geriatric Drug regulators Chief Pharmacist Deans Medical Schools Deans Directors Nursing Schools Representative Family doctors /GPs Rep. Social Workers National NGOs, Religious Org. Journalists/advocacy Relevant leading clinicians, doctors/nurses International Faculty /Resource person (s) Walch D, Pall Med (in Press) :Stjernsward J Gomes Batiste X Participants NPCP Policy Workshop
 Directors Cancer Centers, AIDS, Geriatric Drug regulators Chief Pharmacist Deans Medical Schools Deans Directors Nursing Schools Representative Family doctors /GPs Rep. Social Workers National NGOs, Religious Org. Journalists/advocacy Relevant leading clinicians, doctors/nurses International Faculty /Resource person (s) Walch D, Pall Med (in Press) :Stjernsward J Gomes Batiste X Participants NPCP Policy Workshop.")
27
Factors influencing a patient’s perception of pain Other symptoms Adverse effects of treatment PHYSICAL Total Pain ANXIETY DEPRESSION ANGER Fear of hospital or nursing home Fear of pain Worry about family and finances Fear of death Spiritual unrest, uncertainty about future Loss of social position Loss of job prestige and income Loss of role in family Insomnia and chronic fatigue Sense of helplessness Disfigurement Bureaucratic bungling Delays in diagnosis Unavailable physicians Uncommunicative physicians Failure of therapy Friends who do not visit WHO: Cancer Pain Relief and Palliative Care, TRS 804, WHO,Geneva 1990 Total Pain

28
Hospice T T PC T

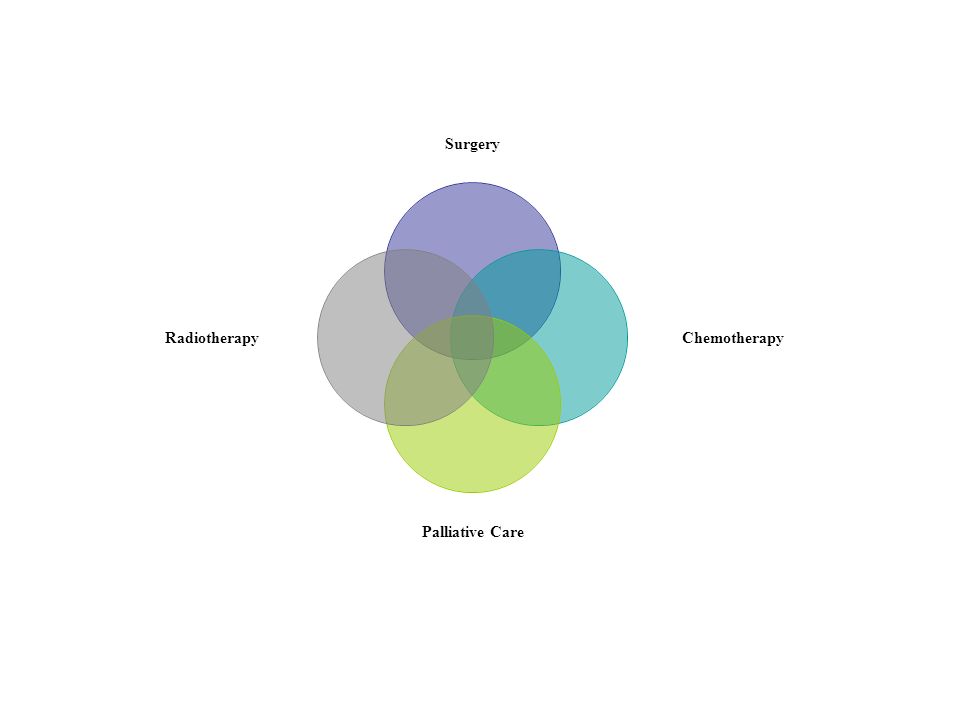
29
T NCCP PP PC ED T Pillars of National Cancer Control Programs

31
T Education Implementation Policy Drug Availability WHO Strategy: Foundation Measures

32
NS/WHO 3 first foundation measures: Cost little, but BIG effect Curbing pain and suffering in a most cost-effective way, that even may save money, as shown by Catalonia

33
Implementation- Closing the “ Know-Do-Gap ”: Finances Manpower Instituonalisation

34
Example access to essential medicines 71 court cases from 12 countries analyzed. In 59 cases access to essential medicines was enforced through the courts as part of the right to health. Hogerzeil et al.

36
Conclusion Our Might for the Patients Right will be that we know the solution and have the knowledge to deliver it.

37
Remember the 3 Ts: Things Takes Time

Similar presentations




























>")
