Download presentation
Presentation is loading. Please wait.

1
IN THE NAME OF GOD

2
15 y CC: Abdominal Pain+Primary Amenorrea PMH: (-)
FH: Her sister had gross Hematuria during menstural cycle. PH/EX: NL Diagnosis: Sonography UT=NL ET=2mm 7×5 cm mass Treatment: Surgery 3×4 cm Ovaries:NL

3
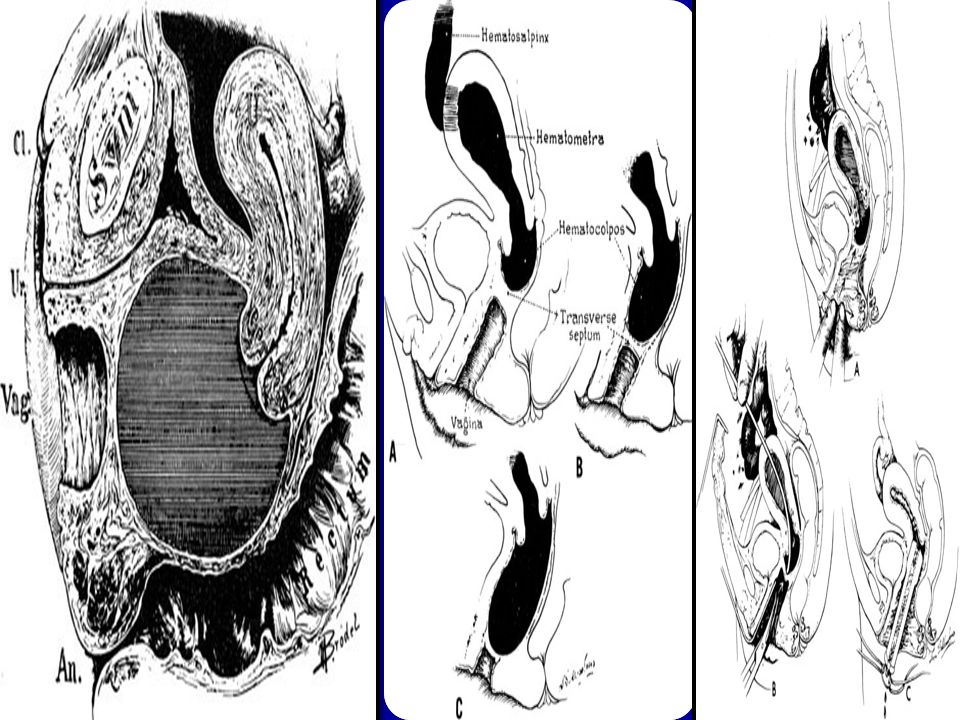
Fig. 1. Unilateral obstruction of a horn (A) and the vagina (B)
Fig.1. Unilateral obstruction of a horn (A) and the vagina (B). When there is failure of lateral fusion of the müllerian ducts with unilateral obstruction, absence of the ipsilateral kidney is the rule. Thus, an intravenous pyelogram is an essential diagnostic tool and may clarify the diagnosis in obscured circumstances.(Rock JA: Diagnosing and repairing uterine anomalies. Contemp Obstet
 and the vagina (B). When there is failure of lateral fusion of the müllerian ducts with unilateral obstruction, absence of the ipsilateral kidney is the rule. Thus, an intravenous pyelogram is an essential diagnostic tool and may clarify the diagnosis in obscured circumstances.(Rock JA: Diagnosing and repairing uterine anomalies. Contemp Obstet.")
4
Fig. 2. Double uterus, complete or incomplete vaginal obstruction, and ipsilateral renal agenesis. A. Complete vaginal obstruction. B. Incomplete vaginal obstruction. C. Complete vaginal obstruction with a lateral communicating double uterus.(Rock JA, Jones HW Jr: The double uterus associated with an obstructed hemivagina and ipsilateral renal agenesis. Am J Obstet Gynecol 138:340, 1980)
.")
8
Vaginal septum viewed on vaginoscopy

9
INTRODUCTION Amenorrhea (absence of menses) is often classified as either primary (absence of menarche by age 16) orsecondary (absence of menses for more than three cycle intervals or six months in women who were previously menstruating).
 is often classified as either primary (absence of menarche by age 16) orsecondary (absence of menses for more than three cycle intervals or six months in women who were previously menstruating).")
10
DEFINITION Primary amenorrhea is defined as the absence of menses at age 16 in the presence of normal growth and secondary sexual characteristics. At age 13, if no menses have occurred and there is an absence of secondary sexual characteristics, such as breast developmentevaluation for primary amenorrhea should be begun. The American Fertility Society

11
ETIOLOGY Chromosomal abnormalities causing gonadal dysgenesis— 50 %
Hypothalamic hypogonadism — 20 % Absence of the uterus, cervix and/or vagina, müllerian agenesis — 15 % Transverse vaginal septum or imperforate hymen — 5 % Pituitary disease — 5% The remaining 5 % of cases are due to a combination of disorders including androgen insensitivity due to mutations in the androgen receptor, congenital adrenal hyperplasia, and polycystic ovary syndrome.

12
Congenital anatomic lesions of the uterus and vagina
Pelvic or lower abdominal pain is a common presenting symptom in girls with primary amenorrhea and an obstructed reproductive tract.

13
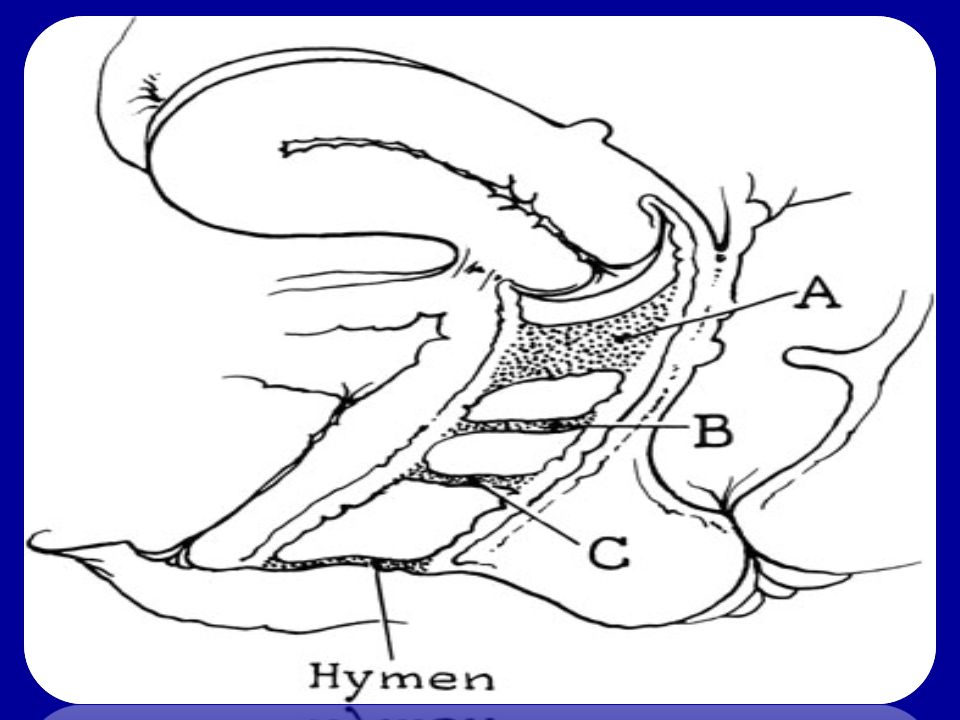
Imperforate hymen An imperforate hymen is the simplest defect that results in primary amenorrhea. It may be associated with cyclic pelvic pain and a perirectal mass from sequestration of blood in the vagina (hematocolpos). Similar findings can be seen with defects in perineal development, which can result in absence of the distal third of the vagina and therefore absence of an outflow tract. Both of these conditions are diagnosed by physical examination. An imperforate hymen is easily corrected with surgery.
. Similar findings can be seen with defects in perineal development, which can result in absence of the distal third of the vagina and therefore absence of an outflow tract. Both of these conditions are diagnosed by physical examination. An imperforate hymen is easily corrected with surgery.")
14
Fig. 5 Imperforate hymen. Notice the thin, transparent hymen stretched over the dark-colored accumulated menstrual blood.

15
Transverse vaginal septum
One or more transverse vaginal septae can occur at any level between the hymenal ring and the cervix.

16
Vaginal agenesis Vaginal agenesis is usually accompanied by cervical and uterine agenesis.

17
DIAGNOSTIC EVALUATION
Primary amenorrhea is evaluated most efficiently by focusing on the presence or absence of breast development (a marker of estrogen action and therefore function of the ovary), the presence or absence of the uterus (as determined by ultrasound, or in more complex cases by magnetic resonance imaging) and the FSH level.
, the presence or absence of the uterus (as determined by ultrasound, or in more complex cases by magnetic resonance imaging) and the FSH level.")
18
DIAGNOSTIC EVALUATION
If the ultrasound indicates that the uterus is absent and FSH is normal, the probable diagnosis is mullerian agenesis or androgen insensitivity syndrome. In the case of mullerian agenesis, the circulating testosterone is in the normal range for women and in the case of androgen insensitivity the circulating testosterone is in the male range. If the FSH is normal, and both breast development and the uterus are present, then the work-up should focus on the common causes of secondary amenorrhea, where the initial work up includes measurement of height and weight, serum FSH, prolactin and TSH.

19
DIAGNOSTIC EVALUATION
Step I: History Has she completed other stages of puberty? Is there a family history of delayed or absent puberty, suggesting a possible familial disorder? Are there any symptoms of virilization? Has there been recent stress? Is she taking any drugs? Is there galactorrhea?

20
DIAGNOSTIC EVALUATION
Step II: Physical examination An evaluation of pubertal development An assessment of breast development A careful genital examination. Step III: Basic laboratory testing Uterus absent Uterus present

21
TREATMENT Treatment of primary amenorrhea is directed at correcting the underlying pathology.

22
congenital anomalies of the uterus
Congenital anomalies of the uterus are often asymptomatic and therefore unrecognized. They may affect a young woman due to pain at the time of menarche, or a woman's obstetric and/or gynecologic health. The American Fertility Society in 1988 produced a standard form for classification of müllerian defects (table1) Dr Bier 2006
 Dr Bier")
23
Type I: "Müllerian" agenesis or hypoplasia :
A. Vaginal (uterus may be normal or exhibit a variety of malformations) B. Cervical C. Fundal D. Tubal E. Combined Type II: Unicornuate uterus : A1a. Communicating (endometrial cavity present) A1b. Noncommunicating (endometrial cavity present) A2. Horn without endometrial cavity B. No rudimentary horn Classification of Müllerian anomalies according to the AFS classification system
 B. Cervical C. Fundal D. Tubal. E. Combined. Type II: Unicornuate uterus : A1a. Communicating (endometrial cavity present) A1b. Noncommunicating (endometrial cavity present) A2. Horn without endometrial cavity. B. No rudimentary horn. Classification of Müllerian anomalies according to the AFS classification system.")
24
Type III: Uterus didelphys Type IV: Uterus bicornuate: A
Type III: Uterus didelphys Type IV: Uterus bicornuate: A. Complete (division down to internal os) B. Partial C. Arcuate Type V: Septate uterus: A. Complete (septum to internal os) B. Partial Type VI: Diethylstibestrol-related anomalies: A. T-shaped uterus B. T-shaped with dilated horns
 B. Partial C. Arcuate Type V: Septate uterus: A. Complete (septum to internal os) B. Partial Type VI: Diethylstibestrol-related anomalies: A. T-shaped uterus B. T-shaped with dilated horns.")
25
INCIDENCE The incidence of congenital uterine anomalies is difficult to determine since many women with such anomalies are not diagnosed, especially if they are asymptomatic. Uterine anomalies occur in 2 to 4 percent of fertile women with normal reproductive outcomes. Dr Mars 2010

26
Frequency of specific anomalies
A review including a combined population of infertile and fertile women, the frequency of anomalies by type was: septate (35 percent), bicornuate (26 percent), arcuate (18 percent), unicornuate (10 percent), didelphys (8 percent), and agenesis (3 percent)
, bicornuate (26 percent), arcuate (18 percent), unicornuate (10 percent), didelphys (8 percent), and agenesis (3 percent)")
27
DEVELOPMENTAL DEFECTS
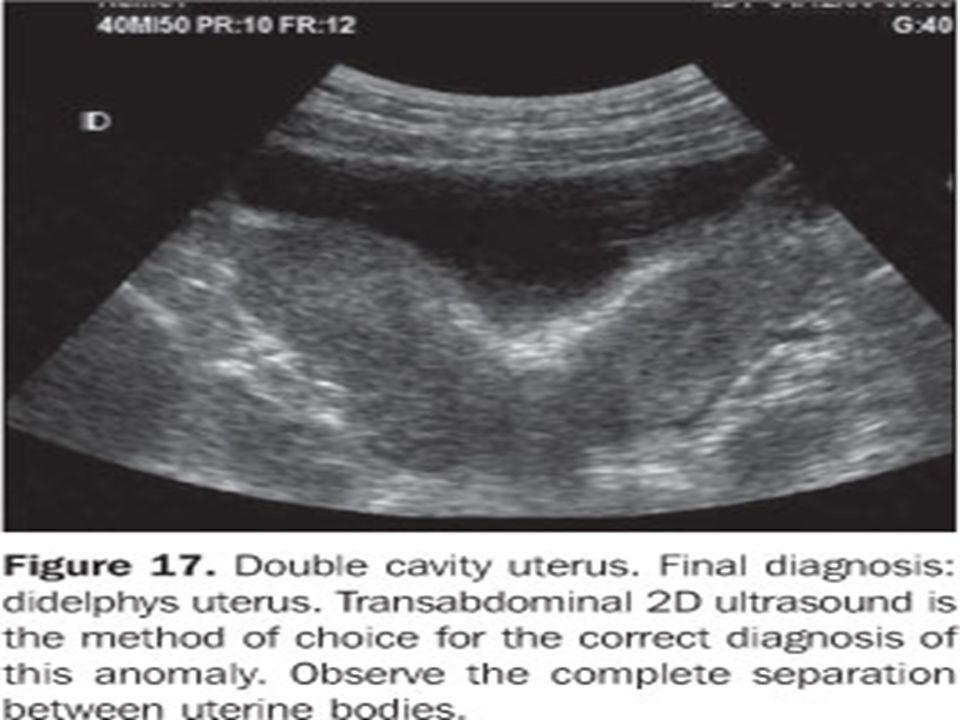
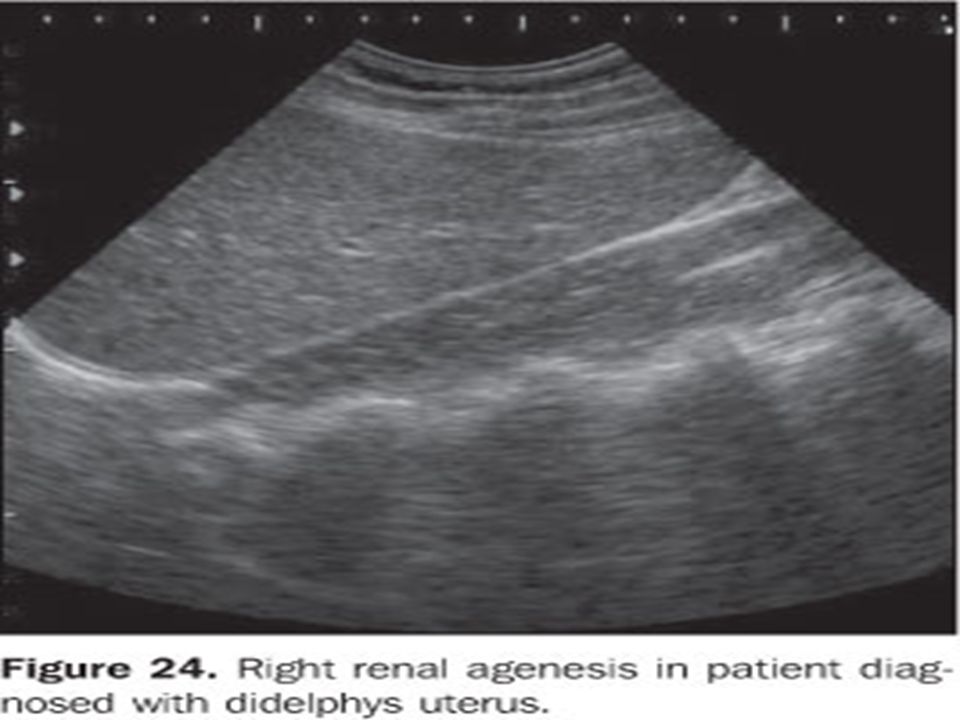
There are three common developmental defects of the müllerian system to consider: Agenesis Lateral fusion defects Vertical fusion defects Uterine didelphys : Uterine didelphys, or double uterus, occurs when the two müllerian ducts fail to fuse, thus producing duplication of the reproductive structures. Associated renal anomalies : Renal anomalies are found in 20 to 30 percent of women with müllerian defects.

28
ETIOLOGY The underlying etiology of congenital müllerian defects is not well understood. The karyotype of women with these anomalies is usually normal (46,XX in 92 percent). Most of the defects are likely to be related to polygenic and multifactorial causes.
. Most of the defects are likely to be related to polygenic and multifactorial causes.")
29
CLINICAL MANIFESTATIONS
Adolescents may present with pelvic pain. Many anomalies in adults are discovered after hysterosalpingography during a work-up of infertility or reproductive loss.

30
Signs & symptoms The signs and symptoms associated with müllerian anomalies vary greatly, depending upon the defect involved. Adolescents may have increased pelvic pain (either cyclic or noncyclic), dysmenorrhea, abnormal vaginal bleeding, or vaginal pain. amenorrhea Longitudinal vaginal septum may occur alone, but is usually seen with didelphic or other forms of double uterus. A vaginal septum may lead to dyspareunia If one side of the vagina is obstructed, complications such a hydrocolpos and hematocolpos may occur and a mass may be detected on bimanual examination. In addition, microperforations into the obstructed vagina can lead to infection.
, dysmenorrhea, abnormal vaginal bleeding, or vaginal pain. amenorrhea. Longitudinal vaginal septum may occur alone, but is usually seen with didelphic or other forms of double uterus. A vaginal septum may lead to dyspareunia. If one side of the vagina is obstructed, complications such a hydrocolpos and hematocolpos may occur and a mass may be detected on bimanual examination. In addition, microperforations into the obstructed vagina can lead to infection.")
31
OBSTETRICAL COMPLICATIONS
Recurrent pregnancy loss Preterm delivery Malpresentation Uterine rupture

32
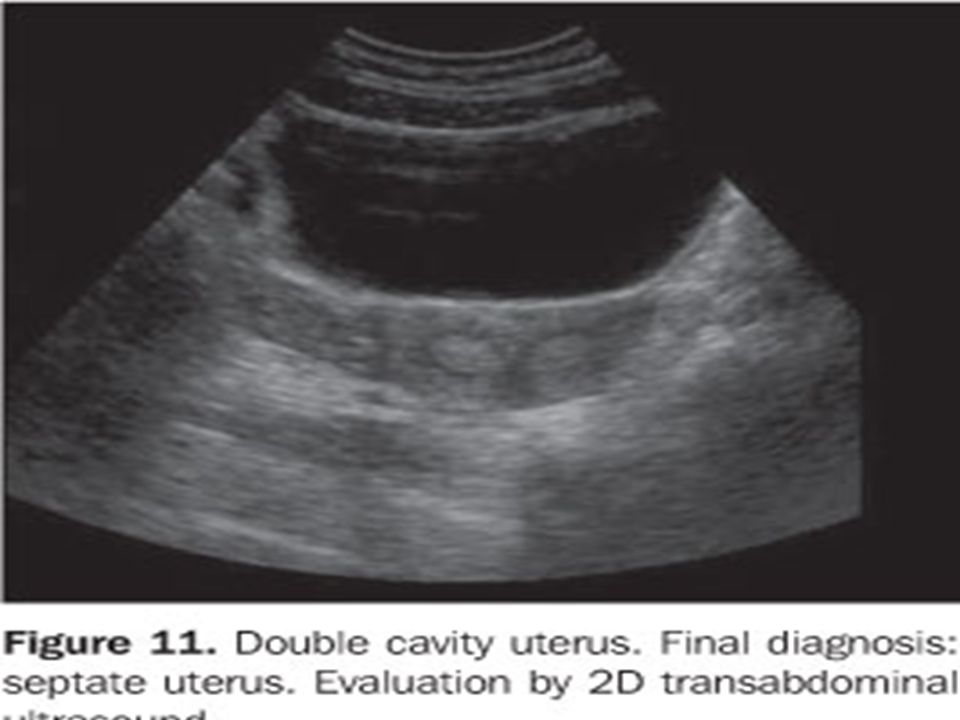
DIAGNOSIS A diagnosis of a structural uterine abnormality may be defined at hysterosalpingography during an infertility evaluation or by ultrasonography for an evaluation of pelvic pain or a mass, additional studies are often required for definitive diagnosis. Traditionally, magnetic resonance imaging (MRI) has been considered the "gold standard" for diagnosing anomalies of the reproductive tract. Hysterosalpingogram Sonohysterography 3-D ultrasound In cases of complicated müllerian anomalies, additional information may also be obtained by examination with the patient under anesthesia, vaginoscopy, laparoscopy, and/or hysteroscopy. However, these procedures are required less frequently because of the radiologic advances described above.
 has been considered the gold standard for diagnosing anomalies of the reproductive tract. Hysterosalpingogram. Sonohysterography. 3-D ultrasound. In cases of complicated müllerian anomalies, additional information may also be obtained by examination with the patient under anesthesia, vaginoscopy, laparoscopy, and/or hysteroscopy. However, these procedures are required less frequently because of the radiologic advances described above.")
33
Longitudinal vaginal septum :
Treatment Longitudinal vaginal septum : Longitudinal septa are typically associated with uterine anomalies, such as septate uterus and uterus didelphys. Treatment:Treatment involves complete removal of the septum. Excision is the traditional procedure with care to avoid compromise to the bladder and rectum. The septal tissue should be excised in total as retained fragments of septum may cause dyspareunia. The septal tissue is resected and then the normal vaginal mucosas from each vagina are sutured together over the defect created by the resection. Surgery is not required in asymptomatic women with a longitudinal vaginal septum, but will facilitate vaginal delivery. Dr jerii 2007

34
Obstructed hemi-vagina :
Treatment Obstructed hemi-vagina : An obstructed hemi-vagina is usually associated with ipsilateral renal agenesis. Treatment: Women with an obstructed hemi-vagina require surgical correction due to pain, increased risk of infection, and retrograde menses. The obstructed vagina is entered, the fluid is drained, and then the vaginal tissue between the two vaginas is resected. Great care is taken to avoid the bladder, rectum and the cervixes. some surgeons prefer to drain the obstructed vagina by the creation of a "window" with a second operation performed at a later time after the inflammation and distention have resolved.

35
Treatment of Imperforate hymen:
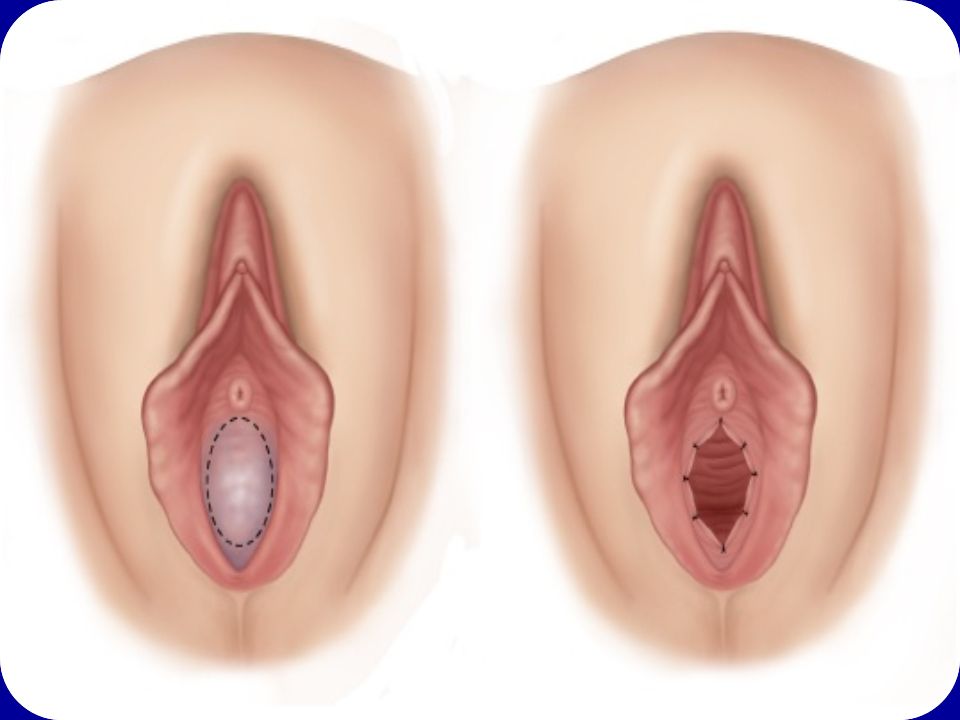
Repair of the hymen can be performed at any age; however, the repair is facilitated if the tissues have undergone estrogen stimulation. Therefore, surgery is ideal in the newborn, postpubertal, or premenarchal time periods. Surgical repair, performed under anesthesia, consists of an elliptical incision in the membrane close to the hymenal ring (figure 4) followed by evacuation of the obstructed material. Extra-hymenal tissue is excised using electrocautery to create a normal sized orifice and the vaginal mucosa is sutured to the hymenal ring using 3-0 or 4-0 vicryl or chromic suture to prevent adhesion and recurrence of the obstruction. Dr David 2005,Dr Dan 2007,Dr Valen 2008
 followed by evacuation of the obstructed material. Extra-hymenal tissue is excised using electrocautery to create a normal sized orifice and the vaginal mucosa is sutured to the hymenal ring using 3-0 or 4-0 vicryl or chromic suture to prevent adhesion and recurrence of the obstruction. Dr David 2005,Dr Dan 2007,Dr Valen")
37
Treatment of Transverse vaginal septum:
A small septum can be resected, followed by an end-to-end anastomosis of the upper and lower vaginal mucosa. A thick septum is more difficult to excise and repair; excision should be attempted only by surgeons experienced with this procedure. Reanastomosis is easier if the upper vagina has been distended with menstrual blood products, as this acts as a natural tissue expander to increase the amount of upper vaginal tissue available for the reanastomosis. In addition, preoperative use of vaginal dilators may thin the septum and facilitate reanastomosis. A Z-plasty technique can be used to prevent circumferential scar formation.

41
Thanks

Similar presentations





 as PID is an infection that affects a woman’s reproductive.>")
(6)(7)>")




 is a process by which egg cells are manually fertilized by sperm outside of the womb. IVF is a major treatment.>")

>")






>")