Download presentation
Presentation is loading. Please wait.

1
House of Care Making the space for a better conversation for people with long term conditions
Sue Roberts Chair, Year of Care Partnerships ‘Talking – differently health coaching for behaviour change and patient centred care’ Event East of England: November 11th 2014’ You've heard form Angela about the principles of what needs to be done to support people with LTCs and some of the benefits for everyone. She has introduced the House of care its main components and how it can be used to local to support the transformational change needed. She has described care and support planning as being at the centre. What I want to do is translate those key ideas into the nuts and bolts that clinical teams and health care communities need to use to get this into routine practice.

2
Setting the scene Who’s here? Wave if……
You work with someone on tasks / solutions (short periods) You work with people with LTCs in routine planned care You manage staff You help ensure the environment is right You plan training You work in the community / outpatients You work in general practice You work in acute settings
 You work with people with LTCs in routine planned care. You manage staff. You help ensure the environment is right. You plan training. You work in the community / outpatients. You work in general practice. You work in acute settings.")
3
Health Coaching - talking differently
Mindsets Skills The context / environment ?

4
The House of Care Making space for the conversation Health Coaching and planned care for people with long term conditions Making it easier to do the right thing

5
Guardian, 4th Jan 2014

6
Making it personal for everyone!
The Challenge! 15 million people Making it personal for everyone! 3 people 3 different needs – how ill we cope with providing a personalised response to all 15 million people with LTCs I believe that the approach to care and support planning I'm going to describe will go along way to doing this . BY providing a systematic approach which paradoxically end sup with unique personalised approach for each individual.

7
The individual's perspective
I start with the individuals perspective. This diagram which was drawn on a paper table cloth by people with LTCs at a workshop. The green wavy line shows the ups and downs of living with a LTC like diabetes. The orange vertical bars indicate the contact with the health services which occurs at regular intervals , for a relatively short period of time in the life of the individual and bears no relation ship to their particular needs in the intervening period. The delivery system offers an approach that addresses both components making better use of NHS contact time and helping CCGs to ensure that the right support is available in the right place at the right time for the characteristics of each community.

8
Making better use of NHS contact time ……..Care and support planning
More meaningful conversations about Support for self management to live good lives Disease surveillance Care provision Linking and coordinating with social care and community activities I start with the individuals perspective. This diagram which was drawn on a paper table cloth by people with LTCs at a workshop. The green wavy line shows the ups and downs of living with a LTC like diabetes. The orange vertical bars indicate the contact with the health services which occurs at regular intervals , for a relatively short period of time in the life of the individual and bears no relation ship to their particular needs in the intervening period. The delivery system offers an approach that addresses both components making better use of NHS contact time and helping CCGs to ensure that the right support is available in the right place at the right time for the characteristics of each community.

9
Care Planning in the beginning
Person’s story Professional story Information gathering Information sharing Builds on current skills Care planning is about taking a systematic approach to that conversation – something that medics here will be familiar with; in this case starting with information gathering , sharing and unpacking and then through a process of discussion and debate identifying the person’s own goals and action plans as well as any clinical work and then recording this. What makes it different from a usual clinical consultation is not just the mutual goal setting and action planning but what goes on up here. To enable this to be a true meeting between experts the consultation needs to be prepared for properly; a way must be found not just to identify the professional story, the usual tests and information in the clinical record but the persons story , what life’s like and how its different since the mother in law with dementia came to stay. The YOC care pilot sites realized that it was not just what when on in the consultation that was important – but what went on around this to make it possible. Goal setting and action planning Agreed & shared ‘care plan’ Year of Care

10
Disease Surveillance Preparation Care Planning
Information gathering Disease Surveillance Health Care Assistant performs ‘annual review’ tests 1st visit Information sharing Preparation Results/agenda setting prompts sent to patient > 1 week before consultation; Between visits Care Planning “ a meeting of equals and experts” Prepared HCP and patient meet to review how things are going consider what's important share ideas discuss options and develop a Care plan Consultation and joint decision making 2nd visit Agreed and shared goals and actions (care plan)
")
11
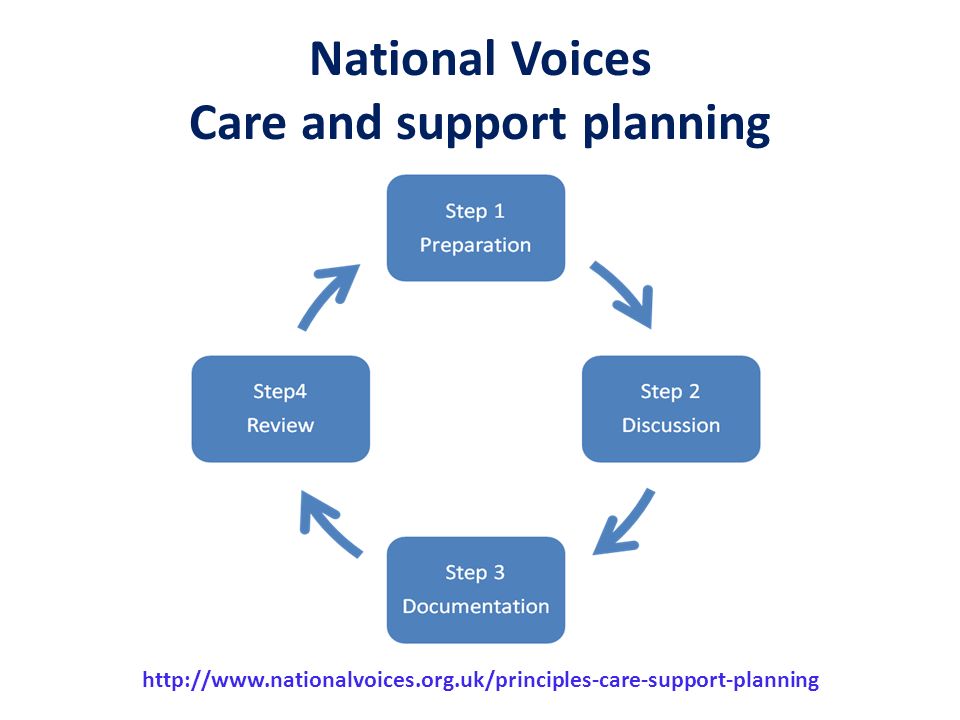
National Voices Care and support planning
12
Being prepared I am more in control. I have the …information so I am not so reliant on the system. I can share the information with my own family and use it to encourage them to be more healthy. (Bengali Patient TH) I got more information out of it than …..previously. …they were probably giving us the information,(but) they were giving it us in a different way. [PWD12] ‘Its actually more rewarding. We spend more time engaging with patients....rather than ticking boxes’ (Nurse practitioner) These key differences were identified systematically in the pilot sites of the yOCP 5 years ago . Three very different primary acre sites identified what they wanted to do by realised that particular involving there person perspective was very different in the way that things were organised in diabetes which provided an exemplar. They realised that the organisation of how care was delivered was getting in the way of working with people with long term conditions They worked collaboratively with patient groups and came up with a new way of working which in diabetes looked like In particular they had to work hard to ensue that the person point of view was unearthed and included. For instance by sharing est. results or prompts before hand. They also separated out all the test and tasks that professionals want to do – and are really important form there conversation. This is what they came up with. A two visit approach with time for reflection built in. Despite the work to organise this it was popular. Information gathering – the individual comes to an initial appointment and has all of the important biometric tests and tasks perfumed – including any assessments – this is all done at a single appointment which has 2 advantages – the individual can have their results before the care planning consultation and during the consultation their aren't any distractions from performing tests and needing to look for information Information sharing – this information is then sent to the individual ahead of the care and support planning appointment and they have some time to digests, share and think about what they want to discuss In addition an agenda setting prompt invites them to consider the non medical issues that they might want to think about They are also clear about the purpose of the appointment and how long they have ! Care Planning The time is now free to plan and work together and enable the better conversations that we have been talking about The sites that had worked this all out for diabetes soon realised that this approach was ideal for other single and multiple LTCs. The Training team began to work with other groups including multidisciplinary teams working with term frailest people – and tested the approach with the Personal health Budget sites as you saw previously. So it became possible to pull out the generic component of care and support planning that would apply to anyone with LTCs or disability. National voices have been carrying out a consultation on this which Laura will describe I will now go over the details of what this will mean in practice for the professional partner and also for the person - this meeting between experts,. … Absolutely 100% better ……for me and for the patients.[GP} Year of Care 12 12 12
 I got more information out of it than …..previously. …they were probably giving us the information,(but) they were giving it us in a different way. [PWD12] ‘Its actually more rewarding. We spend more time engaging with patients....rather than ticking boxes’ (Nurse practitioner) These key differences were identified systematically in the pilot sites of the yOCP 5 years ago . Three very different primary acre sites identified what they wanted to do by realised that particular involving there person perspective was very different in the way that things were organised in diabetes which provided an exemplar. They realised that the organisation of how care was delivered was getting in the way of working with people with long term conditions. They worked collaboratively with patient groups and came up with a new way of working which in diabetes looked like. In particular they had to work hard to ensue that the person point of view was unearthed and included. For instance by sharing est. results or prompts before hand. They also separated out all the test and tasks that professionals want to do – and are really important form there conversation. This is what they came up with. A two visit approach with time for reflection built in. Despite the work to organise this it was popular. Information gathering – the individual comes to an initial appointment and has all of the important biometric tests and tasks perfumed – including any assessments – this is all done at a single appointment which has 2 advantages – the individual can have their results before the care planning consultation and during the consultation their aren t any distractions from performing tests and needing to look for information. Information sharing – this information is then sent to the individual ahead of the care and support planning appointment and they have some time to digests, share and think about what they want to discuss. In addition an agenda setting prompt invites them to consider the non medical issues that they might want to think about. They are also clear about the purpose of the appointment and how long they have ! Care Planning. The time is now free to plan and work together and enable the better conversations that we have been talking about. The sites that had worked this all out for diabetes soon realised that this approach was ideal for other single and multiple LTCs. The Training team began to work with other groups including multidisciplinary teams working with term frailest people – and tested the approach with the Personal health Budget sites as you saw previously. So it became possible to pull out the generic component of care and support planning that would apply to anyone with LTCs or disability. National voices have been carrying out a consultation on this which Laura will describe. I will now go over the details of what this will mean in practice for the professional partner and also for the person - this meeting between experts,. … Absolutely 100% better. ……for me and for the patients.[GP} Year of Care")
13
Organisational processes
Angela Coulter 28/11/12 Test results / agenda setting prompts: beforehand Contact numbers and safety netting IT: clinical record of care planning Know your population Organisational processes informed ‘patient’ Engaged, HCP committed to partnership working Prepared for consultation Information / education Emotional and psychological support Consultation skills / attitudes Integrated, multi-disciplinary team and expertise Senior buy-in and local champions The first group are the things that support and enable patients to be truly engaged and involved into the care planning process. I've talked about preparation for the consultation. Other things on the list might be structured education and emotional and psychological support. In some communities this might best be provided by faith or community groups. The second group are HCPs committed to partnership working; that develop the new consultation skills and really embrace the assets and contribution each person brings with them. It also includes partnership working with colleagues in practice and wider multidisciplinary teams and the importance of clinical champions to promote this new way of working. But it also needs attention to the infrastructure of care, the new organisational process to make it happen; sending out prompts and agenda setting material, identifying who to work with first, developing named contacts, and adapting the IT system to this way of working. Since all of this has work force, training and support implications commissioning is the foundation. So here is the care planning house – with the relationship between individual and professional at the centre and a check list of what needs to be in place. But it is critically also a metaphor. One wall of house is no good by itself; both walls need to be in place if it is to be fit purpose. A leaky roof is no good and the foundation must be secure. While every community will want to build their own house to reflect their own community, be it barn, bungalow or mansion they must all have walls, roof and foundations; and building a house involves bringing together the issues of attitudes, skills and infrastructure if the house is to stand the test of time. Commissioning - The foundation Commission care planning Quality assure and monitor Establish /publicise menu of community support Year of Care King's Fund annual conference 13

14
House Of Care A home for care planning
Flexible ‘plan’ for local tailoring Check list Metaphor Check list, metaphor and tweakable buildign lcoal house croft etc

15
Addressing attitudes, skills and infrastructure
Send test results/ agenda setting prompts Organisational processes informed patient Engaged, HCP committed to partnership working Prepared for consultation Consultation skills / attitudes Collaborative care planning consultation Addressing attitudes, skills and infrastructure Commissioning - The foundation Procured time for consultations, training, & IT

16
Benefits Improves patient experience Reported changes in behaviour
Suitable across diverse populations Clinical outcomes across a number of care planning cycles Improves job satisfaction Improves team work Cost neutral at practice level Better links with specialists

17
Year of Care Training and Support Team Reproducible intervention
International Evidence Base Reproducible intervention A generic approach So the YOC team began to work on how to spread this learning So although it started in diabetes it involves a set of key steps which seem common to all encounters for people it LTCs and we have been working with National voices to make this more access bale to both users and those who want to introduce this as a generic way of working you watch the generic approach to care and support planning in LTCs that we will be describing you need to know that There a robust evidence and experience base formed around a transferable and reproducible prototype - we know this works in England and this work is the basis of the quotes and examples we will describe . The Pilot sites in the Year of Care Programme took the evidence base and worked out what was needed to enable care and support planning to happen in real like – not as an add on project - using diabetes as an exemplar. The programme then developed a carefully crafted training and support programme which was tried and tested this for transferability to 12 other sites. Since the end of the formal evaluation The YOC care have worked or are working with many other teams round the country Including continuing healthcare teams who want to use care and support planning to introduce personal Health budgets. All the time the learning has increased – and the team now know what works and what doesn’t – at least 3000 practitioners have been trained via cascade training from 40 or so quality assured trainers. In this process and more latterly working with National Voices to describe the key components the core elements of what care and support planning is about have been developed so we know the principles works for other single conditions like COPD, for health checks and for the group which is the current focus of LTCs policy - the most frail and vulnerable. There is a strong international evidence base More importantly this has been taken and tested for feasibility in every day clinical practice in England - so what I’m going to show you works. And it is reproducible Points – build on best international evidence of what should work Put together in grass roots primary care in England i.e. tried and tested in English settings red dots Training programme refined in 12 further sites / and quality assured training eh trainers programme developed : yellow Recently transferred using cascade training to a total of 26 sites – and more if include PHB training (White); green (includes waiting) Over 3000 practitioner and 50 trainers Now developed for other conditions beyond diabetes including COPD , health checks and those with multiply morbidity in a variety of settings . >4000 practitioners and 60 quality assured trainers
; green (includes waiting) Over 3000 practitioner and 50 trainers. Now developed for other conditions beyond diabetes including COPD , health checks and those with multiply morbidity in a variety of settings . >4000 practitioners and 60 quality assured trainers.")
18
Beyond diabetes...

19
Diabetes care plan COPD care plan Arthritis care plan Depression care plan

20
Your care plan

21
Holmside Medical Group
One care planning conversation, including all conditions → one care plan Achieved for all 30% on QOF registers ‘It’s what we do now – we would never go back’

22
Elderly, multi morbidity, frailty
……I'm listened to …….you may not have all the answers …….you’ve helped me work things out

23
If you would like to find out more

24
‘Surveying your House of Care’

25
Organisational processes
informed patient Engaged, HCP committed to partnership working Collaborative care planning consultation

26
Surveying your House Going well? What needs to be embedded?
Not so well/missing ? What could you change? What might you need help with?

27
Involving people in their care
Organisational processes informed patient Engaged, HCP committed to partnership working Involving people in their care Commissioning - The foundation

28
Involving people in their care
IT: clinical record of care planning Send test results/ agenda setting prompts Organisational processes Know your Population informed patient Engaged, HCP committed to partnership working ‘Prepared’ for consultation Consultation skills / attitudes Involving people in their care Information/ Structured education Integrated, multi-disciplinary team & expertise Senior buy-in & local champions to support & role model Emotional & psychological support Commissioning - The foundation Identify and fulfil needs Procured time for consultations, training, & IT Quality assure and measure

29
If you would like to find out more

32
Holmside in Newcastle A whole team approach 9000, inner city, two sites
Practice initiated YOC: Care and support planning training Facilitated ‘time in’– getting the whole practice on board Redesigned the systems – admin/HCA key Continuous in house training – building generic skills Implemented a four step approach Information gathering (+/- sharing) separate from Care planning consultation Achieved for all 30% on QOF registers ‘It’s what we do now – we would never go back’
 separate from. Care planning consultation. Achieved for all 30% on QOF registers. ‘It’s what we do now – we would never go back’")
33
What needs to be in place to ensure that ?
People with LTCs are prepared for their care planning consultations / better conversations , are involved in decision making and are supported to self manage ? Health Care Professionals are prepared for a care planning consultation / better conversations and work in partnership with people with long term conditions?

34
Elderly, multi morbidity, frailty
Identification of Individual Prepared ‘person’ Prepared professional Care and Support Planning Conversation ……I'm listened to …….you may not have all the answers …….you’ve helped me work things out

35
Organisational processes
IT: clinical record of care planning Send test results/ agenda setting prompts Organisational processes Know your Population informed patient Engaged, HCP committed to partnership working ‘Prepared’ for consultation Consultation skills / attitudes Collaborative care planning consultation Information/ Structured education Integrated, multi-disciplinary team & expertise Senior buy-in & local champions to support & role model Emotional & psychological support Commissioning - The foundation Identify and fulfil needs Procured time for consultations, training, & IT Quality assure and measure

36
Surveying your House Going well? What needs to be embedded?
Not so well/missing ? How would you know if it was working? How much clinical engagement is there for working differently?

Similar presentations


 Pilot population.>")


















