Download presentation
Presentation is loading. Please wait.

1
Common Dermatologic Conditions
Toby Maurer, MD University of California, San Francisco

3
Acne Papulopustular Cystic, scarring, keloidal Topicals okay
p.o. antibiotics Accutane

4
Topicals BP 5% gel (10% - more drying)
Retin A 0.025% - 0.1% ( vehicle determines strength - start with crème) Cleocin T or erythromycin topically Use 1 qam and 1qhs If NO success after 8 weeks, go to p.o.’s
 Cleocin T or erythromycin topically. Use 1 qam and 1qhs. If NO success after 8 weeks, go to p.o.’s.")
7
P.O. Antibiotics TCN - 500 bid x 8 weeks
Doxycycline bid x 8 weeks Minocycline bid x 8 weeks Taper - Do NOT STOP ABRUPTLY

8
Alternatives Erythromycin - 500 bid Septra - check WBC’s
Keflex-500 tid

9
Spiranolactone Diuretic used in cirrhosis of liver
Also an anti-androgen Useful in females who have cysts around menstruation mg qday continuously Increased urination, don’t use during pregnancy, ?electrolyte imbalance

11
Accutane Document failure of antibiotics
Baseline CBC, LFT’s ,TG and cholesterol Two forms of birth control, negative pregnancy tests MD’s will need to be registered as will patients Counseling on depression

13
Acne Rosacea Common in women over 40
Often seen in persons of Irish decent Associated with seborrheic dermatitis Characterized by papules, erythema, telangiectasia and rhinophyma (M>F) Sun exposure, alcohol and spicy foods exacerbate rosacea
 Sun exposure, alcohol and spicy foods exacerbate rosacea.")
14
Acne Rosacea Oral antibiotics for 6-8 weeks clears skin for some amount of time Topicals work less frequently

16
Perioral Dermatitis TREATMENT Topicals: Cleocin T Gel bid
Erythromycin bid p.o. antibiotics –TCN Doxycycline Minocycline - bid x 8 wks Keeps pts in remission x 2 yrs.

18
Hair Loss Decide if scarring or not: If scarring-refer
If not scarring and diffuse: Check recent surgeries/illness, nutrition, anemia, TSH, estrogen replacement, medication history, VDRL. If hirsute with scalp hair loss-DHEAS and free testosterone If lactating- check prolactin

20
If all negative Androgenetic Alopecia-
Minoxidil 5% bid topically (even in women) Can make hair oily-may want to start with minoxidil 2% or use 2% by day and 5% at night Use for at least 6 months for results and what you see after 1 yr. is the effect you can expect. What about finasteride (propecia)?-equal to minoxidil in men. Does not work in women.
 Can make hair oily-may want to start with minoxidil 2% or use 2% by day and 5% at night. Use for at least 6 months for results and what you see after 1 yr. is the effect you can expect. What about finasteride (propecia) -equal to minoxidil in men. Does not work in women.")
21
Too Much Hair Vaniqa topical cream that breaks the chemical bond of hair apply 2x’s/day forever 30% effective $30/month

22
Hair Removal pigment of hair absorbs the light and is destroyed
dark hair responds hair is always in different growth phases, so treatment has to be repeated several times to catch the phase(expensive) Side effects: pigment changes of surrounding skin and scarring
 Side effects: pigment changes of surrounding skin and scarring.")
24
Psoriasis-What is it? Fast growing skin-takes 3 days to come to surface and desquamate Normal rate is 28 days Psoriatic skin has a fast mitotic rate Triggers an inflammatory response in and around affected skin

25
New onset often preceded by strep infection (strep pharyngitis) especially in the younger age group.
In older age group, drugs often unmask psoriasis Drugs: beta-blockers, lithium, NSAIDS, antimalarials, terbinafine, gemfibrozil-pts on these meds for 3-6 months before onset of psoriasis

29
Psoriasis-Tx: Decrease the mitotic rate of skin
Tar (LCD 5% in TAC 0.1% oint) ( Tar emulsions), topical retinoids (Tazarac) Decrease the inflammatory response of the skin Steroid Ointment (mid-potency-1st line) Calcipotriene (Dovonex Ointment)-not on face or groin Clobetasol/Dovonex combination Ultraviolet light (psoralen+ UVA), UVB NO PREDNISONE
 ( Tar emulsions), topical retinoids (Tazarac) Decrease the inflammatory response of the skin. Steroid Ointment (mid-potency-1st line) Calcipotriene (Dovonex Ointment)-not on face or groin. Clobetasol/Dovonex combination. Ultraviolet light (psoralen+ UVA), UVB. NO PREDNISONE.")
30
NEXT STEP Time for referral
Methotrexate-liver biopsies necessary(don’t give in HEP C pts) Oral retinoids (Acetretin)-not in persons of reproductive potential -? Okay in liver disease; excellent drug in HIV Cyclosporine Biologics (Enbrel, Remicade)-most benefit in psoriatic arthritis and quick reversal of pustular psoriasis
 Oral retinoids (Acetretin)-not in persons of reproductive potential - Okay in liver disease; excellent drug in HIV. Cyclosporine. Biologics (Enbrel, Remicade)-most benefit in psoriatic arthritis and quick reversal of pustular psoriasis.")
31
Eczema Dry, inflamed skin that becomes “weepy”
Not bilateral and symmetric No thick scale No scalp/nail involvement Topical steroids first line of treatment Oral cyclosporine was known to turn off inflammation Now: topical formulation of Cyclosporine

33
Eczema Tacrolimus (Protopic) and Pimecrolimus (Elidel), new kids on the block Great for facial eczema $120 for 30gm

34
Topical Immune Modulators and Cancer
Elidel (pimecrolimus 1%) and Protopic (tacrolimus 0.1% and 0.03%) –heavily marketed 29 cases of cancers in children and adults associated with use of these topicals-lymphomas, SCC’s, sarcomas Causality not proven
 and Protopic (tacrolimus 0.1% and 0.03%) –heavily marketed. 29 cases of cancers in children and adults associated with use of these topicals-lymphomas, SCC’s, sarcomas. Causality not proven.")
35
FDA Response Black Box Warning
Do not use in children under 2 years of age Do not us in adults or children with “weakened” immune systems: Transplants, HIV, cancer patients, etc. Limit use—no continuous usage; limit area treated

37
Topical Immunomodulators When to use
Eyelid dermatitis Refractory psoriasis on upper thighs, scrotum, glans penis Otherwise use cheaper alternatives first Protopic=TAC 0.1% Elidel=HC 2.5%

39
Buttock Folliculitis Mechanical from clothing Ban roll-on good
Topical antibx qd Cleocin/Erythro

41
Keratosis Pilaris Thickening of hair follicles on the out arms and upper legs Associated with dry skin Lubrication Lachydrin 12% lotion bid

43
Intertrigo Pendulous breasts or pannus Always component of candida
Blow dry area Apply topical antifungals Tucks pads

48
Bacterial Skin Infections
Most common pathogen is staph aureus More methicillin resistant staph causing skin and soft tissue infections in the community JAMA-Niami et al Dec 2003

49
Approach to Treatment Culture where you can-if you have pus, that is great Incise and drain when appropriate (Abcesses)
 .")
50
If no pus: Tx with methicillin SENSITIVE drugs-first line but have pt return to evaluate for resolution If recurrent infection, tx with methicillin RESISTANT antibiotics right off the bat Septra, Doxycycline,Cipro/Levofloxacillin), Clindamycin Consider adding rifampin 600 qd for 5 days or mupirocin ointment for staph eradication
, Clindamycin. Consider adding rifampin 600 qd for 5 days or mupirocin ointment for staph eradication.")
52
Was it bacterial in the first place?
Remember HSV-culture and/or Direct Fleurescent Antibody Skin biopsy for histology and tissue culture Diseases that Masquerade as Infectious Diseases Ann Int Med 2005 Jan 4; 142:47-55

55
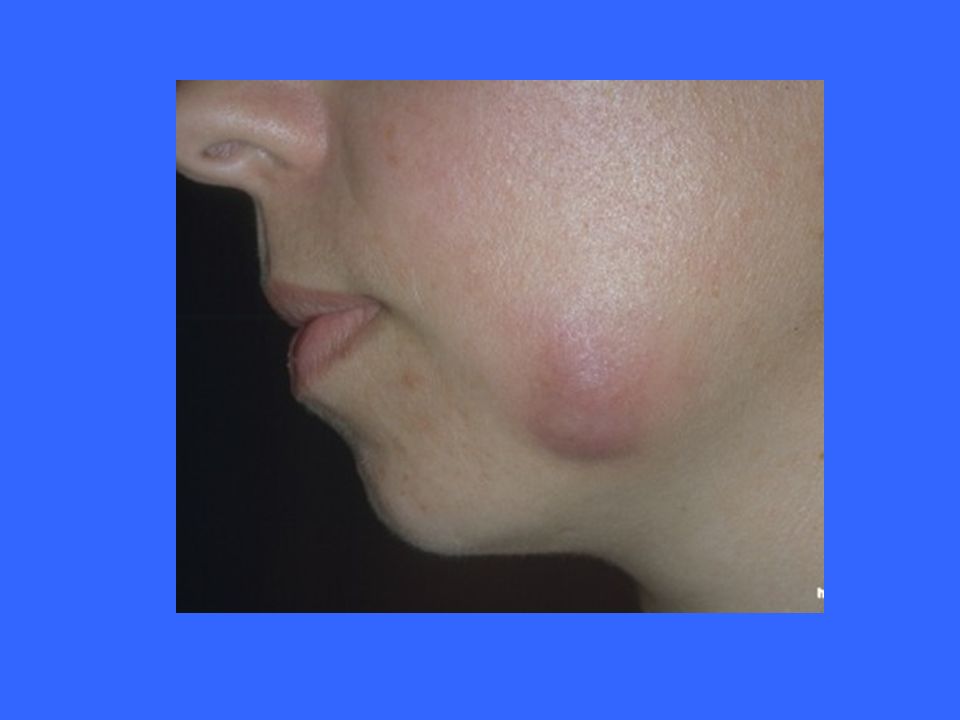
Hidradenitis Supparativa
Not an infectious disease Disease of apocrine glands Treatment IL Kenalog Minocycline Surgery NOT Antibiotics New Biologics

57
Inflamed Epidermoid Cysts
Antibiotics-USELESS If just starting to become inflamed and cyst is small( < 1 cm), can try intralesional Kenalog injection but see them back in few days-you can exacerbate the inflammation INCISE and DRAIN and PACK 6 weeks later, inspect for residual cyst and excise
, can try intralesional Kenalog injection but see them back in few days-you can exacerbate the inflammation. INCISE and DRAIN and PACK. 6 weeks later, inspect for residual cyst and excise.")
60
Recurrent Cellulitis Recurrent cellulitis knocks out lymph system causing low grade cellulitis and retention hyperkeratosis Tx. Cellulitis-may need 6 months of tx or more Tx. Hyperkeratosis-urea crème 40% Tx. Lymphedema-support stockings with 35mm of pressure or mechanical pumps

63
Venous Insufficiency Ulcer
Compression dressing Unna boot covered by Coban – this requires a good nursing staff with training and experience This both provides graded compression AND creates the correct wound environment Semipermeable dressing (Hydrosorb, Duoderm, etc) Change dressing weekly Refer to dermatology if not healing
 Change dressing weekly. Refer to dermatology if not healing.")
64
Venous Insufficiency Ulcer
Control Edema Elevation of leg above heart 2 hours twice daily Walk, don’t sit Compression Diuretics overused and not of benefit unless fluid retention due to central problem is present (CHF, CRF) Create an appropriate wound environment for healing Paradigm shift: Ulcers that don’t heal do not have the appropriate biochemical environment to promote healing
 Create an appropriate wound environment for healing. Paradigm shift: Ulcers that don’t heal do not have the appropriate biochemical environment to promote healing.")
65
Complications of Leg Ulcers
Allergic contact dermatitis to applied antibiotics, topical anesthetics Avoid all topical antibiotics to leg ulcers (except topical metronidazole to prevent odor) Never apply topical benzocaine, Vitamin E, neomycin, or bacitracin to VI leg ulcer
 Never apply topical benzocaine, Vitamin E, neomycin, or bacitracin to VI leg ulcer.")
67
64 year old man with psoriasis, hypertension, hypercholesterolemia
3 months of ulceration of medial aspect of left lower leg Vascular evaluation confirms venous insufficiency

69
3 months of treatment fails to improve ulceration
What is your next step?

70
Skin Biopsy = Squamous Cell Carcinoma
Chronic phototherapy and prior immunosuppressive treatments may have led to skin cancer If leg ulcer doesn’t heal with appropriate treatment—refer or biopsy

Similar presentations









































,>")







