Download presentation
Presentation is loading. Please wait.

1
WelcomeWelcome

2
DVT Prophylaxis in Orthopaedic Surgery Symposium, American Academy of Orthopedic Surgeons, Annual Meeting, San Diego, California February 14, 2007

3
Javad Parvizi, MD, FRCS Associate Professor Department of Orthopedics Thomas Jefferson University Rothman Institute Philadelphia, PA Peter B. Hanson, MD Medical Director of Orthopedics Chief of Staff Grossmont Hospital La Mesa, CA Russell Hull, MBBS, MSc Professor of Medicine Director, Thrombosis Research Unit University of Calgary Calgary, Alberta Canada Program Faculty Eugene R Viscusi, MD Director, Acute Pain Management Associate Professor Department of Anesthesiology Thomas Jefferson University Philadelphia, PA Paul F. Lachiewicz, MD Department of Orthopaedics University of North Carolina School of Medicine Chapel Hill, NC

4
Financial Disclosures Javad Parvizi, MD, FRCS Grant/Research Support: NIH, OREF, DOD, Aircast, GSK, Ortho McNeill, Pfizer, Smith and Nephew, Stryker Consultant: Stryker Orthopaedics Speakers Bureau: Endo Peter B. Hanson, MD Speakers Bureau: Eisai, sanofi- aventis, Bristol-Myers Squibb Russell Hull, MBBS, MSc Grant/Research Support: sanofi- aventis, Bayer Consultant: sanofi-aventis, Wyeth, GSK, Leo Pharmaceuticals, Pfizer, Bayer Eugene R Viscusi, MD Research Support: Ortho-McNeil Pharmaceutical, Inc., Endo Pharmaceuticals, SkyePharma, Pfizer Inc, Xsira Pharmaceuticals, Baxter Pharmaceutical Products, Inc., and Progenics Pharmaceuticals, Inc. Consultant: Ortho-McNeil Pharmaceutical, Inc., Adolor Corporation, Endo and SkyePharma Speakers Bureau: Endo Paul F. Lachiewicz, MD Consultant: Zimmer, Endo Research Grant: Aircast

5
Educational Objectives Learn how to explain current guidelines issued by national professional organizations and colleges, such as the AAOS, ACCP, and ASA, mandating risk-directed prophylaxis against DVT in low-to-high risk patients undergoing orthopedic surgery. Learn how to explain current guidelines issued by national professional organizations and colleges, such as the AAOS, ACCP, and ASA, mandating risk-directed prophylaxis against DVT in low-to-high risk patients undergoing orthopedic surgery. Learn how to identify factors to risk stratify orthopedic surgery patients undergoing THA, TKA, fracture repair, to assess their likelihood for incurring DVT. Learn how to identify factors to risk stratify orthopedic surgery patients undergoing THA, TKA, fracture repair, to assess their likelihood for incurring DVT. Learn how to describe pharmacologic and/or intermittent compression devices as part of a multimodal prophylaxis strategy aimed at the incidence of DVT in the OS patient population. Learn how to describe pharmacologic and/or intermittent compression devices as part of a multimodal prophylaxis strategy aimed at the incidence of DVT in the OS patient population. Learn how to specify pharmacologic agents used for DVT prophylaxis based on an analysis of efficacy, safety, and pharmacoeconomic parameters. Learn how to specify pharmacologic agents used for DVT prophylaxis based on an analysis of efficacy, safety, and pharmacoeconomic parameters.

6
Learn to discuss the special anesthesiological needs of OS patients at risk for DVT, with a focus on timing of prophylaxis, transitioning agents, and duration of prophylaxis based on the surgical procedure. Learn to discuss the special anesthesiological needs of OS patients at risk for DVT, with a focus on timing of prophylaxis, transitioning agents, and duration of prophylaxis based on the surgical procedure. Describe how to risk stratify patients undergoing orthopedic surgery, and implement ACCP-mandated pharmacologic and non-pharmacologic measures aimed at DVT prophylaxis. Describe how to risk stratify patients undergoing orthopedic surgery, and implement ACCP-mandated pharmacologic and non-pharmacologic measures aimed at DVT prophylaxis. Learn how to apply landmark clinical trials focusing on DVT prevention in OS patients. Learn how to apply landmark clinical trials focusing on DVT prevention in OS patients. Educational Objectives

7
DVT Prophylaxis After TJA Importance Catastrophic cardiopulmonary problem Catastrophic cardiopulmonary problem Death

8
Orthopedic procedures are high risk Orthopedic procedures are high risk DVT Prophylaxis After TJA Importance

9
Learn current guidelines (ACCP, AAOS) Learn current guidelines (ACCP, AAOS) Stratify orthopedic surgery patients Stratify orthopedic surgery patients How to apply various modalities How to apply various modalities DVT Prophylaxis After TJA Objectives
 Learn current guidelines (ACCP, AAOS) Stratify orthopedic surgery patients Stratify orthopedic surgery patients How to apply various modalities How to apply various modalities DVT Prophylaxis After TJA Objectives")
10
Pharmacologic agents Pharmacologic agents l Unfractionated heparin l LMWH l Coumadin l Aspirin Mechanical Mechanical Multimodal Multimodal DVT Prophylaxis After TJA Objectives

11
Select pharmacologic agents based on efficacy, safety, pharmacoeconomic parameters Select pharmacologic agents based on efficacy, safety, pharmacoeconomic parameters Issues related to coadministration of anesthesia and DVT prophylaxis Issues related to coadministration of anesthesia and DVT prophylaxis DVT Prophylaxis After TJA Objectives

12
Four 20 minutes talk Four 20 minutes talk Discussion Discussion DVT Prophylaxis After TJA Format

13
Russell Hull MBBS, MSc Professor of Medicine, Director, Thrombosis Research Unit, University of Calgary Current guidelines (ACCP) Current guidelines (ACCP) Risk stratification Risk stratification DVT Prophylaxis After TJA First Talk
 Current guidelines (ACCP) Risk stratification Risk stratification DVT Prophylaxis After TJA First Talk")
14
Peter Hanson, MD Medical Director of Orthopedics, Chief of Staff Grossmont Hospital, La Mesa, CA Current controversies Current controversies Agent selection Agent selection Duration of prophylaxis Duration of prophylaxis DVT Prophylaxis After TJA Second Talk

15
Paul Lachiewicz MD Professor of Orthopedic Surgery, University of North Carolina School of Medicine, Chapel Hill, NC Multimodal approach Multimodal approach Evidence based Evidence based Clinical implications of prophylaxis Clinical implications of prophylaxis DVT Prophylaxis After TJA Third Talk

16
Eugene Viscusi MD Director of Acute Pain, Department of Anesthesia Thomas Jefferson University, Philadelphia, PA Challenges of coadministration of DVT prophylaxis and anesthesia Challenges of coadministration of DVT prophylaxis and anesthesia DVT Prophylaxis After TJA Final Talk

17
Applying The Science of DVT Prophylaxis to Orthopedic Surgery Javad Parvizi MD, FRCS Rothman Institute of Orthopedics, Thomas Jefferson University Philadelphia, PA

18
Pubmed; MesH heading DVT and THA Pubmed; MesH heading DVT and THA 29,714 articles DVT Prophylaxis After THA Literature

19
Historic1 - 2% Historic1 - 2% Current0.1 - 0.2% Current0.1 - 0.2% Fatal P.E. DVT Prophylaxis After THA Importance

20
In many cases the complication is preventable We (not the internists) are responsible for choosing and administering prophylaxis
 are responsible for choosing and administering prophylaxis")
21
What agent? What agent? How long How long Screening Screening DVT Prophylaxis After THA Introduction

22
Data Difficult to Interpret: Different methods of diagnosis Different methods of diagnosis l clinical - ultrasound l venography - scans Different endpoints Different endpoints l death - DVT proximal vs distal l clinical PE or DVT Different definitions of complications Different definitions of complications l bleeding: major, minor l post phlebitic syndrome DVT Prophylaxis After THA Introduction

23
DVT Prophylaxis After THA Prophylaxis: No Warwick, JBJS, Br, 1995 1162 THA 1162 THA No chemical prophylaxis No chemical prophylaxis Fatal PE 0.34% Fatal PE 0.34% Murray et al, JBJS Br, 1996 Meta-analysis Meta-analysis 130,000 THA 130,000 THA Reported fatal PE 0.1 - 0.2% Reported fatal PE 0.1 - 0.2%

24
Effective prophylaxis is necessary in these patients [THA, TKA]... NIH consensus panel, 1986 NIH consensus panel, 1986 European consensus conference 1992 European consensus conference 1992 DVT Prophylaxis After THA Prophylaxis: Yes
![Effective prophylaxis is necessary in these patients [THA, TKA]...](http://images.slideplayer.com/1/678021/slides/slide_24.jpg "NIH consensus panel, 1986 NIH consensus panel, 1986 European consensus conference 1992 European consensus conference 1992 DVT Prophylaxis After THA Prophylaxis: Yes.")
25
In 2007 in North America we are obligated to do something In 2007 in North America we are obligated to do something King obtains $1.5M settlement for husband and children in pulmonary embolism death September 14, 2004 | Massachusetts Lawyers Weekly: Verdicts & Settlements DVT Prophylaxis After THA

26
DVT Prophylaxis After THA Agents Available Unfractionated heparin Unfractionated heparin LMWH LMWH Aspirin Aspirin Mechanical prophylaxis Mechanical prophylaxis

27
DVT Prophylaxis After THA LMWH Advantages: Predictable dose response Predictable dose response Proven efficacy Proven efficacyDisadvantages: Bleeding complications Bleeding complications Injection required Injection required

28
DVT Prophylaxis After THA LMWH: Results LMWH BID LMWH BID 194 THA 194 THA DVT rate 5% DVT rate 5% 8 major bleeding episodes 8 major bleeding episodes Colwell et al, JBJS Am, 1994

29
DVT Prophylaxis After THA Warfarin vs. LMWH Prospective, randomized Prospective, randomized Venography endpoint Venography endpoint LMWH started 2 hrs postop LMWH started 2 hrs postop Proximal DVT 5% (LMWH) vs 8% (Warfarin), p = 0.19 Proximal DVT 5% (LMWH) vs 8% (Warfarin), p = 0.19 More bleeding in LMWH group (p=0.001) More bleeding in LMWH group (p=0.001) Francis, et al: JBJS (A), 1995
 vs 8% (Warfarin), p = 0.19 Proximal DVT 5% (LMWH) vs 8% (Warfarin), p = 0.19 More bleeding in LMWH group (p=0.001) More bleeding in LMWH group (p=0.001) Francis, et al: JBJS (A),")
30
DVT Prophylaxis After THA LMWH Randomized, double blind Randomized, double blind 1472 THA 1472 THA Dalteparin before or early after vs warfarin Dalteparin before or early after vs warfarin Venogram detected DVT Venogram detected DVT Symptomatic thrombi less frequent in preop dalteparin group (p<0.02) Symptomatic thrombi less frequent in preop dalteparin group (p<0.02) Increased bleeding at surgical site for preop dalteparin group Increased bleeding at surgical site for preop dalteparin group Modified regimen (postoperative) Modified regimen (postoperative) Hull R et al: Arch Intern Med. 2000

31
Bottom Line: Effective Effective 2nd most commonly used agent in N. America 2nd most commonly used agent in N. America Probably increased bleed risk esp. if given too early Probably increased bleed risk esp. if given too early DVT Prophylaxis After THA LMWH

32
Coumadin and LMWH equally effective at preventing DVT after THA Coumadin and LMWH equally effective at preventing DVT after THA A slightly higher bleeding rate with LMWH A slightly higher bleeding rate with LMWH Coumadin is harder to use (outpatient monitoring) Coumadin is harder to use (outpatient monitoring) DVT Prophylaxis After THA Results: Summary
 Coumadin is harder to use (outpatient monitoring) DVT Prophylaxis After THA Results: Summary")
33
DVT Prophylaxis After THA Preventative Measures Expeditious surgery Expeditious surgery Minimize time vessels kinked in surgery Minimize time vessels kinked in surgery Mobilize promptly Mobilize promptly Calf exercises in bed Calf exercises in bed Elastic stockings (?) Elastic stockings (?) Epidural anesthesia Epidural anesthesia Lemos, Clin. Orth. 1992

34
DVT Prophylaxis After THA Prophylaxis Options What is the best agent for prophylaxis?

35
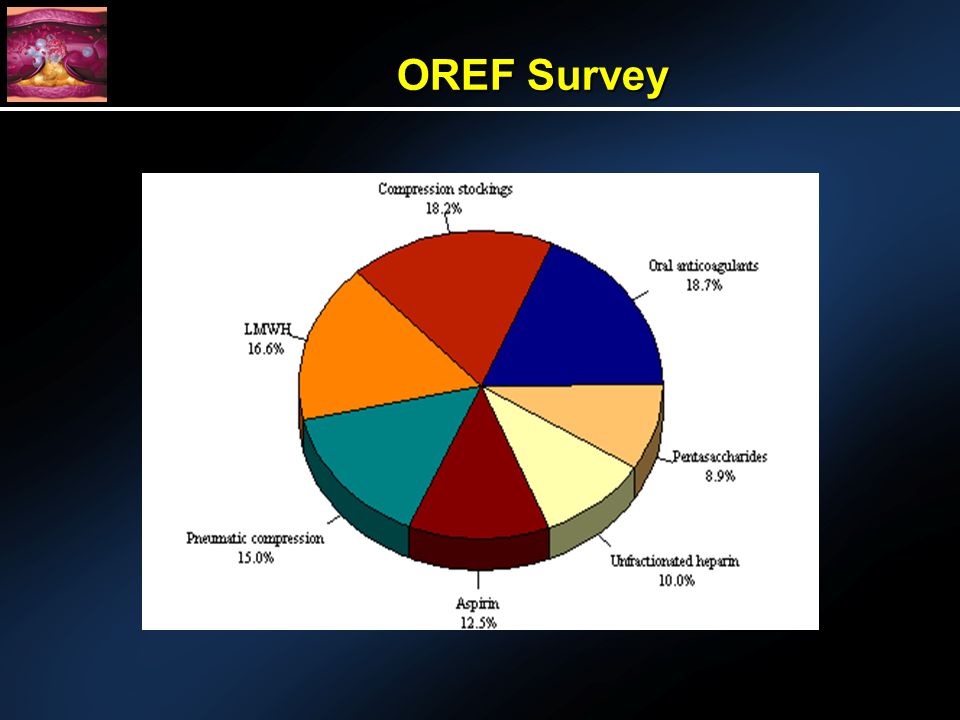
434 surgeons representing 48 states and three countries (Canada, Egypt, Pakistan) 434 surgeons representing 48 states and three countries (Canada, Egypt, Pakistan) Surgeons have been in practice an average of 19 years Surgeons have been in practice an average of 19 years >96% prophylax for DVT in their THA and TKA patients >96% prophylax for DVT in their THA and TKA patients OREF Survey
 434 surgeons representing 48 states and three countries (Canada, Egypt, Pakistan) Surgeons have been in practice an average of 19 years Surgeons have been in practice an average of 19 years >96% prophylax for DVT in their THA and TKA patients >96% prophylax for DVT in their THA and TKA patients OREF Survey")
37
DVT Prophylaxis After THA Which LMWH Certoparin (18 mg), dalteparin 30 mg, enoxaparin (24 mg) Certoparin (18 mg), dalteparin 30 mg, enoxaparin (24 mg) 188 patients undergoing TJA, or spine sx 188 patients undergoing TJA, or spine sx Changes in venous flow pre and postop doppler Changes in venous flow pre and postop doppler DVT= 1.1% DVT= 1.1% Bleeding = 11.2% (13 in certoparin, 4 in each) Bleeding = 11.2% (13 in certoparin, 4 in each) No difference in APTT, TCT, blood count No difference in APTT, TCT, blood count All as efficacious All as efficacious Janni W, et al.Zentralbl Chir. 2001

38
DVT Prophylaxis After THA Summary Proven efficacy Proven efficacy Works for you Works for you

39
DVT Prophylaxis After THA Duration of Prophylaxis How long should prophylaxis be continued after THA?

40
LMWH LMWH l Conflicting data Warfarin Warfarin l Amstutz: 15 days l Colwell: 7 days DVT Prophylaxis After THA Duration of Prophylaxis

41
DVT Prophylaxis After THA LMWH Randomized, double blind Randomized, double blind 569 THA 569 THA dalteparin vs warfarin in hospital and placebo out of hospital (35 days) dalteparin vs warfarin in hospital and placebo out of hospital (35 days) Venogram preop and postop Venogram preop and postop Proximal DVT significantly higher in warfarin/placebo group Proximal DVT significantly higher in warfarin/placebo group No major bleeding No major bleeding Hull R et al: Arch Intern Med. 2000

42
DVT Prophylaxis After THA Duration of Prophylaxis Markov-based decision analysis Markov-based decision analysis Outcome measures: PE prevented, hemorrhages induced, overall cost, overall cost for each PE prevented Outcome measures: PE prevented, hemorrhages induced, overall cost, overall cost for each PE prevented Agents: LMWH, warfarin, ASA, nothing Agents: LMWH, warfarin, ASA, nothing Extending to 4 weeks was safe for all agents Extending to 4 weeks was safe for all agents LMWH-most effective LMWH-most effective ASA-most cost effective ASA-most cost effective Conclusion: Safe to extend the prophylaxis to 4 but NOT 6 weeks Conclusion: Safe to extend the prophylaxis to 4 but NOT 6 weeks Sarasin FP, Bounameaux H.Thromb Haemost 2002

43
Patients with no specific risk factors (1-3 weeks) Patients with no specific risk factors (1-3 weeks) Patients with specific risk factor (6 weeks) (like previous DVT) Patients with specific risk factor (6 weeks) (like previous DVT) DVT Prophylaxis After THA Duration of Prophylaxis
 Patients with no specific risk factors (1-3 weeks) Patients with specific risk factor (6 weeks) (like previous DVT) Patients with specific risk factor (6 weeks) (like previous DVT) DVT Prophylaxis After THA Duration of Prophylaxis")
44
DVT Prophylaxis After THA Screening Do patients need routine screening for DVT after THA? Do patients need routine screening for DVT after THA?

45
Advantages: Identify and treat clots Identify and treat clotsDisadvantages: Accuracy of tests varies Accuracy of tests varies Problem of treating asymptomatic clots Problem of treating asymptomatic clots Unproven advantage Unproven advantage Cost Cost DVT Prophylaxis After THA Screening

46
A large prospective randomized trial comparing discharge ultrasound with sham ultrasound showed NO advantage to screening A large prospective randomized trial comparing discharge ultrasound with sham ultrasound showed NO advantage to screening DVT Prophylaxis After THA Screening Robinson, KS et al. Ann Intern Med. 1997 Sep 15;127(6):439-45
:")
47
Good judgment comes from experience and experience comes from bad judgment Good judgment comes from experience and experience comes from bad judgment Winston Churchill

48
Russell D. Hull Professor of Medicine,Thrombosis Research Unit University of Calgary Current Guidelines for Deep Vein Thrombosis Prophylaxis in Orthopedic Surgery: ACCP Guidance and Risk Stratification Strategies – Matching Intensity of Therapy with Patient Subgroups

49
Diagnosis Of Fatal Pulmonary Embolism In North America Is Problematic Due To The Low Autopsy Rate

50
Evidence-Based Guidelines Recommendations Two Components: Benefit/Risk Benefit/Risk Methodological Quality of a Recommendation Methodological Quality of a Recommendation The 7 th ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126: 179S-187S. Grade 1Grade 1 Grade AGrade A Grade BGrade B Grade CGrade C Or Or Grade 2Grade 2

51
Methodologic Quality Grade A Consistent findings by randomized trials Grade B Randomized clinical trials with inconsistent results Grade C Observational studies Chest 2004; 126: 179S-187S.

52
Benefit/RiskBenefit/Risk Grade 1 If we are very certain that the benefits do, or do not, outweigh the risks, burdens, and cost, we make a strong recommendation (in our formulation, Grade 1) Grade 2 If we are less certain of the magnitude of the benefits and the risks, burdens, and costs, and thus of their relative impact, we make a weaker Grade 2 recommendations Chest 2004; 126: 179S-187S.
 Grade 2 If we are less certain of the magnitude of the benefits and the risks, burdens, and costs, and thus of their relative impact, we make a weaker Grade 2 recommendations Chest 2004; 126: 179S-187S.")
53
Thromboprophylaxis Regimens Mechanical Graduated Compression Stockings (GCS) Intermittent Pneumatic Compression (IPC) Anticoagulants Low-Dose Unfractionated Heparin (LDUH) Low-Molecular-Weight Heparin (LMWH/fondaparinux) Vitamin-K-Antagonists (VKA) Chest 2004; 126: 179S-187S.
 Intermittent Pneumatic Compression (IPC) Anticoagulants Low-Dose Unfractionated Heparin (LDUH) Low-Molecular-Weight Heparin (LMWH/fondaparinux) Vitamin-K-Antagonists (VKA) Chest 2004; 126: 179S-187S.")
54
We recommend against the use of ASA alone as prophylaxis against VTE for any patient group (Grade 1A) ASA Chest 2004; 126: 179S-187S.
 ASA Chest 2004; 126: 179S-187S.")
55
Antiplatelets:Antiplatelets: -ASA-ASA X X

56
We recommend against the routine use of DUS screening at the time of hospital discharge in asymptomatic patients following major orthopedic surgery (Grade 1A) Screening for DVT Chest 2004; 126: 338S-400S.
 Screening for DVT Chest 2004; 126: 338S-400S.")
57
Levels of Thromboembolism Risk in Surgical Patients Without Prophylaxis Patients are stratified as: Low Risk Low Risk Moderate Risk Moderate Risk High Risk High Risk Highest Risk Highest Risk Risk Stratification Chest 2004; 126: 338S-400S.

58
CalfProximal DVT, % PE, % ClinicalFatal High Risk Surgery in patients with multiple risk factors (age >40 yr, cancer prior VTE) Successful Prevention Strategies: 40-8010-204-100.2-5 Hip or knee arthroplasty, HFS Major trauma; SCI Chest 2004; 126: 338S-400S. LMWH (>3,400 U daily), fondaparinux, oral VKAs (INR, 2-3), or IPC/GCS + LDUH/LMWH
, fondaparinux, oral VKAs (INR, 2-3), or IPC/GCS + LDUH/LMWH.")
59
Orthopaedic Surgery

60
Highest risk Elective Hip Surgery

61
Elective Hip Arthroplasty For patients undergoing elective THR, we recommend the routine use of one of the following three anticoagulants: LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) fondaparinux, (2.5 mg started 6 to 8h after surgery) fondaparinux, (2.5 mg started 6 to 8h after surgery) Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Chest 2004; 126: 338S-400S.
![Elective Hip Arthroplasty For patients undergoing elective THR, we recommend the routine use of one of the following three anticoagulants: LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) fondaparinux, (2.5 mg started 6 to 8h after surgery) fondaparinux, (2.5 mg started 6 to 8h after surgery) Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Chest 2004; 126: 338S-400S.](http://images.slideplayer.com/1/678021/slides/slide_61.jpg "Elective Hip Arthroplasty For patients undergoing elective THR, we recommend the routine use of one of the following three anticoagulants: LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day) fondaparinux, (2.5 mg started 6 to 8h after surgery) fondaparinux, (2.5 mg started 6 to 8h after surgery) Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all Grade 1A] Chest 2004; 126: 338S-400S.")
62
We recommend against the use of: As the only method of thromboprophylaxis in these patients (Grade 1A) ASA ASA Dextran Dextran Low-dose unfractionated heparin Low-dose unfractionated heparin Graduated compression stockings Graduated compression stockings Intermittent pneumatic compression Intermittent pneumatic compression Venous foot pump Venous foot pump Elective Hip Arthroplasty Chest 2004; 126: 338S-400S.
 ASA ASA Dextran Dextran Low-dose unfractionated heparin Low-dose unfractionated heparin Graduated compression stockings Graduated compression stockings Intermittent pneumatic compression Intermittent pneumatic compression Venous foot pump Venous foot pump Elective Hip Arthroplasty Chest 2004; 126: 338S-400S.")
63
Underlying values and preferences We have not recommended the use of: fondaparinux over LMWH and VKA fondaparinux over LMWH and VKA Or the use of LMWH over VKA Or the use of LMWH over VKA Because we place a relatively low value on the prevention of venographic thrombosis and a relatively high value on minimizing bleeding complications Elective Hip Arthroplasty Chest 2004; 126: 338S-400S.

64
Elective Knee Surgery Highest risk

65
For patients undergoing elective TKA, we recommend routine thromboprophylaxis using: LMWH (at the usual high-risk dose) LMWH (at the usual high-risk dose) Fondaparinux Fondaparinux Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) all Grade 1A Elective Knee Arthroplasty Chest 2004; 126: 338S-400S.
 LMWH (at the usual high-risk dose) Fondaparinux Fondaparinux Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) all Grade 1A Elective Knee Arthroplasty Chest 2004; 126: 338S-400S.")
66
The optimal use of IPC is an alternative option to anticoagulant prophylaxis (Grade 1B) The optimal use of IPC is an alternative option to anticoagulant prophylaxis (Grade 1B) We recommend against the use of any of the following as sole methods of thromboprophylaxis: We recommend against the use of any of the following as sole methods of thromboprophylaxis: ASA (Grade 1A)ASA (Grade 1A) LDUH (Grade 1A)LDUH (Grade 1A) Or venous foot pump (Grade 1B)Or venous foot pump (Grade 1B) Elective Knee Arthroplasty Chest 2004; 126: 338S-400S.
 The optimal use of IPC is an alternative option to anticoagulant prophylaxis (Grade 1B) We recommend against the use of any of the following as sole methods of thromboprophylaxis: We recommend against the use of any of the following as sole methods of thromboprophylaxis: ASA (Grade 1A)ASA (Grade 1A) LDUH (Grade 1A)LDUH (Grade 1A) Or venous foot pump (Grade 1B)Or venous foot pump (Grade 1B) Elective Knee Arthroplasty Chest 2004; 126: 338S-400S.")
67
Underlying values and preferences We have not recommended: fondaparinux over LMWH and VKA fondaparinux over LMWH and VKA Or LMWH over VKA Or LMWH over VKA Because we place a relatively low value on the prevention of venographic thrombosis and a relatively high value on minimizing bleeding complications Elective Knee Arthroplasty Chest 2004; 126: 338S-400S.

68
Hip Fracture Surgery Highest risk

69
For patients undergoing hip fracture surgery, we recommend the routine use of: fondaparinux (Grade 1A) fondaparinux (Grade 1A) LMWH at the usual high-risk dose (Grade 1C) LMWH at the usual high-risk dose (Grade 1C) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) (Grade 2B) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) (Grade 2B) Or LDUH (Grade 1B) Or LDUH (Grade 1B) Hip Fracture Surgery Chest 2004; 126: 338S-400S.
 fondaparinux (Grade 1A) LMWH at the usual high-risk dose (Grade 1C) LMWH at the usual high-risk dose (Grade 1C) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) (Grade 2B) Adjusted-dose VKA (target INR, 2.5; INR range, 2.0 to 3.0) (Grade 2B) Or LDUH (Grade 1B) Or LDUH (Grade 1B) Hip Fracture Surgery Chest 2004; 126: 338S-400S.")
70
We recommend against the use of ASA alone (Grade 1A) We recommend against the use of ASA alone (Grade 1A) If surgery will likely be delayed, we recommend that prophylaxis with either LDUH or LMWH be initiated during the time between hospital admission and surgery (Grade 1C+) If surgery will likely be delayed, we recommend that prophylaxis with either LDUH or LMWH be initiated during the time between hospital admission and surgery (Grade 1C+) We recommend mechanical prophylaxis if anticoagulant prophylaxis is contraindicated because of a high risk of bleeding (Grade 1C) We recommend mechanical prophylaxis if anticoagulant prophylaxis is contraindicated because of a high risk of bleeding (Grade 1C) Hip Fracture Surgery Chest 2004; 126: 338S-400S.
 We recommend against the use of ASA alone (Grade 1A) If surgery will likely be delayed, we recommend that prophylaxis with either LDUH or LMWH be initiated during the time between hospital admission and surgery (Grade 1C+) If surgery will likely be delayed, we recommend that prophylaxis with either LDUH or LMWH be initiated during the time between hospital admission and surgery (Grade 1C+) We recommend mechanical prophylaxis if anticoagulant prophylaxis is contraindicated because of a high risk of bleeding (Grade 1C) We recommend mechanical prophylaxis if anticoagulant prophylaxis is contraindicated because of a high risk of bleeding (Grade 1C) Hip Fracture Surgery Chest 2004; 126: 338S-400S.")
71
Distal Fracture of the Lower Extremity

72
We suggest that clinicians not use thromboprophylaxis routinely in patients with isolated lower extremity injuries (Grade 2A) Isolated Lower Extremity Injuries Chest 2004; 126: 338S-400S.
 Isolated Lower Extremity Injuries Chest 2004; 126: 338S-400S.")
73
Timing of Thromboprophylaxis Timing of Thromboprophylaxis Knee arthroscopy Knee arthroscopy Thrombocytopenia Thrombocytopenia Special Considerations

74
Timing of Thromboprophylaxis

75
We performed a randomized, double-blind trial Patients received either: Just-in-time subcutaneous dalteparin sodium once daily (initiated immediately pre-operatively or early post-operatively) Or warfarin during the acute hospital stay North American Dalteparin Trial (NAFT) Hull et al. Arch Intern Med 2000; 160: 2199-2207. Hull et al. Arch Intern Med 2000; 160: 2208-2215.

76
Multicentre: 28 centres in the United States and Canada Randomized Double-blind NAFT Hull et al. Arch Intern Med 2000; 160: 2199-2207. Hull et al. Arch Intern Med 2000; 160: 2208-2215.

77
Overall Study Design Phase I Phase II Day 0 (surgery) Day 6±2 Day 7±2 Day 35±2 Pre-op Dalteparin (2,500 IU)Dalteparin Post-op Dalteparin (2,500 IU)Dalteparin Warfarin Placebo for Warfarin Venography Venography (5,000 IU) (5,000 IU) NAFT Hull et al. Arch Intern Med 2000; 160: 2199-2207. Hull et al. Arch Intern Med 2000; 160: 2208-2215.

78
Frequency of DVT: Acute Hospital Phase 0 0 5 5 10 15 20 25 DVT Rate (%) All DVT Proximal DVT Pre-operative dalteparin Post-operative dalteparin Combined pre- and post- operative dalteparin Warfarin Pre-op dalteparin vs warfarin: All DVT 55% (p<0.001); Proximal DVT 72% (p=0.035) Pre-op dalteparin vs warfarin: All DVT 55% (p<0.001); Proximal DVT 72% (p=0.035) Post-op dalteparin vs warfarin: All DVT 45% (p<0.001); Proximal DVT 72% (p=0.033) Post-op dalteparin vs warfarin: All DVT 45% (p<0.001); Proximal DVT 72% (p=0.033) Combined pre- and post-op dalteparin vs warfarin: All DVT 50% (p<0.001); Proximal DVT 72% (p=0.009) Combined pre- and post-op dalteparin vs warfarin: All DVT 50% (p<0.001); Proximal DVT 72% (p=0.009) Relative Risk Reductions Hull et al. Arch Intern Med 2000; 160: 2199-2207. Hull et al. Arch Intern Med 2000; 160: 2208-2215.

79
Low-Molecular-Weight Heparin Prophylaxis Using Dalteparin in Close Proximity to Surgery Vs Warfarin in Hip Arthroplasty Patients A modified dalteparin regimen in close proximity to surgery resulted in substantive risk reductions for all and proximal deep vein thrombosis, compared with warfarin therapy A modified dalteparin regimen in close proximity to surgery resulted in substantive risk reductions for all and proximal deep vein thrombosis, compared with warfarin therapy Such findings have not been observed with low-molecular-weight heparin therapy commenced 12 hours preoperatively or 12 to 24 hours postoperatively vs oral anticoagulants Such findings have not been observed with low-molecular-weight heparin therapy commenced 12 hours preoperatively or 12 to 24 hours postoperatively vs oral anticoagulants Hull et al. Arch Intern Med 2000; 160: 2199-2207.

80
Increased major but not serious bleeding occurred in patients receiving preoperative dalteparin Increased major but not serious bleeding occurred in patients receiving preoperative dalteparin Dalteparin therapy initiated postoperatively provided superior efficacy vs warfarin without significantly increased overt bleeding Dalteparin therapy initiated postoperatively provided superior efficacy vs warfarin without significantly increased overt bleeding Low-Molecular-Weight Heparin Prophylaxis Using Dalteparin in Close Proximity to Surgery Vs Warfarin in Hip Arthroplasty Patients Hull et al. Arch Intern Med 2000; 160: 2199-2207.

81
Quadratic Fit For Study Odds Ratio For DVT Vs Number Of Hours From Surgery For The First Dose Of LMW Heparin Upper and lower dashed lines indicate the 95% confidence interval for the true odds ratio Hours from Surgery Odds Ratio Hull et al. Arch Intern Med 2001; 161: 1952-60

82
Impact of Timing of Prophylaxis: Total DVT in Patients Undergoing Elective Hip Surgery RelativeRisk (95% CI*) RelativeRisk pValue 0.891.010.570.50 0.444 0.444 0.984 0.984 0.008 0.008<0.001 Favours LMWH Favours Oral Anticoagulants 1.00100.00.1010.0 Hull (1993) HamulyakFrancis Hull (2000) Study Expt n/N (%) Ctrl n/N (%) 69/332 (20.8) 27/195 (13.8) 28/192 (14.6) 80/673 (11.8) 79/340 (23.2) 27/196 (13.8) 49/190 (25.8) 81/338 (24.0) Time of Initiation (hrs) Post:18-24Pre:12 Pre: 2 Post:4-6 0.01 * CI Fixed Hull et al. Arch Intern Med 2001; 161: 1952-60

83
RelativeRisk pValue RelativeRisk (95% CI*) Hull (1993) HamulyakFrancis Hull (2000) Study Expt n/N (%) Ctrl n/N (%) Time of Initiation (hrs) 1.26 0.526 0.526 1.00 100.00.1010.0 16/332 (4.8) 13/340 (3.8) Post:18-24 0.01 Favours LMWH Favours Oral Anticoagulants 6/712 (0.8) 10/192 (5.2) 12/195 (6.2) 11/363 (3.0) 16/190 (8.4) 9/196 (4.6) 0.011 0.011 0.218 0.495 0.495 0.28 0.62 1.34 Post:4-6 Pre: 2 Pre:12 Impact of Timing of Prophylaxis: Proximal DVT in Patients Undergoing Elective Hip Surgery Hull et al. Arch Intern Med 2001; 161: 1952-60 * CI Fixed

84
Timing of Initial Administration of Low-Molecular-Weight Heparin Prophylaxis Against Deep Vein Thrombosis in Patients Following Elective Hip Arthroplasty The timing of initiating LMWH significantly influences antithrombotic effectiveness The timing of initiating LMWH significantly influences antithrombotic effectiveness The practice of delayed initiation of LMWH prophylaxis results in suboptimal antithrombotic effectiveness without a substantive safety advantage The practice of delayed initiation of LMWH prophylaxis results in suboptimal antithrombotic effectiveness without a substantive safety advantage Hull et al. Arch Intern Med 2001; 161: 1952-60

85
For major orthopedic surgical procedures, we recommend that a decision about the timing of the initiation of pharmacologic prophylaxis be based on the efficacy-to-bleeding tradeoffs for that particular agent (Grade 1A) For major orthopedic surgical procedures, we recommend that a decision about the timing of the initiation of pharmacologic prophylaxis be based on the efficacy-to-bleeding tradeoffs for that particular agent (Grade 1A) For LMWH, there are only small differences between starting preoperatively or postoperatively, and both options are acceptable (Grade 1A) For LMWH, there are only small differences between starting preoperatively or postoperatively, and both options are acceptable (Grade 1A) Timing of Prophylaxis Chest 2004; 126: 338S-400S.
 For major orthopedic surgical procedures, we recommend that a decision about the timing of the initiation of pharmacologic prophylaxis be based on the efficacy-to-bleeding tradeoffs for that particular agent (Grade 1A) For LMWH, there are only small differences between starting preoperatively or postoperatively, and both options are acceptable (Grade 1A) For LMWH, there are only small differences between starting preoperatively or postoperatively, and both options are acceptable (Grade 1A) Timing of Prophylaxis Chest 2004; 126: 338S-400S.")
86
Dosing Options for Patients Undergoing Hip Replacement Surgery Dose of Dalteparin to be Given Subcutaneously Timing of First Dose of Dalteparin 10-14 hr Pre-op Within 2 hr Pre-op 4-8 hr Post-op 1 Post-op Period 2 Post-op start Pre-op start-day of surgery Pre-op start-evening before surgery 4 --- --- --- --- 5000 IU 2500 IU 2500 IU3 2500 IU3 5000 IU 5000 IU qd 5000 IU qd 5000 IU qd 1 Or later, if hemostasis has not been achieved. 2 Up to 14 days of treatment was well tolerated in controlled clinical trials, where the usual duration of treatment was 5 to 10 days postoperatively. 3 Allow a minimum of 6 hours between this dose and the dose to be given on Postoperative Day 1. Adjust the timing of the dose on Postoperative Day 1 accordingly. 4 Allow approximately 24 hours between doses. www.fda.gov/medwatch/SAFETY/2003/03Feb_PI/Fragmin_pdf

87
Knee Arthroscopy

88
We suggest clinicians do not use routine thromboprophylaxis in these patients, other than early mobilization (Grade 2B) Knee Arthroscopy Chest 2004; 126: 338S-400S.
 Knee Arthroscopy Chest 2004; 126: 338S-400S.")
89
For patients undergoing arthroscopic knee surgery who are at a higher than usual risk based on: Pre existing VTE risk factors Pre existing VTE risk factors Or following a prolonged or complicated procedure Or following a prolonged or complicated procedure We suggest thromboprophylaxis with LMWH (Grade 2B) Knee Arthroscopy Chest 2004; 126: 338S-400S.
 Knee Arthroscopy Chest 2004; 126: 338S-400S.")
90
Thrombocytopenia The Harbinger of Doom for Unfractionated Heparin

91
Risk for Heparin-Induced Thrombocytopenia with Unfractionated and Low Molecular-Weight Heparin Thromboprophylaxis: A Meta-Analysis Heparin-induced thrombocytopenia (HIT) is an uncommon but potentially devastating complication of anticoagulation with unfractionated heparin (UFH) or low-molecular- weight heparin (LMWH) Heparin-induced thrombocytopenia (HIT) is an uncommon but potentially devastating complication of anticoagulation with unfractionated heparin (UFH) or low-molecular- weight heparin (LMWH) The inverse variance–weighted average that determined the absolute risk for HIT with LMWH was 0.2%, and with UFH the risk was 2.6%. Most studies were of patients after orthopedic surgery The inverse variance–weighted average that determined the absolute risk for HIT with LMWH was 0.2%, and with UFH the risk was 2.6%. Most studies were of patients after orthopedic surgery Martel et al. Blood 2005; 106:2710-15

92
VTE is associated with HIT infrequently (<1%) in LMWH-treated patients, yet often (approximately one in eight cases) in unfractionated heparin- treated patients. Physicians should suspect the possibility of HIT if VTE develops during or soon after unfractionated heparin use; if thrombocytopenia is present, alternative anticoagulation should be used until HIT is excluded. Levine et al. CHEST 2006; 130(3): 681-687. How Frequently is VTE in Heparin-Treated Patients Associated with Heparin-Induced Thrombocytopenia (HIT)
: How Frequently is VTE in Heparin-Treated Patients Associated with Heparin-Induced Thrombocytopenia (HIT).")
93
Electronic Medical Alerts So Simple, So Complex Electronic Medical Alerts So Simple, So Complex One of the most consistent findings in health research is the gap between evidence and practice. One of the most consistent findings in health research is the gap between evidence and practice. Durieux. N Engl J Med 2005: 352: 1034-1036

95
Appendix

96
Obesity

97
The Safety of Dosing Dalteparin Based on Actual Body Weight for the Treatment of Acute Venous Thromboembolism in Obese Patients Our study suggests that it is safe to administer dalteparin at or near full dose based on actual body weight for the treatment of acute venous thromboembolism without an increased risk of major hemorrhage Limiting the dose of dalteparin to 18 000 IU could lead to an increased risk of recurrence of venous thromboembolism Al-Yaseen et al. J Thromb Haemost 2005; 3: 100-102.

98
Dosing in Heavy-Weight/Obese Patients with the LMWH, Tinzaparin: A Pharmacodynamic Study Subcutaneous tinzaparin dosing in heavy or obese patients is appropriate based on body weight alone; the dose need not be capped at a maximal absolute dose Hainer J et al. J Thromb Haemost 2002; 87: 817-823.

99
Renal Impairment

100
The use of a 30-mL/min (0.50-mL/s) cutoff is not justified, on the basis of currently available evidence, to select individuals at increased risk of accumulation when LMW heparin is used The use of a 30-mL/min (0.50-mL/s) cutoff is not justified, on the basis of currently available evidence, to select individuals at increased risk of accumulation when LMW heparin is used The pharmacokinetic response to impaired renal function may differ among low-molecular- weight heparin preparations The pharmacokinetic response to impaired renal function may differ among low-molecular- weight heparin preparations Is Impaired Renal Function a Contraindication to the Use of Low-Molecular-Weight Heparin? Nagge et al. Arch Intern Med 2002; 162: 2605-2609.

101
Evidence-Based Guidelines Recommendations Two Components: Methodological Quality of a Recommendation Methodological Quality of a Recommendation Grade A Grade A Grade B or Grade B or Grade C Grade C Benefit/Risk Benefit/Risk Grade A or Grade A or Grade B Grade B The 7 th ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126: 179S-187S.

102
Venous Thromboembolism: Recognizing and Treating the Patient at Risk Peter Hanson, MD Medical Director of Orthopaedics Chief of Staff Grossmont Hospital, La Mesa, CA

103
What Are We Trying To Prevent? Asymptomatic DVT? Asymptomatic DVT? Symptomatic DVT? Symptomatic DVT? All PEs? All PEs? Fatal PEs? Fatal PEs? Post-phlebitic Syndrome? Post-phlebitic Syndrome?

104
Dear Surgeon……….. ??

107
VenousStasis Tourniquet Immobilization and bed rest Vascular Injury Surgical manipulation of the limb Endothelial injury Hypercoagulability Increase in thromboplastin agents Very High Risk Medium/High Risk Low/Medium Risk Virchows Triad Thrombosis Risk in Orthopedic Surgery

108
DVT Prevention in Knee Replacement (Total DVT by venography)
")
109
Preventing DVT in TKR With Aspirin Aspirin Alone Is Not Effective Prophylaxis After TKR

110
DVT Prophylaxis in Total Knee Replacement (TKR) LMWH vs Warfarin Spiro et al. Blood. 1994;84(suppl 1):246a. Enoxaparin 30 mg sc twice daily (n=173) Warfarin dose-adjusted INR 2-3 (n=176) Total DVT 25.4 45.4 0 10 20 30 40 50 P 0.001 P<0.001 Proximal DVT 1.7 11.4 0 2 4 6 8 10 12 Enoxaparin 30 mg sc twice daily (n=173) Warfarin dose-adjusted INR 2-3 (n=176) Incidence %
:246a. Enoxaparin 30 mg sc twice daily (n=173) Warfarin dose-adjusted INR 2-3 (n=176) Total DVT P P<0.001 Proximal DVT Enoxaparin 30 mg sc twice daily (n=173) Warfarin dose-adjusted INR 2-3 (n=176) Incidence %.")
111
2.3 3.4 23.3 5.2 6.4 33.5 0 10 20 30 40 Major BleedingWound Complications (clinically significant) Overall Bleeding Bleeding in Total Knee Replacement (TKR) LMWH vs Warfarin Warfarin dose-adjusted INR 2-3 Enoxaparin 30 mg sc bid P=0.04 Incidence % Spiro et al. Blood. 1994;84(suppl 1):246a.
:246a..")
112
Enoxaparin vs Warfarin in Total Knee Replacement Leclerc JR et al. Ann Intern Med. 1996, 124.619-626.

113
Fondaparinux Targeted Mechanism of Action IIaII Fibrinogen Fibrin clot Extrinsic pathway Intrinsic pathway 3 ATIII Xa 1 ATIII 2 Fondaparinux Xa ATIII = antithrombin III Antithrombin Adapted with permission from Turpie AGG, et al. N Engl J Med. 2001;344:619-625.

114
Incidence of patients with VTE up to day 11 27.8 12.5 0 4 8 12 16 20 24 28 32 Fondaparinux 2.5 mg QD (n=361) Enoxaparin 30 mg BID(n=363) n = 45 n = 101 RRR = 55% P = 0.0000003 95% CI 9.2; 16.3 23.3; 32.7 Patients (%) TKR Efficacy Results: Primary Endpoint Pentamaks
 Enoxaparin 30 mg BID(n=363) n = 45 n = 101 RRR = 55% P = % CI 9.2; ; 32.7 Patients (%) TKR Efficacy Results: Primary Endpoint Pentamaks")
115
Any DVT P < 0.0001 Proximal DVT P = 0.056 Patients (%) 12.5 2.4 9.4 27.1 5.4 21.3 0 5 10 15 20 25 30 Distal DVT only P = 0.000009 Fondaparinux Enoxaparin TKR Efficacy Results: Secondary Endpoint Incidence of patients with VTE up to day 11 Pentamaks
 Distal DVT only P = Fondaparinux Enoxaparin TKR Efficacy Results: Secondary Endpoint Incidence of patients with VTE up to day 11 Pentamaks")
116
Pentamaks NS = no statistically significant difference Fondaparinux 2.5 mg QD Enoxaparin 30 mg BID Fatal bleeding, n Nonfatal bleeding in critical organ, n Bleeding leading to reoperation, n (%) Bleeding with transfusion 2 units and/or hg decrease 2 g/dL, n (%) Other bleeding (minor), n (%) TKR Safety: Bleeding P value NS <0.05 NS From 1st injection to day 11 – all treated patients 0 0 2 (0.4) 9 (1.7) 15 (2.9) 0 0 1 (0.2) 0 (0.0) 21 (4.0)
 Bleeding with transfusion 2 units and/or hg decrease 2 g/dL, n (%) Other bleeding (minor), n (%) TKR Safety: Bleeding P value NS <0.05 NS From 1st injection to day 11 – all treated patients (0.4) 9 (1.7) 15 (2.9) (0.2) 0 (0.0) 21 (4.0)")
117
Incidence of VTE (%) 25.7 19.7 0 10 20 30 >7.5 and 9 hrs (n=61) >9 and 12 hrs (n=74) 40 30.0 >13 hrs (n=20) Time to first dalteparin dose VTE, venous thromboembolism Thromboprophylaxis for Knee Replacement Dalteparin vs Warfarin: Post-Hoc Analysis Post-hoc analysis of patients (n=155) who received the 1 st dose of dalteparin >7.5 hours postoperatively Ayers DC et al. Poster presented at: American Academy of Orthopaedic Surgeons 2006 Annual Meeting; March 22, 2006; Chicago, IL.

118
Rationale for Extended Prophylaxis After THR/TKR Cumulative Risk of Thromboembolic Events During First 3 Months Postoperatively All VTE PE 0 1 2 3 142842567084 Primary Knee Primary Hip Days 0 1 2 3 142842567084 Days Primary Knee Primary Hip The incidence of thromboembolic events does not stabilize until approximately 10 weeks after THR Incidence % White et al. Arch Intern Med. 1998;158:1525-1531.

119
Rationale for Extended Prophylaxis White et al. Arch Intern Med. 1998;158:1525-1531. 1.1% 0.8% 0 0.5 1.0 Total Hip Arthroplasty n = 19,000 Total Knee Arthroplasty n = 24,000 % of patients with PE Incidence of PE within 3 months post-surgery

120
76 47 0 20 40 60 80 Total Hip Replacement Total Knee Replacement % DVT Diagnosis Made Post-Discharge n=19,000n=24,000 Rationale for Extended Prophylaxis White et al. Arch Intern Med. 1998;158:1525-1531.

121
Total Knee Arthroplasty Total Hip Arthroplasty Median Time of DVT Diagnosis After Surgery (Days) 05101520 17 Days 7 Days n=19,000 n=24,000 Rationale for Extended Prophylaxis White et al. Arch Intern Med. 1998;158:1525-1531.

122
NAFT Study Design visit Screening Day 35 Dalteparin (post-op) Dalteparin Dalteparin (pre-op) Dalteparin Warfarin Venography Switched to Placebo Acute Phase Extended Phase Day 0 (surgery) Day 6 Day 7 Venography
 Dalteparin Dalteparin (pre-op) Dalteparin Warfarin Venography Switched to Placebo Acute Phase Extended Phase Day 0 (surgery) Day 6 Day 7 Venography")
123
*RR=combined risk reduction vs. warfarin/placebo group P=0.023 P<0.001 § P=0.007 ¥ P=0.003 NAFT Results Treatment Group Proximal DVT RR* Total DVT RR* (%) Pre-op dalteparin3.167 17.255 Pre-op dalteparin3.167 17.255 Post-op dalteparin2.079 § 22.241 ¥ Warfarin/placebo 9.2 (5 de novo)36.7 Extended Outpatient Phase (Day 35 ± 2) (Patients with negative bilateral venograms at day 6±2) Hull RD, et al. Arch Intern Med. 2000;160:2199-2207.
 Pre-op dalteparin Pre-op dalteparin Post-op dalteparin2.079 § ¥ Warfarin/placebo 9.2 (5 de novo)36.7 Extended Outpatient Phase (Day 35 ± 2) (Patients with negative bilateral venograms at day 6±2) Hull RD, et al. Arch Intern Med. 2000;160:")
124
Major Treatment Group Bleeding (%) Wound Hematoma (%) Complicated Uncomplicated Complicated Uncomplicated Pre-op dalteparin0 0.5 2.5 Post-op dalteparin0 0.5 2.1 Warfarin0 1.1 2.8 NAFT Results Extended Outpatient Phase (Day 35 ± 2) (Patients with negative bilateral venograms at day 6±2) Hull RD, et al. Arch Intern Med. 2000;160:2199-2207.

125
Enoxaparin: Extended Prophylaxis Comp et al 2001 JBJS: Comp et al 2001 JBJS: l Enoxaparin 7-10 days vs 4 wks, TKAs and THAs l Extended dosing in THAs significantly decreased DVTs, no difference in TKAs l No added bleeding risk

126
Recent Studies: Extended Prophylaxis Eikelboom et al 2001 Lancet: Eikelboom et al 2001 Lancet: l Meta-analysis of 3999 patients, THA and TKA, extended prophylaxis vs placebo/no tx l Decreased Sxic DVT in hips (not knees) l Decreased Asxic DVT in hips (not knees) l 20 sxic DVT/1000 pts, 1death/1000 pts prevented l $4-7 / day in UK, $24-28 / day in US l No warfarin studies available
 l Decreased Asxic DVT in hips (not knees) l 20 sxic DVT/1000 pts, 1death/1000 pts prevented l $4-7 / day in UK, $24-28 / day in US l No warfarin studies available")
127
Extended Prophylaxis: PENTasaccharide in Hip- FRActure Surgery (PENTHIFRA Plus) Results Incidence (%) of Events PlaceboFondaparinux RRR % VTE*351.495.9 DVT*33.91.495.8 Proximal DVT* 15.80.994.3 Major Bleeding Major Bleeding 0.62.4 Minor Bleeding Minor Bleeding 0.61.5 Eriksson BI et al. Arch Intern Med. 2003;163:1337-1342. * p < 0.001 no significant difference between treatment groups

128
Extended Prophylaxis with Fondaparinux: Hip Fracture Repair 35.0% 1.4% 0 5 10 15 20 25 30 35 Fondaparinux(n=208)Placebo(n=220) n = 3 n = 77 RRR = 96% Patients (%) Eriksson BI et al. Arch Intern Med. 2003;163:1337-1342.

129
Guidelines for Prevention of VTE: Are They Relevant? Current Findings: Applications for Thromboprophylaxis in Orthopaedic Surgery The Four Seasons Hotel, San Francisco March 10, 2004

130
Definition of Practice Guidelines Practice guidelines are systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances.

131
Seventh ACCP Recommendations

134
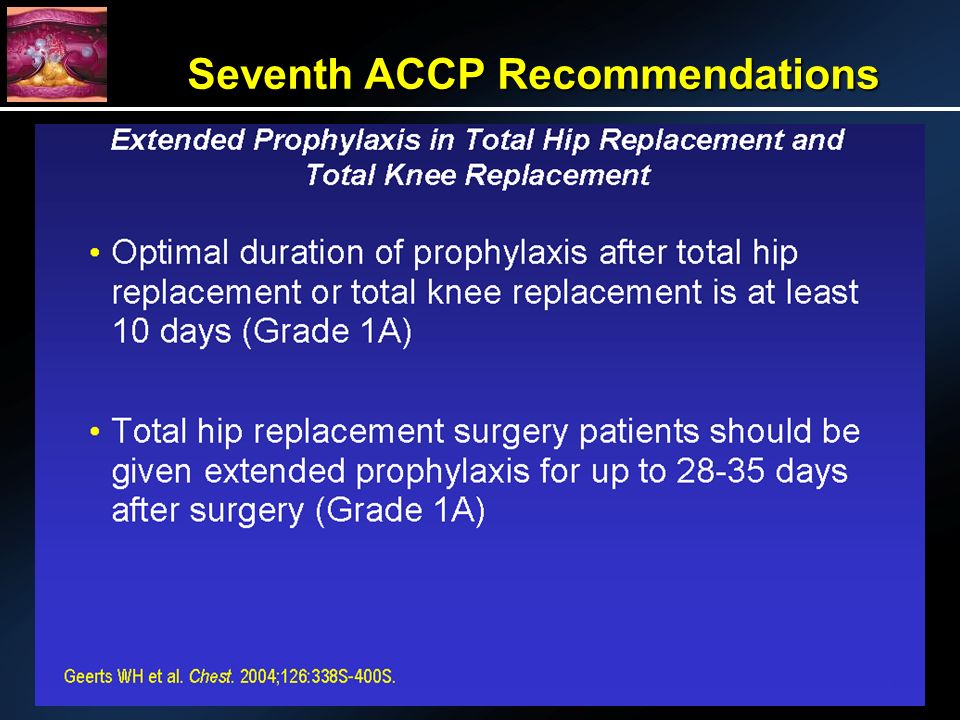
Duration Of Treatment (ACCP) Optimal duration of prophylaxis after THR or TKR - at least 7-10 days Optimal duration of prophylaxis after THR or TKR - at least 7-10 days Extended prophylaxis with LMWH recommended at least for high risk patients Extended prophylaxis with LMWH recommended at least for high risk patients
 Optimal duration of prophylaxis after THR or TKR - at least 7-10 days Optimal duration of prophylaxis after THR or TKR - at least 7-10 days Extended prophylaxis with LMWH recommended at least for high risk patients Extended prophylaxis with LMWH recommended at least for high risk patients")
135
Multimodal Approach to VTED Prophylaxis for THA and TKA Paul F. Lachiewicz, M.D. Department of Orthopaedics University of North Carolina - Chapel Hill ACCP Orthopaedists

136
THA Techniques Then Now Then Now Bed rest1 week<1 day Hospital stay2-3 weeks2-4 days EBL (mean) 1650 ml300-600 ml BloodHomologousAutologous Transfusion (mean) 1144 ml0-500 ml AnesthesiaGeneralRegional
 1650 ml ml BloodHomologousAutologous Transfusion (mean) 1144 ml0-500 ml AnesthesiaGeneralRegional")
137
These major changes in THA techniques suggest that our older ideas about chemoprophylaxis should be reconsidered in 2007

138
PreoperativeIntraoperativePostoperative Multimodal Prophylaxis

139
Preoperative Risk Factors VTED Genetic predisposition Genetic predisposition Hypercoaguable states Hypercoaguable states Prior history PE Prior history PE Oral contraceptives (?) Oral contraceptives (?) Classic risk factors have not Classic risk factors have not correlated with VTED in elective THA patients
 Oral contraceptives ( ) Classic risk factors have not Classic risk factors have not correlated with VTED in elective THA patients")
140
Preoperative Autologous Donation Retrospective study: 2043 patients Retrospective study: 2043 patients Donation 1037; not 1006 Donation 1037; not 1006 DVT Donation 9.0% (p=0.003) DVT Donation 9.0% (p=0.003) (venogram) Not13.5% (venogram) Not13.5% P.E. Donation 0.3% (ns) P.E. Donation 0.3% (ns) (clinical) Not 0.7% (clinical) Not 0.7% Bae et al. JBJS (B) 2001
 P.E. Donation 0.3% (ns) (clinical) Not 0.7% (clinical) Not 0.7% Bae et al. JBJS (B)")
141
Thromboembolism THR Anesthesia Spinal or epidural anesthesia reduces risk by 40-50% Spinal or epidural anesthesia reduces risk by 40-50% Regional anesthesia increased blood flow in lower extremities during and after the procedure Regional anesthesia increased blood flow in lower extremities during and after the procedure Lower blood loss, ? quicker surgery Lower blood loss, ? quicker surgery

142
Mechanical Prophylaxis THA Intraoperative use does not interfere with positioning, exposure, placement of implants

143
Intraop and postop IPC is specific localized prophylaxis: Decreased venous stasis Decreased venous stasis increase venous velocity increase venous volume Inhibits coagulation cascade Inhibits coagulation cascade tissue factor pathway inhibitor tissue factor pathway inhibitor factor VIIa factor VIIa NO and endogenous NO synthase NO and endogenous NO synthase Mechanical Prophylaxis THA

144
Wide variety of devices Wide variety of devices l foot pump l calf l thigh-calf Each device has its own mechanics with resultant change in peak venous velocity and venous volume Each device has its own mechanics with resultant change in peak venous velocity and venous volume For THA, optimal characteristics of pneumatic compression are not known For THA, optimal characteristics of pneumatic compression are not known Mechanical Prophylaxis THA

145
Venous Hemodynamics After THA Devices with rapid inflation time Devices with rapid inflation time l Produced the greatest increase in peak venous velocity Devices that compress calf and thigh Devices that compress calf and thigh l Produced the greatest increase in venous volume

146
Multimodal Prophylaxis June 1991 – May 2005 June 1991 – May 2005 Single surgeon Single surgeon 1042 consecutive THA 1042 consecutive THA (388 in previous study) (388 in previous study) 10 exclusions 10 exclusions (5 hemophilia, 5 other) (5 hemophilia, 5 other) Lachiewicz, Soileau. Clin Orthop 2006

147
Study Group 1032 hip procedures 1032 hip procedures 422 male, 610 female 422 male, 610 female Mean age 64 (22-95) Mean age 64 (22-95) Primary 680 Primary 680 Revision 352 *Patients with prior history of TED or on warfarin for cardiac conditions not excluded
 Mean age 64 (22-95) Primary 680 Primary 680 Revision 352 *Patients with prior history of TED or on warfarin for cardiac conditions not excluded")
148
Materials & Methods Anesthesia Anesthesia Regional95% General only 5% Intraoperative mechanical Intraoperative mechanical l bilateral, thigh-high l sterile sleeve-operative limb l single manufacturer Recovery room + until discharge Recovery room + until discharge Duplex ultrasound prior to discharge (day 3-8) Duplex ultrasound prior to discharge (day 3-8)
 Duplex ultrasound prior to discharge (day 3-8)")
149
Results - Mortality 1 fatal pulmonary embolism (0.09%) 1 fatal pulmonary embolism (0.09%) l 24 days postop-autopsy l patient in long-leg brace l minimal ambulation 1 cerebrovascular accident 1 cerebrovascular accident 1 unknown; abdominal pain & cardiac arrest 1 unknown; abdominal pain & cardiac arrest l ? M.I. vs P.E. 30 day mortality 3 of 1032 (0.3%) 30 day mortality 3 of 1032 (0.3%)
 30 day mortality 3 of 1032 (0.3%).")
150
Pulmonary Embolism Symptomatic 7 (0.7%) 4 early (POD #4-7) 3 late POD # 23 24 (fatal) 37 Only 1 of 7 also had DVT or Duplex
 4 early (POD #4-7) 3 late POD # (fatal) 37 Only 1 of 7 also had DVT or Duplex")
151
Mechanical Prophylaxis with Aspirin vs Aspirin Alone Prospective, randomized Prospective, randomized 100 hips - MR venography 100 hips - MR venography Rapid inflation device (Venaflow®) Rapid inflation device (Venaflow®) l applied in recovery room l epidural hypotensive anesthesia l aspirin 325 mg BID Mechanical + aspirin 8% prox. DVT Mechanical + aspirin 8% prox. DVT l aspirin alone 22% prox. DVT (p<.05) Ryan et al. JBJS 2002
 Ryan et al. JBJS")
152
Multimodal Prophylaxis THA Calf-thigh compression begun intraoperatively is effective and acceptable for 99% THA patients Calf-thigh compression begun intraoperatively is effective and acceptable for 99% THA patients 1032 hips 1032 hips Fatal PE 0.09% Fatal PE 0.09% Total DVT-PE 4.6% Total DVT-PE 4.6% Pulmonary embolism 0.7% Pulmonary embolism 0.7%

153
VTED After TKA Orthopaedic Perspective Different disease than after THA Different disease than after THA Most thrombi occur in calf only Most thrombi occur in calf only Extension to proximal veins occurs infrequently Extension to proximal veins occurs infrequently Pulmonary embolism rare Pulmonary embolism rare

154
Orthopaedists Concerns Prevention of Fatal PE Fatal PE Symptomatic PE Symptomatic PE Symptomatic DVT Symptomatic DVT Knee bleeding Knee bleeding How important is it to prevent asymptomatic venogram or Duplex scan-detected thrombi?

155
Orthopaedists Concerns Anticoagulation TKA Increased risk of major bleeding into knee and wound complications (0.9 – 5.2%) Increased risk of major bleeding into knee and wound complications (0.9 – 5.2%) True risk of bleeding and outcome not established for all TKA patients True risk of bleeding and outcome not established for all TKA patients Bleeding into TKA associated with hematomas, drainage, infection and poorer outcomes Bleeding into TKA associated with hematomas, drainage, infection and poorer outcomes
 Increased risk of major bleeding into knee and wound complications (0.9 – 5.2%) True risk of bleeding and outcome not established for all TKA patients True risk of bleeding and outcome not established for all TKA patients Bleeding into TKA associated with hematomas, drainage, infection and poorer outcomes Bleeding into TKA associated with hematomas, drainage, infection and poorer outcomes")
156
Mechanical Prophylaxis TKA Wide variety of devices Wide variety of devices l thigh-calf l calf only l foot pump Each device has its own mechanics with different changes in peak venous velocity and volume Each device has its own mechanics with different changes in peak venous velocity and volume Optimal characteristics for devices? Optimal characteristics for devices?

157
Venous Hemodynamics After TKA Westrich et al. JBJS (B) 1998 Flowtron DVTVenaFlowPlexiPulse foot-calf PlexiPulse foot A-V impulse system DPFJobst athrombic pump SCD system Calf-thighCalfFoot calfFoot Increase in verious velocity (%)
 1998 Flowtron DVTVenaFlowPlexiPulse foot-calf PlexiPulse foot A-V impulse system DPFJobst athrombic pump SCD system Calf-thighCalfFoot calfFoot Increase in verious velocity (%).")
158
Mechanical Prophylaxis TKA Devices with rapid inflation time produced the greatest increase in peak venous velocity Devices with rapid inflation time produced the greatest increase in peak venous velocity Devices that compress calf and thigh produced the greatest increase in venous volume Devices that compress calf and thigh produced the greatest increase in venous volume What matters most – What matters most – velocity or volume?

159
Two Mechanical Devices for Prophylaxis of Thromboembolism After TKA Lachiewicz et al. JBJS (B), Nov 2004. University of North Carolina-Chapel Hill Prospective, randomized study
, Nov University of North Carolina-Chapel Hill Prospective, randomized study.")
160
Patient Population 423 patients, 472 knees 423 patients, 472 knees Mean age 66.8 yrs (23-94) Mean age 66.8 yrs (23-94) Mean wt 87.3 kg (45-148) Mean wt 87.3 kg (45-148) DiagnosisDJD 307 DiagnosisDJD 307 RA 25 Rev. 64 Other 27

161
Results Asymmetrical Circumferential Compression Compression Compression Compression Patients 206217 Knees 232240 Mortality 0 1 (.46%) Pulm. Embolism01 (.46%) Thrombi 16 (6.9%) 36 (15%) p =.007 Calf 1530 Calf 1530 Proximal 16
 Thrombi 16 (6.9%) 36 (15%) p =.007 Calf 1530 Calf 1530 Proximal 16.")
162
Thromboembolism Knee Procedure AsymmetricalCircumferential Compression Compression Compression Compression Unilateral, primary Unilateral, primary Knees 155 158 Thrombi 13 (8.4%) 26 (15.8%) p = 0.03 Thrombi 13 (8.4%) 26 (15.8%) p = 0.03 Bilateral, primary Patients (knees) 25 (50) 22 (44) Patients-thrombi 1 (4%) 5 (22.7%) p = 0.09 Limbs-thrombi 2 (4%) 7 (15.9%) p = 0.05 Limbs-thrombi 2 (4%) 7 (15.9%) p = 0.05
 26 (15.8%) p = 0.03 Thrombi 13 (8.4%) 26 (15.8%) p = 0.03 Bilateral, primary Patients (knees) 25 (50) 22 (44) Patients-thrombi 1 (4%) 5 (22.7%) p = 0.09 Limbs-thrombi 2 (4%) 7 (15.9%) p = 0.05 Limbs-thrombi 2 (4%) 7 (15.9%) p = 0.05")
163
Personal TKA Series Calf IPC Plus Aspirin Personal TKA Series Calf IPC Plus Aspirin 856 TKAs Mortality (MI) 1 (0.12%) Symptomatic PE 3 (0.35%) DVT (Duplex) 66 (7.7%) (56 pts) 1991 - present
 1 (0.12%) Symptomatic PE 3 (0.35%) DVT (Duplex) 66 (7.7%) (56 pts) present")
164
Multimodal Prophylaxis TKA Venaflow ® + LMWH vs. Venaflow ® + Aspirin Prospective, randomized Prospective, randomized 275 unilateral TKAs 275 unilateral TKAs Duplex scan 3-5 days; 4-6 weeks Duplex scan 3-5 days; 4-6 weeks DVT 14.1% vs 17.8% (p = 0.27) DVT 14.1% vs 17.8% (p = 0.27) No difference between groups! No difference between groups! Westrich et al. J. Arthroplasty 2006
 DVT 14.1% vs 17.8% (p = 0.27) No difference between groups. No difference between groups. Westrich et al. J. Arthroplasty")
165
VTED Prophylaxis TKA What is Acceptable in 2007 Mechanical prophylaxis plus aspirin is safe and effective for most TKA patients Mechanical prophylaxis plus aspirin is safe and effective for most TKA patients Recommend rapid-inflation, asymmetric calf compression device Recommend rapid-inflation, asymmetric calf compression device Anticoagulation for patients allergic to aspirin or with heritable coagulopathy Anticoagulation for patients allergic to aspirin or with heritable coagulopathy Multimodal prophylaxis is an acceptable alternative to ACCP Guidelines Multimodal prophylaxis is an acceptable alternative to ACCP Guidelines

166
Anticoagulation and the Orthopedic Patient: the Anesthesiologists Perspective Eugene R Viscusi, MD Director, Acute Pain Management Associate Professor Department of Anesthesiology Thomas Jefferson University, Philadelphia, PA

167
Overview Venous thromboembolism (VTE), DVT and PE are real and significant threats to the orthopedic patient Venous thromboembolism (VTE), DVT and PE are real and significant threats to the orthopedic patient The anesthesia and analgesia plan must accommodate treatment of VTE The anesthesia and analgesia plan must accommodate treatment of VTE Anesthesia and pain management can be challenging and pose risks to the patient in the absence of communication and cooperation between care teams Anesthesia and pain management can be challenging and pose risks to the patient in the absence of communication and cooperation between care teams
, DVT and PE are real and significant threats to the orthopedic patient Venous thromboembolism (VTE), DVT and PE are real and significant threats to the orthopedic patient The anesthesia and analgesia plan must accommodate treatment of VTE The anesthesia and analgesia plan must accommodate treatment of VTE Anesthesia and pain management can be challenging and pose risks to the patient in the absence of communication and cooperation between care teams Anesthesia and pain management can be challenging and pose risks to the patient in the absence of communication and cooperation between care teams")
168
The 2004 ACCP recommendations further increased the level and duration of thromboprophylasis. Despite the reduction of asymptomatic thromboembolic events, an actual reduction of clinically relevant events has been difficult to demonstrate 1,2 The 2004 ACCP recommendations further increased the level and duration of thromboprophylasis. Despite the reduction of asymptomatic thromboembolic events, an actual reduction of clinically relevant events has been difficult to demonstrate 1,2 These changes create new challenges for managing neuraxial and invasive non- compressible peripheral blockade These changes create new challenges for managing neuraxial and invasive non- compressible peripheral blockade 1. Murray DW, et al. J Bone Joint Surg. 1996;78:863-870. 2. Mantilla CB, et al. Anesthesiology. 2002;96:1140-1146. Overview

169
The ACCP guidelines and the ASRA consensus statement on neuraxial techniques often leave the clinician in the zone of discomfort: The ACCP guidelines and the ASRA consensus statement on neuraxial techniques often leave the clinician in the zone of discomfort: l Both statements provide important clinical information but dont address all situations l ASRA guidelines are based on knowledge of the agents and past adverse events rather than large studies. (Difficult to provide the denominator) The Challenge
 The Challenge.")
170
2004 ACCP Recommendations Unfractionated heparin every 8 hours Unfractionated heparin every 8 hours l No data documenting safety of neuraxial catheters; complicates catheter removal Fondaparinux following major orthopedic surgery Fondaparinux following major orthopedic surgery l ASRA recommends against epidural catheter Warfarin; target INR for TJA is 2.5 Warfarin; target INR for TJA is 2.5 l If achieved would preclude epidural catheters Chest. Sept 2004, supp

171
2004 ACCP Recommendations Dosing of LMWH early in the postoperative period was associated with an increased risk of neuraxial bleeding Dosing of LMWH early in the postoperative period was associated with an increased risk of neuraxial bleeding Anticoagulate a minimum of 10 days; 28-35 for total hip Anticoagulate a minimum of 10 days; 28-35 for total hip l Interaction of prolonged thromboprophylaxis, neuraxial instrumentation, difficult or traumatic needle insertion is UNKNOWN

172
1,260,000 spinals; 450,000 epidurals 33 spinal hematomas 33 spinal hematomas l 24 in females, 25 with epidural l Coagulopathy in 11 Time of occurrence: 24 hours (6H-14D) Time of occurrence: 24 hours (6H-14D) 5 of 33 recovered (delay in treatment) 5 of 33 recovered (delay in treatment) 4 patients with indwelling epidural catheters received 5,000 U heparin during surgery 4 patients with indwelling epidural catheters received 5,000 U heparin during surgery Moen V, et al. Anesthesiology. 2004;101:950-959

173
Authors calculated risk for females undergoing TKA 1:3,600! (female, age, spinal canal pathology, duration of catheter, thromboprophylaxis) Authors calculated risk for females undergoing TKA 1:3,600! (female, age, spinal canal pathology, duration of catheter, thromboprophylaxis) One–third of all spinal hematomas occurred in patients receiving thromboprophylaxis in accordance with current guidelines One–third of all spinal hematomas occurred in patients receiving thromboprophylaxis in accordance with current guidelines Moen V, et al. Anesthesiology. 2004;101:950-959
 Authors calculated risk for females undergoing TKA 1:3,600. (female, age, spinal canal pathology, duration of catheter, thromboprophylaxis) One–third of all spinal hematomas occurred in patients receiving thromboprophylaxis in accordance with current guidelines One–third of all spinal hematomas occurred in patients receiving thromboprophylaxis in accordance with current guidelines Moen V, et al. Anesthesiology. 2004;101:")
174
Spinal Hematoma May occur in the absence of identifiable risk factors May occur in the absence of identifiable risk factors Neurological monitoring is critical for early intervention Neurological monitoring is critical for early intervention l Early recognition and treatment is key to improved outcome (laminectomy within 8 hours) 1 Focus not only on prevention but also improving neurological outcome Focus not only on prevention but also improving neurological outcome Vandermeulen ER, et al. Anesth Analg 1994:79:1165-77

175
Warfarin INR of less than 1.5 is recommended for removal of epidural catheters 1 INR of less than 1.5 is recommended for removal of epidural catheters 1 Check INR: Check INR: l Every day with an indwelling epidural catheter l Prior to needle insertion if given more than 36 hours prior 1. 2 nd ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation. Reg Anesth Pain Med. 2003;28:172-197.

176
Can Epidural Anesthesia and Warfarin be Coadministered? 1 Prudence must be exercised when enforcing these guidelines, both in the upper INR limit as well as potential reversal of anticoagulation 1 Prudence must be exercised when enforcing these guidelines, both in the upper INR limit as well as potential reversal of anticoagulation 1 l 11,235 patients: no detectable hematomas 1030 randomly reviewed charts: 398 patients had INR greater than 1.5 (1.54 mean, range 0.93-4.25)1030 randomly reviewed charts: 398 patients had INR greater than 1.5 (1.54 mean, range 0.93-4.25) 1. Parvizi J, Viscusi ER. CORR, 2007( in press)
1030 randomly reviewed charts: 398 patients had INR greater than 1.5 (1.54 mean, range ) 1. Parvizi J, Viscusi ER. CORR, 2007( in press).")
177
If the INR is elevated, should anticoagulation be reversed? If the INR is elevated, should anticoagulation be reversed? l Pulmonary embolism is a serious risk l FFP is not without risk in itself Decision should be taken case by case and the thought process fully documented! Decision should be taken case by case and the thought process fully documented! Can Epidural Anesthesia and Warfarin be Coadministered? 1 1. Parvizi J, Viscusi ER. CORR, 2007( in press)
.")
178
Standard (Unfractionated) Heparin BID dosing is theoretically safe if catheter removal is timed with trough levels BID dosing is theoretically safe if catheter removal is timed with trough levels TID dosing: no data exists but PTT (anecdotally) may remain elevated TID dosing: no data exists but PTT (anecdotally) may remain elevated Heparin induced thrombocytopena (HIT) is a real concern Heparin induced thrombocytopena (HIT) is a real concern l Platelet count is indicated after 5 days of unfractionated heparin
 Heparin BID dosing is theoretically safe if catheter removal is timed with trough levels BID dosing is theoretically safe if catheter removal is timed with trough levels TID dosing: no data exists but PTT (anecdotally) may remain elevated TID dosing: no data exists but PTT (anecdotally) may remain elevated Heparin induced thrombocytopena (HIT) is a real concern Heparin induced thrombocytopena (HIT) is a real concern l Platelet count is indicated after 5 days of unfractionated heparin")
179
Standard Heparin and Regional Anesthesia No contraindication following subcutaneous injection prior to spinal/epidural needle insertion No contraindication following subcutaneous injection prior to spinal/epidural needle insertion Delay administration for one hour following needle placement Delay administration for one hour following needle placement Remove indwelling catheter at trough level or one hour prior to next dose Remove indwelling catheter at trough level or one hour prior to next dose Prolonged therapy is linked to increase in spinal hematoma Prolonged therapy is linked to increase in spinal hematoma Traumatic needle insertion may increase risk of spinal hematoma Traumatic needle insertion may increase risk of spinal hematoma ASRA consensus guidelines

180
LMWH Restrict to once daily dosing regimen with epidural catheter Restrict to once daily dosing regimen with epidural catheter LMWH dosing minimum of 2 hours after catheter removal LMWH dosing minimum of 2 hours after catheter removal Spinal hematomas have been reported with this regimen; (The last chapter hasnt been written) Spinal hematomas have been reported with this regimen; (The last chapter hasnt been written) ASRA consensus guidelines
 Spinal hematomas have been reported with this regimen; (The last chapter hasnt been written) ASRA consensus guidelines")
181
Consider the risk/benefit ratio of thromboembolic event vs. spinal hematoma Consider the risk/benefit ratio of thromboembolic event vs. spinal hematoma Timing: With once daily dosing, time epidural catheter removal in a safe window before next dose Timing: With once daily dosing, time epidural catheter removal in a safe window before next dose l Minimize delay of next dose Renal function affects metabolism of LMWH (and other drugs). Elderly at particular risk. Dose accordingly 1 Renal function affects metabolism of LMWH (and other drugs). Elderly at particular risk. Dose accordingly 1 DSousa G, Viscusi ER. ASA 2006 (abstract) LMWH
. Elderly at particular risk. Dose accordingly 1 Renal function affects metabolism of LMWH (and other drugs). Elderly at particular risk. Dose accordingly 1 DSousa G, Viscusi ER. ASA 2006 (abstract) LMWH.")
182
Antiplatelet Medications Uncommon as primary agents for thromboprophylaxis but may be used chronically by orthopedic patients 1 Uncommon as primary agents for thromboprophylaxis but may be used chronically by orthopedic patients 1 l A number of large studies demonstrated relative safety l However, if this is combined with heparin there may be increased (but unquantified) risk Horlocker T, Wedel D. Anesth Analg 1995;80:303-309

183
Platelet Aggregation Inhibitors Interfere with platelet-fibrinogen binding and platelet-platelet interaction Interfere with platelet-fibrinogen binding and platelet-platelet interaction l Ticlopidine: stop 14 days l Clopidogrel: stop 7 days Platelet glycoprotein IIb/IIIa receptor antagonists Platelet glycoprotein IIb/IIIa receptor antagonists l 48 hours: abciximab l 8 hours eptifibatide, tirofiban ASRA consensus guidelines

184
Fondaparinux Factor Xa inhibitor with half-life of 21 hours 1 Factor Xa inhibitor with half-life of 21 hours 1 Clinical trials: Clinical trials: l Atraumatic epidural needle placement l Epidural catheter removed 2 hours prior to dosing Avoid indwelling epidural catheters with this drug Avoid indwelling epidural catheters with this drug Turpie AG et al.[Letter]NEJM. 2001; 345:292
![Fondaparinux Factor Xa inhibitor with half-life of 21 hours 1 Factor Xa inhibitor with half-life of 21 hours 1 Clinical trials: Clinical trials: l Atraumatic epidural needle placement l Epidural catheter removed 2 hours prior to dosing Avoid indwelling epidural catheters with this drug Avoid indwelling epidural catheters with this drug Turpie AG et al.[Letter]NEJM.](http://images.slideplayer.com/1/678021/slides/slide_184.jpg "2001; 345:292.")
185
Recommendations for Safety with Neuraxial Techniques Know the ASRA guidelines Know the ASRA guidelines Employ single agent anticoagulation Employ single agent anticoagulation Understand risks of each individual agent Understand risks of each individual agent Follow developments with peripheral nerve blocks Follow developments with peripheral nerve blocks Careful monitoring of dose timing, coagulation studies and neurologic function are critical Careful monitoring of dose timing, coagulation studies and neurologic function are critical Atraumatic needle placement if possible Atraumatic needle placement if possible

186
Analgesic Techniques: Hip Intrathecal Morphine Intrathecal Morphine Lumbar Plexus Block Lumbar Plexus Block l Single injection or continuous catheter Epidural Analgesia Epidural Analgesia l Single injection, standard morphine l Extended-release Epidural Morphine l Indwelling epidural catheter

187
Femoral Block Femoral Block l Single injection or catheter Lumbar plexus (posterior approach) Lumbar plexus (posterior approach) l Single injection or continuous catheter Epidural analgesia Epidural analgesia l Indwelling continuous catheter l Extended-release Epidural Morphine l Single injection standard morphine Analgesic Techniques: Knee
 Lumbar plexus (posterior approach) l Single injection or continuous catheter Epidural analgesia Epidural analgesia l Indwelling continuous catheter l Extended-release Epidural Morphine l Single injection standard morphine Analgesic Techniques: Knee")
188
Summary Safe and effective anesthesia and pain management for the orthopedic patient can be achieved in the presence of VTE prophylaxis when the entire care team (orthopedics, anesthesiology, nursing) understands the limitations, risks and works together Safe and effective anesthesia and pain management for the orthopedic patient can be achieved in the presence of VTE prophylaxis when the entire care team (orthopedics, anesthesiology, nursing) understands the limitations, risks and works together
 understands the limitations, risks and works together Safe and effective anesthesia and pain management for the orthopedic patient can be achieved in the presence of VTE prophylaxis when the entire care team (orthopedics, anesthesiology, nursing) understands the limitations, risks and works together")
Similar presentations












 www.ahrq.gov.>")




 Prophylaxis Policy Mary-Anne Davies Patient Safety Specialist Accreditation Coordinator.>")

>")


 recommended cardiac surgery patients, with.>")