Download presentation
Presentation is loading. Please wait.

1
Dr Kneale Metcalf Stroke Physician (NNUHFT)
Stroke Imaging Dr Kneale Metcalf Stroke Physician (NNUHFT)
")
2
Overview Modalities available When to use? Targets Real world imaging
Future aspirations

3
Hyperacute Stroke Diagnosis difficulties Patient stability issues
Vomiting Airway Low GCS Seizures

4
CT Scan First time every time Fast Safe Available
?? Posterior, late presentation Fast Safe ? Radiation Available

5
CT Scanner

6
Early CT scan Give Radiologist correct information
TIME of onset neurology Side and details of neurology Associated headache? Trauma? Anticoagulant? Relevant PMH Cancer Stroke Neurosurgery / clips etc.

7
Early CT scan Often normal Why do? Exclude haemorrhage Exclude tumour
Grade for thrombolysis risk

10
Dense Middle Cerebral Artery

12
Do early infarct signs matter?
Help confirm diagnosis Dense middle cerebral artery 10% chance opening with IV thromolysis ? May lead to intra-arterial or mechanical treatments Prognosis for thrombolysis 1/3 MCA territory

13
ASPECTS Canadian study Academic CT head interpretation
Leads to 10 point scoring system on plain axial CT head Scores of <7 increased functional dependence + increased risk of death

14
ASPECTS Scored from two axial slices 10 points
One at thalamic level / basal ganglia One just above ganglionic structures (such that none are seen) 10 points One subtracted for each area of early ischemic change (thus score 10=normal scan)
 10 points. One subtracted for each area of early ischemic change (thus score 10=normal scan)")
16
Core message Extensive early infarction may be poor prognostic indicator for outcome from thrombolysis

17
Intracerebral Haemorrhage
Main causes Hypertension Cerebral Amyloid Angiopathy (CAA) Rarities
 Rarities.")
20
Hypertensive bleed

21
Cerebral Amyloid Angiopathy

22
Can be more subtle

23
Core message Main causes of intracerebral haemorrhage are amyloid angiopathy and hypertension

24
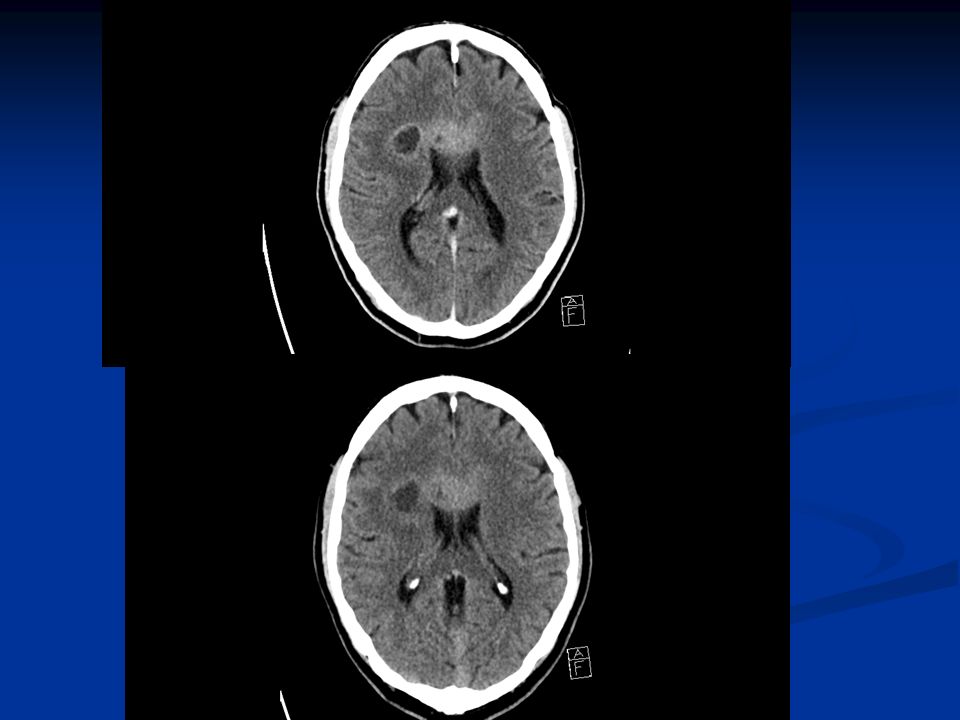
Tumour Can be subtle History review Plain CT may not show
Non acute onset Seizures Headache Cancer Plain CT may not show Contrast

25
Subtle sub-acute LEFT weakness

26
Post contrast

30
Brain tumours Often contrast enhance May have vasogenic oedema
May respect grey / white junction

31
Other mimics Subdural haematoma Sub arachnoid haemorrhage ++

32
Subdural haematoma

33
Sub arachnoid haemorrhage

34
Don’t miss mimics History just as important as the scan!

35
Timing of CT changes

36
Infarct

38
Haemorrhage

39
Haemorrhage

40
Core message After days both haemorrhage and infarct both look like a black hole Important to be able to distinguish old from new infarcts

41
Urgent Scans % of URGENT scans performed within 60mins of arrival to hospital (Best Prac + NICE quality standard) 90% by April 2011 Best practice = scan + report

42
What are indications for an urgent scan?
GCS <13 On Warfarin Bleeding tendency Severe headache Papilloedema / neck stiff / fever Progressive / fluctuating symptoms For thrombolysis

43
MRI scan

44
Why do an MRI? If stroke uncertain To confirm vascular territory
Look for multi-territory involvement Look for previous haemorrhage

45
Main MRI sequences Diffusion

46
Main MRI sequences Gradient-echo (T2*)
")
47
CT Perfusion Concept of ischaemic pemumbra

48
CT Perfusion Cerebral blood volume Cerebral blood flow Mismatch

49
CT Perfusion Wake up strokes Large strokes Timing questions Mimics

50
Future More CT Perfusion More MRI
Movement towards acute arterial imaging

51
Summary Brain imaging from Stroke Physician perspective
Targets – why + how Where imaging may go

Similar presentations























 Angela Roots Angela Roots (Practice Development.>")
 July 2008.>")
 Sensitive indicator of perfusion Diagnosis and prognosis of.>")


