Download presentation
Presentation is loading. Please wait.

1
The European Society’s HERMES Project, a Model to Emulate Francesco Blasi Department Pathophysiology and Transplantation, University of Milan, Italy

2
Disclosures I have accepted grants, speaking and conference invitations from Almirall, Angelini, AstraZeneca, Bayer, Chiesi, GSK, Guidotti-Malesci, Menarini, Novartis, Pfizer, and Zambon I have had recent or ongoing consultancy with Almirall, Angelini, AstraZeneca, GSK, Menarini, Mundipharma and Novartis

3
What is HERMES? Harmonised Education in Respiratory Medicine for European Specialists

4
Harmonised Training standards across the European Union Recognition of diplomas and certificates of qualification in medicine in EU Free access and mobility for European medical specialists MISSION OF THE HERMES INITIATIVE

5
EU CONTEXT: FREE ACCESS AND MOBILITY EU mutual recognition of diplomas and certificates of qualification in medicine in all member countries EU parliament 2013 modernised the 2005 directive (Directive 2013/55/EU) –Modernisation of the definition for harmonised minimum training requirements for professions which benefit from automatic recognition –For example for doctors, modernised directive clarifies that the basic medical education ought to be based on 5’500 training hours done within a minimum of 5 years
 –Modernisation of the definition for harmonised minimum training requirements for professions which benefit from automatic recognition –For example for doctors, modernised directive clarifies that the basic medical education ought to be based on 5’500 training hours done within a minimum of 5 years")
6
EUROPEAN PROFESSIONAL QUALIFICATIONS LANDSCAPE AND PLAYERS Postgraduate Specialist Training Universities Training Centres Training Centre Networks Certification National authorities HERMES UEMS central UEMS section of pneumology EAP/Section of Paediatrics Other sections (ICM, Thoracic Surgery, Oncology) Continuing Medical Education National authorities/ regulatory boards EBAP EACCME
 Continuing Medical Education National authorities/ regulatory boards EBAP EACCME")
7
Adult Respiratory Medicine (2005) Paediatric Respiratory Medicine (2008) Spirometry (2009) Respiratory Sleep Medicine (2009) Respiratory Critical Care (2010) Thoracic Oncology (2011) Physiotherapy (2012) Thoracic Surgery (2014) Respiratory Infections (2014) HERMES Task Forces 2005-2014
 Paediatric Respiratory Medicine (2008) Spirometry (2009) Respiratory Sleep Medicine (2009) Respiratory Critical Care (2010) Thoracic Oncology (2011) Physiotherapy (2012) Thoracic Surgery (2014) Respiratory Infections (2014) HERMES Task Forces")
8
Preliminary Phase Phase 4Phase 3 Phase 2Phase 1 Core Syllabus Completed Sept 06 Standards for Training Centres (not started) European Exam First Oct 08 Core Curriculum Completed Sept 08 HERMES Project
 European Exam First Oct 08 Core Curriculum Completed Sept 08 HERMES Project")
9
Preliminary Phase Phase 4Phase 3 Phase 2Phase 1 Core Syllabus Completed Sept 06 Standards for Training Centres (not started) European Exam First Oct 08 Core Curriculum Completed Sept 08 HERMES Project
 European Exam First Oct 08 Core Curriculum Completed Sept 08 HERMES Project")
13
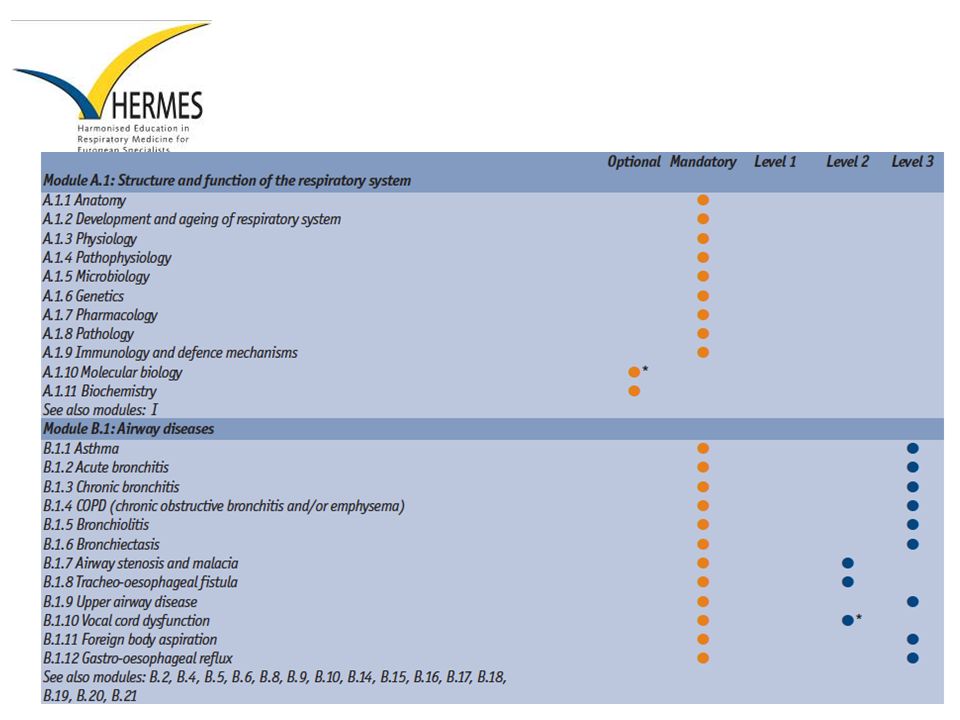
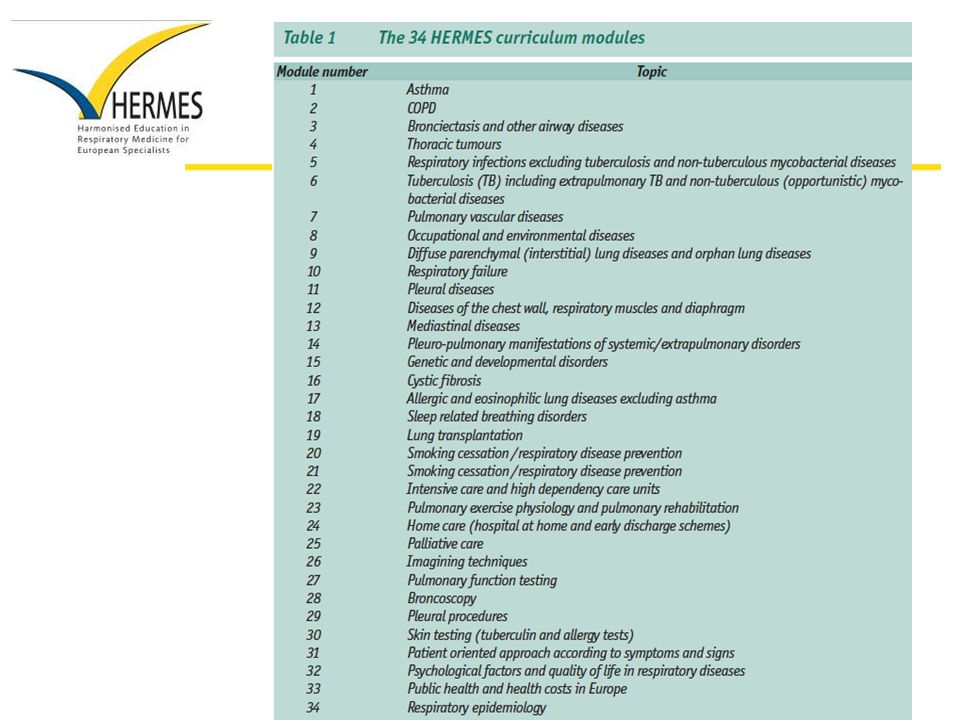
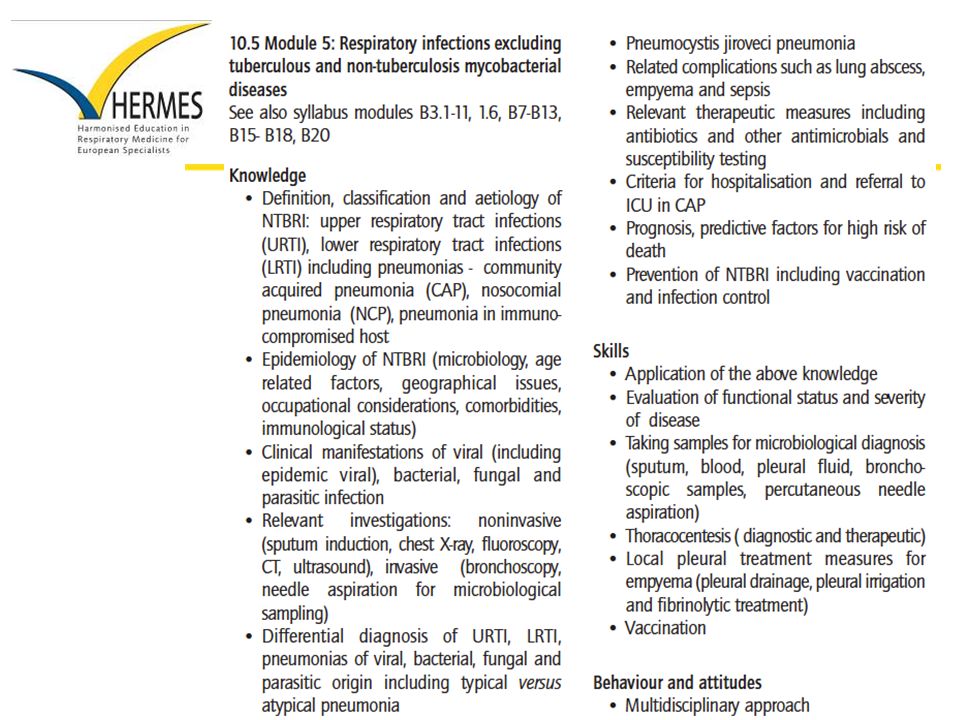
What does the Examination look like? Knowledge-based only Paper-based multiple-choice questionnaire (MCQ) in English; 90 questions; 3 hrs Blueprint for the content of the examination is the consensus-based European syllabus (Breathe 2006; 3: 59-70) available in 24 languages at: http://hermes.ersnet.org/452-syllabus-dissemination.htm
 in English; 90 questions; 3 hrs Blueprint for the content of the examination is the consensus-based European syllabus (Breathe 2006; 3: 59-70) available in 24 languages at:")
14
What does the Examination look like?

15
Why take a European Examination? Proof of Excellence: to demonstrate to patients and colleagues your commitment to high-quality life-long learning Mobility: if moving to another country, the European Diploma will certainly be known and recognised within the profession Self-assessment: you may wish to find out where you stand against the current European standard Tangible recognition: European Diploma and membership of ERS School Diplomate Club Advantages for the individual:

16
The European Diploma in Adult Respiratory Medicine Re-validation: To comply with European Curriculum recommendations (Breathe Sept 2008; volume 5, number 1), candidates are advised to voluntarily re-sit the European Examination every 5 years to demonstrate that their knowledge is up-to-date. It is mandatory to re-sit the Examination every 10 years or the right to hold the Diploma will lapse.

17
SIMER INTERNATIONAL SCHOOL - Lectures Review of current guidelines - Interactive sessions MCQ Clinical Cases

18
SIMER INTERNATIONAL SCHOOL A 24-year-old woman has had a long-standing mild, persistent asthma for which she has been using approximately four puffs (44 mcg/puff) per day od inhaled fluticasone and approximately two to four puffs of albuterol per week with good results. However, approximately 6 months ago, she and her husband bought and moved into a new house, which they are living in and slowly renovating. Although the main triggers to her asthma are believed to be cats and ragweed, she has noted a deterioration in her asthma since they moved in, despite multiple steps to limit her potential exposure to dust and mold during renovations. She has continued her fluticasone at the same dose but is now using two puffs of albuterol four to six times per day. She awakens because of asthma symptoms approximately once per week, and although she has not curtailed her regular activities, she reports feeling “more winded than usual”. Physical examination results are notable only for rare scattered wheezes on exhalation. FEV1 is 2.99 L (74% predicted), and FVC is 4.69 (98% predicted): the flow-volume loop shows mild expiratory coving. Assuming that no additional opportunities for trigger avoidance are identified, what is the most appropriate next step in her pharmacologic management? A.Add a long-acting B-agonist to her current dose of inhaled fluticasone B.Add montelukast to her current dose of inhaled fluticasone C.Add omalizumab therapy to her current dose of inhaled fluticasone D.Change her dose of inhaled fluticasone to four puffs bid of the 220 mcg/puff
, and FVC is 4.69 (98% predicted): the flow-volume loop shows mild expiratory coving. Assuming that no additional opportunities for trigger avoidance are identified, what is the most appropriate next step in her pharmacologic management. A.Add a long-acting B-agonist to her current dose of inhaled fluticasone B.Add montelukast to her current dose of inhaled fluticasone C.Add omalizumab therapy to her current dose of inhaled fluticasone D.Change her dose of inhaled fluticasone to four puffs bid of the 220 mcg/puff.")
19
SIMER INTERNATIONAL SCHOOL 12-15 December 2011

20
Existing country collaborations ADULT Switzerland Netherlands Russia Spain Portugal Austria Ireland PAEDIATRIC UK

21
ACCREDITATION

22
Feedback collated from centres The opportunity to be part of a Pan-European network of centres To benchmark trainee facilities and educational opportunities To receive recommendations on how to improve To present to the national ministry of health (for example) any basic standards not met which will justify requests for additional budget for training and facilities FROM AN ERS PERSPECTIVE Bridge the gap between European criteria and local implementation
 any basic standards not met which will justify requests for additional budget for training and facilities FROM AN ERS PERSPECTIVE Bridge the gap between European criteria and local implementation")
23
ACCREDITATION STEPS Step 1 Qualification for Accreditation Qualification based on ERS Criteria for Accreditation Document Step 2 Site Visit and Accreditation Accreditation based on monitoring and implementation of ERS criteria for accreditation

24
EDUCATIONAL RESOURCES

25
ERS HANDBOOKS ERS Handbook Series – 2 nd edition Respiratory Medicine – Respiratory Sleep Medicine – Self-Assessment in Respiratory Medicine – Paediatric Respiratory Medicine

26
HERMES Publications HERMES Adult BookletHERMES Paediatric Booklet

27
Accreditation of Training Centres Assessments Preliminar y Phase Syllabus HERMES Project Phases Continuous Professional Development and accreditation Curriculum Analysis of training & certification Analysis of training gap Educational Resources Published Outputs Phase 1 & 2 Phase 3, 4 and 5 Standards and Frameworks Adult Respiratory Medicine, Paediatric Respiratory Medicine. Multidisciplinary groups eg Respiratory Critical Care, Respiratory Sleep medicine, Thoracic Oncology, incorporation of skills assessment in addition to knowledge based assessment (HERMES Exam + portfolio), involvement of AHPs, scientists and trained staff Applicability and acceptability of standards
, involvement of AHPs, scientists and trained staff Applicability and acceptability of standards.")
28
CONTINUOUS PROCESSES CONSIDERED Consolidation Unifying processes and ensure robust methodology Investigation of outcomes on how standards are used Strategies of implementation Value of criteria and how they impact training and the healthcare system Linkages CME/CPD opportunities Based on HERMES standards (syllabi, curricula, accreditation criteria etc) UEMS and other EU entities Other ERS committees (guidelines, scientific etc) EBAP Other professional associations Training centres/networks Other local/national authorities
 UEMS and other EU entities Other ERS committees (guidelines, scientific etc) EBAP Other professional associations Training centres/networks Other local/national authorities")
29
CHALLENGES

30
Promoting state-of-the-art medical education (curriculum development, assessments, teaching and learning etc) Differences in acceptability and applicability of the recommendations in different countries Applicability Acceptability Finding the balance
 Differences in acceptability and applicability of the recommendations in different countries Applicability Acceptability Finding the balance ")
31
HERMES CHALLENGES Translation (different languages) of educational standards and assessments Different lengths of training across EU countries Different organisation of training across EU countries Legal aspects of practice in various fields Availability of resources in different countries for training Legal adoption of educational standards and assessments Models of collaboration for accreditation (individuals, centres and networks)
 of educational standards and assessments Different lengths of training across EU countries Different organisation of training across EU countries Legal aspects of practice in various fields Availability of resources in different countries for training Legal adoption of educational standards and assessments Models of collaboration for accreditation (individuals, centres and networks)")
32
PRIORITIES

33
HERMES PRIORITIES Consolidation of HERMES projects Development of processes for implementation of educational standards Scientific approach with the processes involved (including Delphi technique and measurements) Development of the HERMES initiative as a European/regional approach Developing CME/CPD standards for trained specialists Exploration of legal aspects
 Development of the HERMES initiative as a European/regional approach Developing CME/CPD standards for trained specialists Exploration of legal aspects")
34
RIGOROUS VALIDATION and COMMITMENT in formulating the educational standards through robust methodologies in medical education.

35
THE TRANSNATIONAL NATURE OF THE HERMES INITIATIVE HIGHLIGHTS AND ADDRESSES THE CURRENT TREND OF MOBILITY AMONG SPECIALISTS AND PATIENTS WITHIN EUROPE.

36
THANK YOU FOR YOUR ATTENTION !

Similar presentations



 in Europe. It operates through a Council,>")





>")









