Download presentation
Presentation is loading. Please wait.

1
Novel Therapies for Myeloma A. Keith Stewart Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Disclosure of Potential Conflicts of Interest Honoraria: Celgene, Millenium Research grants: Millenium Consultant: Proteolix

2
A “Gold Rush” in Myeloma Pre-clinical Drug Testing >200 drugs reported in preclinical studies (~$30,000,000)
")
3
>200 drugs reported in preclinical studies ~30 - 40 trial results reported 3 agents with known significant single agent activity – all arise from known active drug classs

4
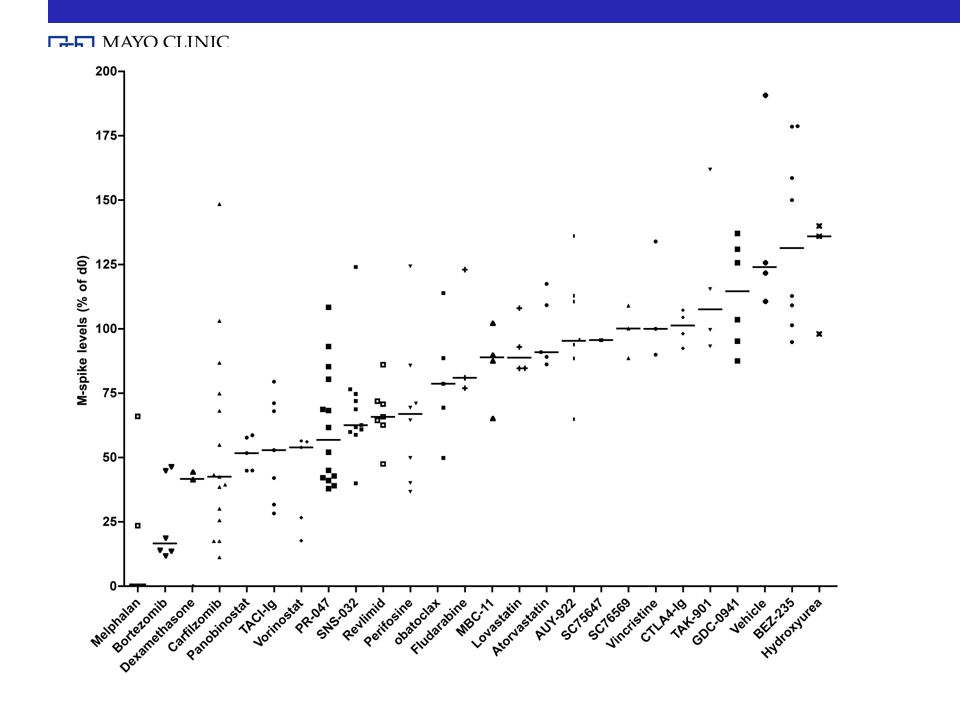
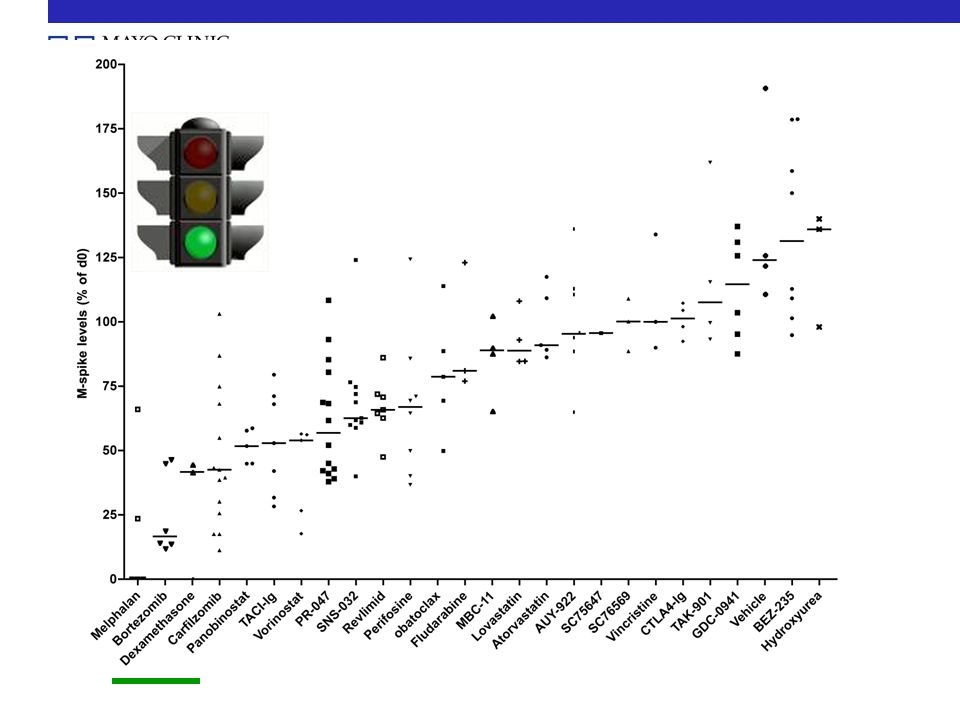
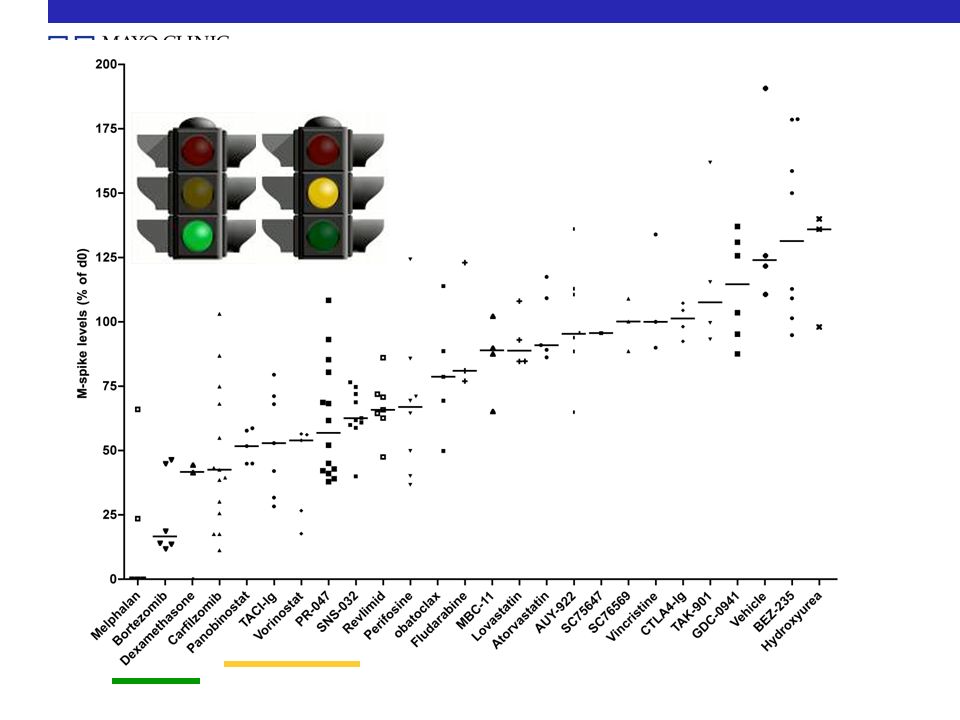
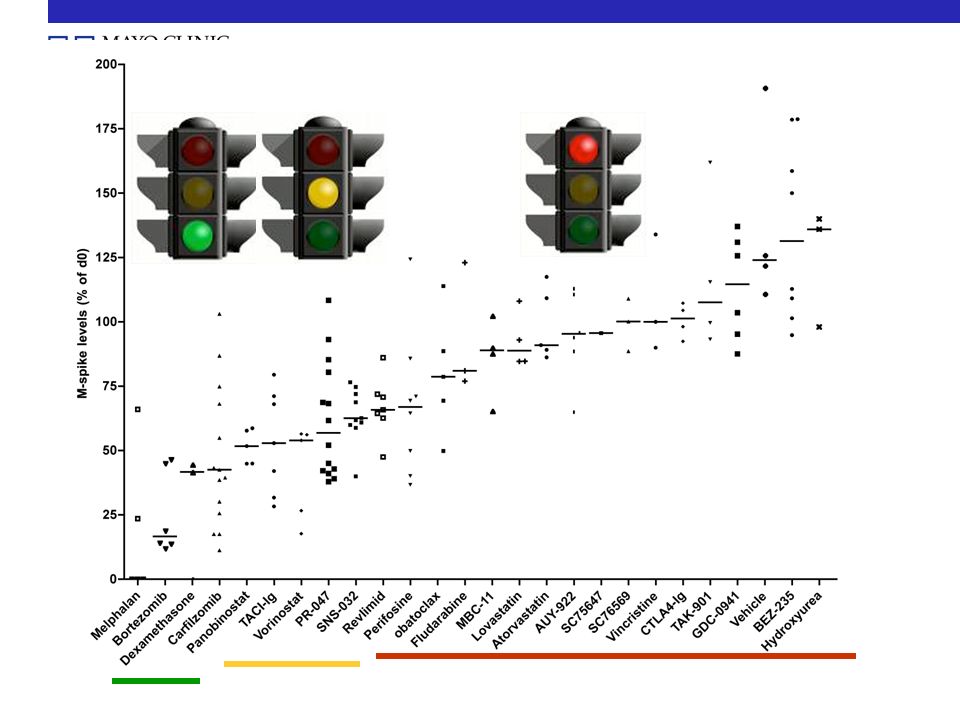
Single Agent Activity of 39 Drugs Tested in Myeloma

5
Active Drugs Single Agent Activity of 39 Drugs Tested in Myeloma Inactive Drugs

6
Pomalidomide (CC4047) plus low-dose dexamethasone (Pom/Dex) is highly effective therapy in relapsed multiple myeloma MQ Lacy, S Hayman, M Gertz, J Allred, S Mandrekar, A Dispenzieri, S Zeldenrust, S Kumar, P Greipp, J Lust, S Russell, F Buadi, R Kyle, PL Bergsagel, R Fonseca, V Roy, J Mikhael, AK Stewart, and SV Rajkumar Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
 plus low-dose dexamethasone (Pom/Dex) is highly effective therapy in relapsed multiple myeloma MQ Lacy, S Hayman, M Gertz, J Allred, S Mandrekar, A Dispenzieri, S Zeldenrust, S Kumar, P Greipp, J Lust, S Russell, F Buadi, R Kyle, PL Bergsagel, R Fonseca, V Roy, J Mikhael, AK Stewart, and SV Rajkumar Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida")
7
Molecular Structure of Thalidomide, Lenalidomide and Pomalidomide Lenalidomide 15-25 mg/d Myelosuppression Skin rash DVT Structurally similar, but functionally different both qualitatively and quantitatively Thalidomide 100-200 mg/d Neuropathy Constipation Sedation DVT Pomalidomide 1-4 mg/d N O O N H O O NH 2

8
Study design & treatment Phase II trial, 60 patients A confirmed response is defined to be a CR, PR or VGPR as assessed by the International Myeloma Working Group Uniform Response criteria. Starting Dose: Pomalidomide - 2mg p.o. daily days 1-28 Dexamethasone - 40mg p.o. days 1, 8, 15 & 22 Aspirin - 325mg p.o. days 1-28

9
Response N =60 CR3 (5%) VGPR17 (28%) PR18 (30%) SD15 (25%) PD6 (10%) NE1 (2%) ORR 63% CR +VGPR 33% Best Response Median follow-up 7 months
 VGPR17 (28%) PR18 (30%) SD15 (25%) PD6 (10%) NE1 (2%) ORR 63% CR +VGPR 33% Best Response Median follow-up 7 months")
10
Responses in patients refractory to other novel agents Refractory to NCRVGPRPRSDPDRR* Bortezomib101 (10%)2 (20%)3 (30%)4 (40%)06 (60%) Lenalidomide2001 (5%)7 (35%)9 (45%)3 (15%)8 (40%) Thalidomide1602 (12.5%)4 (25%)6 (37.5%)4 (25%)6 (37.5%)
2 (20%)3 (30%)4 (40%)06 (60%) Lenalidomide2001 (5%)7 (35%)9 (45%)3 (15%)8 (40%) Thalidomide1602 (12.5%)4 (25%)6 (37.5%)4 (25%)6 (37.5%)")
11
M-spike 3.5 CRD started Relapsing on CRD Bortezomib M-spike 2.6 Bortezomib Melphalan, Pred Pom/dex, M-spike 2.9 Patient 2, 67 year old female

12
Conclusions The combination of pomalidomide and low dose dexamethasone is highly active in the treatment of relapsed/refractory multiple myeloma. Toxicity has been manageable and consists primarily of myelosuppression with neutropenia. Future directions include phase II trial of pomalidomide and dexamethasone for lenalidomide-refractory and bortezomib – refractory patients

13
Updated Results of Bortezomib-Naïve Patients in PX-171-004, An Open-Label, Phase 2 Study of Single-Agent Carfilzomib in Patients with Relapsed or Refractory Multiple Myeloma Luhua Wang, MD, David Siegel, MD, Jonathan L. Kaufman, MD, Keith Stewart, MD, Andrzej J. Jakubowiak, MD, PhD, Melissa Alsina, MD, Vishal Kukreti, MD, FRCPC, Nizar J Bahlis, MD, Kevin T. McDonagh, MD, Andrew Belch, MD, Michael Sebag, MD, PhD, Nashat Gabrail,MD, Mai H. Le, MD, Mark K Bennett, PhD, Lori Kunkel, MD, Michael Kauffman, MD, PhD, Robert Z Orlowski, M.D., Ph.D., Ravi Vij, MD and The Multiple Myeloma Research Consortium (MMRC)
.")
14
Carfilzomib: Carfilzomib is a new, selective and irreversible proteasome inhibitor with pre-clinical anti-tumor activity. Responses seen in Phase I Myeloma trials. Ketoepoxide Tetrapeptide

15
% proteasome inhibition D8 D9 0 Week: D15 D16 123 28-day cycle 80 D1 D2 Rest period (12 days) 4 *IMWG response criteria PX-171-004 Carfilzomib Phase 2 Study Design Population: Multiple Myeloma, relapsed after 1-3 prior therapies CFZ administration: 20 mg/m 2 IV bolus; maximum 12 cycles Premedication: Hydration, Dexamethasone 4 mg during Cycle 1 Primary endpoint: Overall response rate (ORR = CR + VGPR + PR)* Secondary endpoints: DOR, PFS, TTP, OS, Safety QDx2 weekly for 3 weeks
 4 *IMWG response criteria PX Carfilzomib Phase 2 Study Design Population: Multiple Myeloma, relapsed after 1-3 prior therapies CFZ administration: 20 mg/m 2 IV bolus; maximum 12 cycles Premedication: Hydration, Dexamethasone 4 mg during Cycle 1 Primary endpoint: Overall response rate (ORR = CR + VGPR + PR)* Secondary endpoints: DOR, PFS, TTP, OS, Safety QDx2 weekly for 3 weeks")
16
Carfilzomib: Dose Escalation to 27 mg/m 2 N (%) Evaluable population 19 (100) CR0 (0) VGPR1 (5) PR9 (47) MR0 (0) SD6 (32) ≥SD : 84% ≥MR : 53% ≥PR : 53% ORR (> PR) = 53% Disease Control in 84%
 Evaluable population 19 (100) CR0 (0) VGPR1 (5) PR9 (47) MR0 (0) SD6 (32) ≥SD : 84% ≥MR : 53% ≥PR : 53% ORR (> PR) = 53% Disease Control in 84%")
17
PX-171-003: Response Summary (N=39) Seven subjects excluded from response analysis: Serum free light chain only (4) Received < 1 cycle of therapy (2) No baseline value (1) * 50% of responses occurred at 2 weeks
 Seven subjects excluded from response analysis: Serum free light chain only (4) Received < 1 cycle of therapy (2) No baseline value (1) * 50% of responses occurred at 2 weeks")
18
* All AEs reported in >25% patients 1 Includes both related and non-related Most Commonly Reported Adverse Events Adverse Event*, 1 Overall n (%) > Grade 3 n (%) Fatigue40 (68)7 (12) Nausea27 (46)0 (0) Dyspnea25 (42)3 (5) Cough22 (37)0 (0) Anemia21 (36)4 (7) Diarrhea18 (31)1 (2) Pyrexia18 (31)0 (0) Peripheral Edema18 (31)1 (2) Thrombocytopenia15 (25)7 (12) Upper Respiratory Infection 15 (25)1 (2) Data through Oct 2009
 > Grade 3 n (%) Fatigue40 (68)7 (12) Nausea27 (46)0 (0) Dyspnea25 (42)3 (5) Cough22 (37)0 (0) Anemia21 (36)4 (7) Diarrhea18 (31)1 (2) Pyrexia18 (31)0 (0) Peripheral Edema18 (31)1 (2) Thrombocytopenia15 (25)7 (12) Upper Respiratory Infection 15 (25)1 (2) Data through Oct 2009")
19
Peripheral Neuropathy is Infrequent and Mild Data through October 2009 There were no reports of Grade 4 peripheral neuropathy *Grade Based on physical assessment at screening (NCI-CTC scale) Only 1 patient was discontinued for peripheral neuropathy
 Only 1 patient was discontinued for peripheral neuropathy")
20
Carfilzomib Conclusions: Ph 2 Relapsed MM Single agent carfilzomib is highly active in relapsed patients –57% response rate in BTZ-naïve patients –26% CBR in Refractory disease CFZ achieves durable disease control with continued dosing –Median TTP 11.1 mos in BTZ-naïve patients –Median TTP 8.3 mos in BTZ-exposed patients Few > grade 3 Aes Peripheral neuropathy is not a treatment-limiting toxicity with CFZ

21
Dose escalation to 27 mg/m 2 Combination with Lenalidomide and Dexamethasone Registrational Development –single arm monotherapy Phase 2 in refractory pts completed –Randomized Phase 3 lenalidomide/dexamethasone +/- CFZ planned for 2010 Carfilzomib: Future Directions

22
Many drugs in trials – some current examples AUY922 TAK901 / MLN8237 CEP070 / MLN9708 TKI258 / MFGR1877S SCH727965 Panobinostat Monoclonals : CD38 BHQ880

23
t(4;14) 15% of Myeloma
 15% of Myeloma")
24
Hypothesis Pharmacologic abrogation of tyrosine kinase signaling by FGFR3 in MM cells will result in a tumour-specific cytotoxicity TKI-258 (Dovitinib) MFGR1877S
 MFGR1877S")
25
BM restricted plasmacytosis in Vk*MYC mice CD138 B220 wtVk*MYC spleen BM Chesi et al, Cancer Cell, February 2008

26
Monoclonal Protein %decrease from d=0 Day 0 14 0 14 0 14 0 14 0 14 MelphalanDexamethasoneBortezomibPlacebo { Revlimid

31
Conclusions Three new active drugs with many more being tested in clinical trials New Mouse models and target selection may result in higher success rate in clinic Future trials will likely focus on individualized therapy for different types of myeloma

Similar presentations












 with Newly Diagnosed Multiple Myeloma (NDMM) Receiving Lenalidomide and Low-Dose Dexamethasone.>")

 Inhibitor, Ibrutinib (PCI-32765), in Relapsed or Refractory.>")
 Induces High Rates.>")

: Results from the Expansion.>")
 for Newly Diagnosed Multiple Myeloma (MM) Patients: Initial Results of a Multicenter, Open Label.>")
