Download presentation
Presentation is loading. Please wait.

1
Perinatal HIV Screening in Colorado: Help Needed! Kay Kinzie MSN, FNP-C Pregnancy Coordinator Children’s Hospital Immunodeficiency Program

2
A Word About “CHIP” Existing since 1992 to care for HIV infected children, Pediatric AIDS Clinical Trials site After participation in PACTG 076 trial, increased involvement in maternal HIV screening and care Multidisciplinary team now caring for HIV positive children, youth, expectant mothers, and exposed newborns Contracted by Colorado Department of Health and Environment for resource on perinatal HIV testing.

3
HIV Transmission and Pathophysiology

4
HIV Transmission Mucosal/parenteral contact with infected: –Blood –Breast Milk –Semen –Vaginal Fluid

5
Symptoms of Acute Retroviral Syndrome Fever 96% Adenopathy 74% Pharyngitis 70% Rash 70% Myalgias 54% Diarrhea 32% Headache 32% N+V 27% Hepatomegaly, Splenomegaly 14% Weight Loss 13% Thrush 12% Neurologic 12%

6
Hematologic Events in Adult Acute HIV Retroviral Syndrome High viral replication Sharp initial decline in CD4 cells Development of HIV- specific antibodies – –6 weeks- 3 months – –“Window” period Viral “set point”

7
Early Asymptomatic HIV Disease in Adults 50% progression to AIDS within 8-10 years 5% “rapid progressors” 5% long term “non progressors” Long latency period ––A––Asymptomatic- “HIV Positive” ––A––Ability to infect other hosts

10
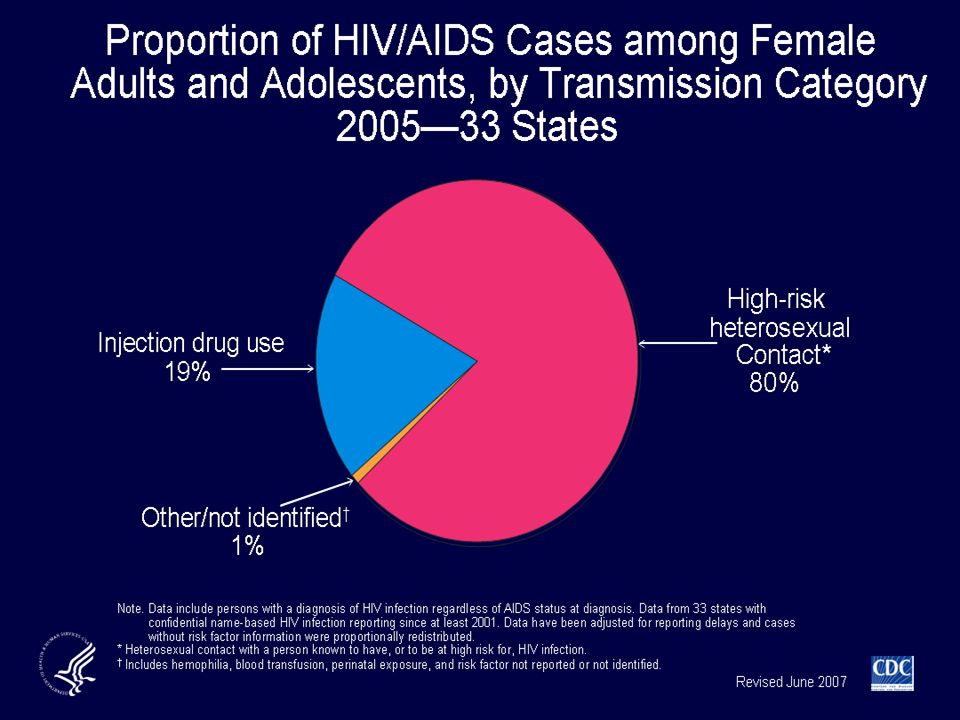
HIV/AIDS in Colorado Epidemiologic Profile CDPHE June 2004 Comparing Gender Characteristics AIDS 1985-1989 Female 5% Male 95% HIV 1999-2003 Female (196) 16% Male (1049) 84%
 16% Male (1049) 84%")
11
Demographics of HIV-infected Women who Delivered a Child in Colorado by Percent

12
Children Born to HIV-infected Women in Colorado by Area of Residence at Birth, Colorado 6/30/2006 30/64 counties had births to HIV infected women

13
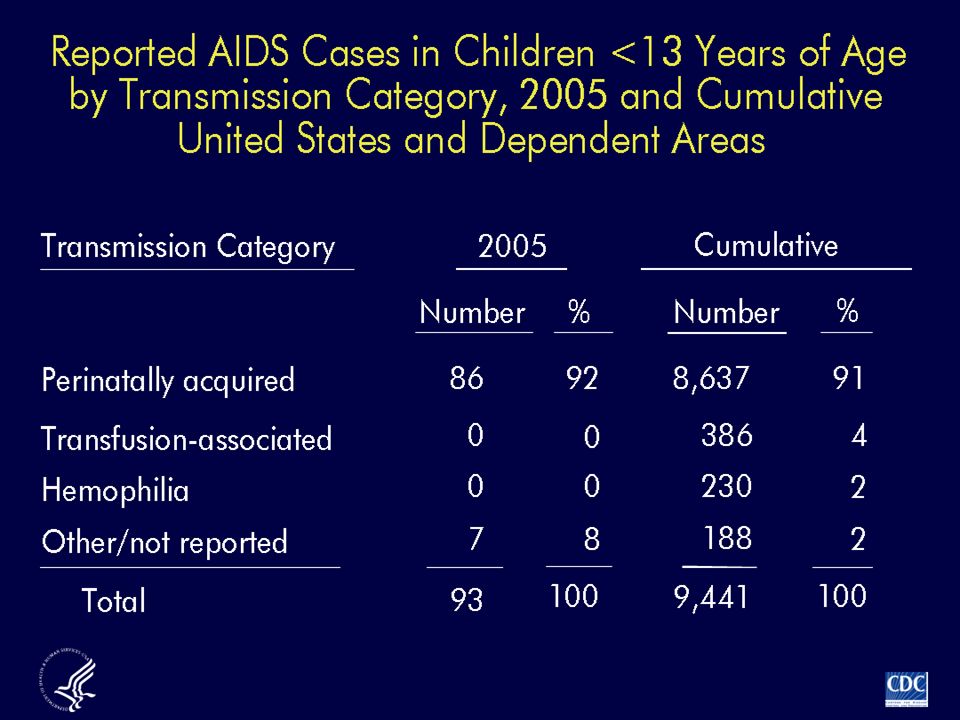
Pediatric HIV Infection > 92% due to vertical transmission –Acute Retroviral Syndrome superimposed on immature infant immune system –High levels of HIV viremia –Longer duration of viremia (years) before achievement of viral “set point” –20% of infants progress to AIDS within 4 years Median age at death 11 months PCP pneumonia- 50% mortality rate in infants
 before achievement of viral set point –20% of infants progress to AIDS within 4 years Median age at death 11 months PCP pneumonia- 50% mortality rate in infants")
15
Vertical (Mother to Child) HIV Transmission 25- 30% risk without treatment Timing –Antepartum 30% Acute retroviral syndrome or advanced disease –Intrapartum 70% Maternal-fetal microtransfusion Fetal mucous membrane or percutaneous exposure –Breastfeeding 16% Infection in early breastfeeding period, incremental risk with duration of nursing
 HIV Transmission % risk without treatment Timing –Antepartum 30% Acute retroviral syndrome or advanced disease –Intrapartum 70% Maternal-fetal microtransfusion Fetal mucous membrane or percutaneous exposure –Breastfeeding 16% Infection in early breastfeeding period, incremental risk with duration of nursing")
18
Strategies to Interrupt Vertical HIV Transmission Reduce maternal HIV viral load – –Antepartum maternal combination ARV Chemoprophylaxis of neonate – –Maternal intrapartum ARV meds Zidovudine, Nevirapine, others – –* Continue infant dosing until 6 weeks of age Reduce fetal/neonatal exposure to infected fluids – –Limit duration of ruptured maternal membranes (4 hrs) – –Limit invasive procedures (amnio, SVE, internal monitors) – –Elective C Section at 38 weeks – –Avoid breastfeeding
 – –Limit invasive procedures (amnio, SVE, internal monitors) – –Elective C Section at 38 weeks – –Avoid breastfeeding")
19
Rate of Perinatal HIV-1 Transmission by ARV Therapy Category ACTG 076ACTG 185French TrialWITSACTG 316 Placebo ZDV ZDV + 3TC No Rx ZDV Combo - PI Combo+ PI -NVP +NVP

20
Current estimated risk of vertical HIV transmission No therapy, vaginal delivery 25 % ZDV prophylaxis 5-8 % ZDV, elective Cesarean2% Undetectable viral load0.9% < 10,000 copies/ml+ C/S2% > 10,000 copies/ml+ C/S4.5% ACOG Technical Bulletin 8/99, ACTG case review 1998

21
Timing of ARV Prophylaxis is Linked to Infant Outcome Retrospective Epidemiologic Study 8/1/1995-1/1/1997 – –New York State – –939 infants with perinatal HIV exposure – –Moms with no prenatal care or chose to limit meds Wade, NA. Abbreviated regimens of zidovudine prophylaxis and perinatal transmission of the human immunodeficiency virus. NEJM 1998: 339 (20).
..")
22
Results Timing of AZTTransmission Rate Maternal Prenatal6.1 % (CI 4.1%-8.9%) Maternal Intrapartum10.0% (CI 3.3%-21.8%) Infant w/in 48 hrs9.3% (CI 4.1%-17.5%) Infant day 3 of life/ more18.4% (CI 7.7%-34%) No Prophylaxis26.6% (CI 21.1%-32.7%)
 Maternal Intrapartum10.0% (CI 3.3%-21.8%) Infant w/in 48 hrs9.3% (CI 4.1%-17.5%) Infant day 3 of life/ more18.4% (CI 7.7%-34%) No Prophylaxis26.6% (CI 21.1%-32.7%)")
23
The “Take Home” 92% of pediatric HIV result of vertical transmission With intervention, risk of vertical transmission can be reduced to < 1% Timing of interventions significantly affects infant outcomes: 48 hour window Effective maternal screening is key

24
Current Testing and Treatment Guidelines aidsinfo.nih.gov

25
Endorsements for Rapid Testing of Women with Unknown HIV Status at Labor/Delivery American College of Obstetrics and Gynecologists Centers for Disease Control, Department of Health and Human Services The Office of the Inspector General(OIG) in the Department of Health and Human Services Institute of Medicine (IOM) American Academy of Pediatrics Colorado Department of Public Health and Environment
 in the Department of Health and Human Services Institute of Medicine (IOM) American Academy of Pediatrics Colorado Department of Public Health and Environment")
26
Vertical HIV Transmission Continues CDC estimates 280-370* infants continue to be born annually with HIV infection Missed opportunities for maternal care Mother not offered or refused HIV testing Mothers with no prenatal care (40%) * Estimates based upon report of Office of Inspector General, Department of Health and Human Services 2002
 * Estimates based upon report of Office of Inspector General, Department of Health and Human Services 2002")
27
Live Births in Colorado by HIV Test and Prenatal Care Status, 2005 CDPHE Birth Certificates/Vital Records Data 69,210 live births in Colorado 11,263 (16.6%) did not receive a prenatal HIV test 795 (1.2%) did not receive prenatal care 400 (0.3%) lacked both a prenatal HIV test and prenatal care
 did not receive a prenatal HIV test 795 (1.2%) did not receive prenatal care 400 (0.3%) lacked both a prenatal HIV test and prenatal care")
28
Prenatal HIV Testing: Birth Certificate Data 2005 testing varied from 53.4% to 99.8% Average rate 85% Low rates in some metropolitan sites in counties with higher case numbers

29
PRAMS Pregnancy Risk Assessment Monitoring Survey Randomized selected sample Maternal interviews Results (1999 data, CDPHE) –72 % of mothers reported they had been tested for HIV –7% unsure
 –72 % of mothers reported they had been tested for HIV –7% unsure")
30
Timing of HIV Testing in HIV-infected Women who Delivered a Child in Colorado by HIV Status of Child, 6/30/2006

31
Case 1 Married, employed 26 y/o primigravida in private MFM practice. Reports recent (within 1 year) HIV screen negative; test done for immigration purposes Declined HIV testing x2 Uncomplicated pregnancy, delivery; nursing infant Infant hospitalized with pneumonia at age 4 mos –Opportunistic pathogen (PCP) –Child tested for HIV and found to be infected –Parents subsequently tested, both positive
 HIV screen negative; test done for immigration purposes Declined HIV testing x2 Uncomplicated pregnancy, delivery; nursing infant Infant hospitalized with pneumonia at age 4 mos –Opportunistic pathogen (PCP) –Child tested for HIV and found to be infected –Parents subsequently tested, both positive.")
32
Case 2 25 yo G4 P3 new to state Presents in labor, no local prenatal care Routine prenatal panel and HIV test sent Vaginal delivery within hours of arrival Maternal HIV antibody screen positive on postpartum day 3; confirmed on postpartum day 5 Infant infected

33
Case 3 22 you G3 P2 presents in labor with no prenatal care Rapid HIV antibody performed, result positive Mother counseled re: possible infection –Intrapartum meds given –Infant placed on prophylaxis after delivery Maternal infection confirmed on pp day 3 Infant uninfected

34
Rapid HIV testing at delivery is needed Improved efforts to screen all expectant and breastfeeding mothers is needed –Rapid testing may positively impact prenatal testing rates once initiated

35
Issues with HIV Rapid Testing at Delivery Availability of rapid test for clinical use Obtaining counseling and consent during labor Ordering and performing the test Confidentiality and informing of positive results Treatment decisions for mother and baby must be made on initial, unconfirmed result Treatment availability (parenteral, pediatric formulations) Adequate follow up of family after discharge Cost/reimbursement issues
 Adequate follow up of family after discharge Cost/reimbursement issues")
36
Collaborative Project Combined efforts of CDPHE and CHIP Systematic outreach, training and support to delivery sites around CO: – –Train staff to perform pretest counseling/consent – –Initiate rapid HIV testing when needed 24 hour access to expert perinatal treatment consultants via pager/answering service Assist with treatment, follow up testing and referral for infected/affected families

37
An Invitation Calls welcome to discuss how our project can assist your site –Implementation of rapid HIV testing at delivery sites –Assistance to referring providers and clinics to continue/improve universal voluntary HIV prenatal screening –Kay Kinzie MSN, FNP-C Pregnancy Coordinator, CHIP 13123 E 16 th Ave Box B055 Aurora CO 80045 720-777-6006 –24 Hour Perinatal HIV Pager: 1-888-787-5947

Similar presentations



















>")