Download presentation
Presentation is loading. Please wait.

1
Advances in Thoracic Radiation Therapy Shilpen Patel MD, FACRO Department of Radiation Oncology, University of Washington, Seattle, WA

2
Objectives Understand the basics on Lung Cancer Discuss the new techniques and technologies in radiation oncology Understand current data available using these techniques

3
Roadmap Background SBRT Calypso Intensity Modulated Radiation Therapy (IMRT) Neutrons Protons
 Neutrons Protons")
4
Worldwide Incidence ACS Global Facts and Figures, 2007

5
Background: Epidemiology Estimated Incidence Jemal et al. CA Cancer J Clin. 2008 Mar-Apr;58(2):71-96
:")
6
Background: Epidemiology Estimated Deaths Jemal et al. CA Cancer J Clin. 2008 Mar-Apr;58(2):71-96
:71-96")
7
Leading Cancer Sites US Death Rate estimated

8
SBRT

9
Conventional Radiation Therapy For Medically Inoperable Tumors with 60-66 Gy: 15% long term survivors 25% death from intercurrent illness 30% death from metastatic disease 30% death from local failure only Sibley, Cancer 1998

10
Conventional Radiation Therapy What is the influence of dose? –Retrospective studies show local and distant failures decrease with increasing dose <65 Gy vs ≥ 65 Gy in Stage I patients –In a prospective dose-escalation study, doses ≥ 80 Gy resulted in improved local control and overall survival in stage I/II patients So increased dose may IMPROVE SURVIVAL Kaskowitz L et al. IJROBP 1993 Dosoretz D et al. IJROBP 1992 Sibley G et al. IJROBP 1998 Rosenzweig et al. Cancer 2005

11
An extension of existing technologies Intracranial SRS3D-CRT

12
Overview SBRT Used in primary or metastatic lesions of lung, liver, spine, retroperitoneum, pelvis Key FeaturesSRSSBRT LocationCranialExtracranial ImmobilizationRigid head frameBody Frame Max tumor diameter3-4 cm6-7 cm Dose Regimen15-24 Gy, single fraction 36-60 Gy, 3-5 fractions Targeting accuracy1 mm5 mm Respiratory ControlNoYes

13
Selecting patients for SBRT Staging of patient must be optimal –IA, IB (<=5-7cm), select IIB i.e. (T3N0 involving chest wall) –CT chest (hi-res)/abdomen with contrast –PET (sensitivity, specificity and accuracy ~90%) Confirm suspicious nodes by mediastinoscopy Caution with centrally located tumors
 –CT chest (hi-res)/abdomen with contrast –PET (sensitivity, specificity and accuracy ~90%) Confirm suspicious nodes by mediastinoscopy Caution with centrally located tumors.")
14
SBRT Results – Local Control Author# ptsDose/Fx2 yr (%) 3 yr (%)5 yr (%) Timmerman7060-66/395-- Xia4350/10-95- Onishi (multi-inst) 30018-75/1-22--80 Uematsu5050-60/5-10-94- Nagata4548/4-98- RTOG 02385954/3-98- Nyman4545/15--80
 3 yr (%)5 yr (%) Timmerman /395-- Xia4350/ Onishi (multi-inst) / Uematsu / Nagata4548/4-98- RTOG /3-98- Nyman4545/15--80")
15
IU Phase II Local Control Median follow-up = 18 months One year local control = 98% Two year local control = 95% n=5 n=60 n=32 n=70

16
RTOG 0236 Phase II Median follow-up = 34 months Three year local control = 98% Median Overall Survival = 48 months Timmerman et al JAMA 2010

17
Calypso

18
Calypso :Limitations with Current Methods Setup Errors Patient Motion Organ Motion Tumor Geometry Changes Barriers Highly Conformal Radiation Therapy Tight Margins Increased Dose Therapeutic Technologies Goals Improve Disease Control Reduce Complications Organ Motion Limits Effectiveness

19
Platform Technology — GPS for the Body ® Beacon ® Electromagnetic Transponder Wireless miniature Beacon ® Electromagnetic Transponders Accurate, objective guidance for target localization and continuous, real-time tracking Wireless miniature Beacon ® Electromagnetic Transponders Accurate, objective guidance for target localization and continuous, real-time tracking Actual size: ~8.5 mm

20
Platform Overview Implanted Beacon ® Electromagnetic Transponders 4D Tracking Station™ 4D Console™ Infrared Cameras Optical Targets Optical System 4D Electromagnetic Array™

21
System Overview – Monitoring 0.00 0.05 0.10 0.150.200.25 0.050.000.15 Tumor bed motion monitoring Post-treatment reports Tumor bed motion monitoring Post-treatment reports

22
What about IMRT?

23
Lung IMRT (primary) Wedge-Pair Conventional 6MV 9-Field
 Wedge-Pair Conventional 6MV 9-Field")
24
Reasons to wait Tumor motion Dose calculations –Small field heterogeneity NTCP –Large volume low dose But sometimes you can’t –Consider radioprotectors

25
Neutrons

26
Relative Biologic Effectiveness

27
Salivary Gland Protocol 80-01

28
Salivary Gland: Local Control

29
Example of Tumors Treated

30
Adenoid Cystic Ca Trachea

31
Protons

32
Protons behave differently than x-rays: –Protons –X-Rays do not Protons improve the “therapeutic ratio” –maximizing tumor control while minimizing side effects At a given radiation dose to a tumor protons deliver, on average, less than half the radiation dose to normal tissues than do x-rays 1 The Value of Protons

34
Evidence of Distal Range Stopping Before treatmentTreatment planAfter treatment

35
35 3D 5 fields 6x Parallel opposed fields tumor Improvements in radiation dose distribution Protons 4 field IMRT 9 fields E VOLUTION ? x-rays protons

36
Why Protons for Lung Cancer? Paradigms for lung cancer and radiation therapy –More dose leads to improved outcomes? –Retrospective analysis shows that >70 Gy is desirable –Larger volumes to low and intermediate doses are associated with high rates of esophagitis and pneumonitis 36

37
Why Protons for Lung Cancer? X-rays have reached its dose limits Trials showing that the maximum tolerated dose is 74 Gy with chemotherapy Protons allow dose escalation while reducing toxicity compared to x-rays Dose escalation can be achieved with protons without exceeding known indicators of lung toxicity 37

38
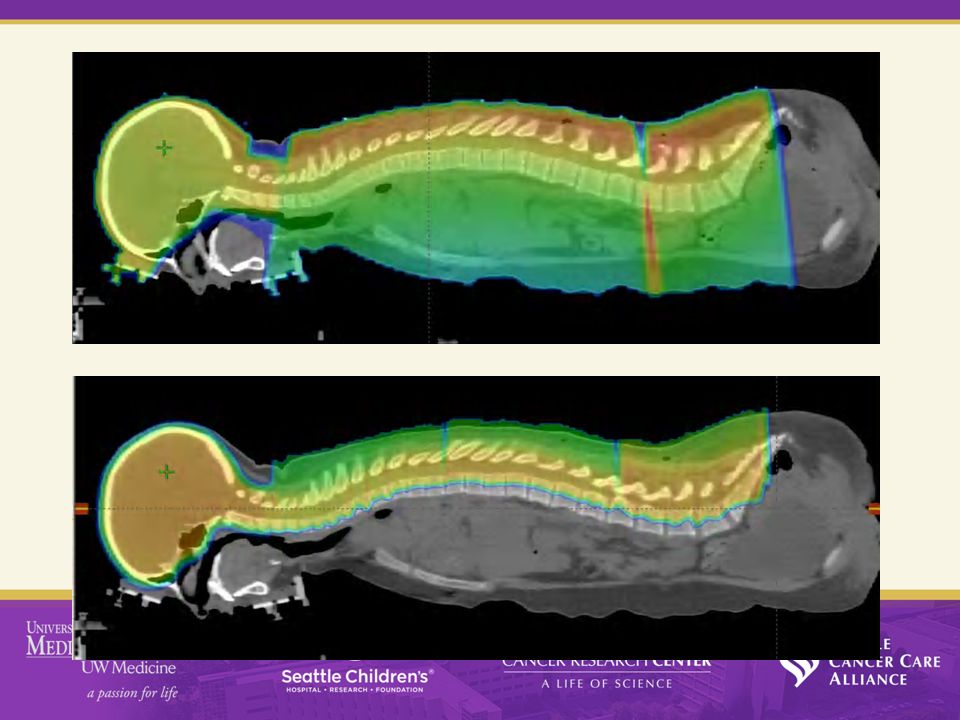
Lung/Mediastinum – IIIA NSCLC ProtonsIMRT IMRT- Protons 38

39
Lung with tumor (dose to healthy tissue only) Lung without tumor Both lungs Volume receiving doseVolume receivingIntegral dose Mean Dose5 Gy10 Gy20 Gy5 Gy IMRT24.2 Gy61.5%49.0%37.1%49.7%8.1 Gy Proton21.2 Gy44.0%39.3%33.3%27.1%5.4 Gy Absolute improvement3.0 Gy17%10%4%23%33% Radiation-induced pneumonitis can result from even low doses of excess radiation in the lungs Excess Radiation Causes Long-Term Side Effects Comparison of Dose Escalated Proton Therapy and IMRT, both 74 Gy, for Stage III Lung Cancer 39
 Lung without tumor Both lungs Volume receiving doseVolume receivingIntegral dose Mean Dose5 Gy10 Gy20 Gy5 Gy IMRT24.2 Gy61.5%49.0%37.1%49.7%8.1 Gy Proton21.2 Gy44.0%39.3%33.3%27.1%5.4 Gy Absolute improvement3.0 Gy17%10%4%23%33% Radiation-induced pneumonitis can result from even low doses of excess radiation in the lungs Excess Radiation Causes Long-Term Side Effects Comparison of Dose Escalated Proton Therapy and IMRT, both 74 Gy, for Stage III Lung Cancer 39")
40
Lung with tumor (dose to healthy tissue only) Lung without tumor Both lungs Volume receiving doseVolume receivingIntegral DoseMean Dose5 Gy10 Gy20 Gy5 Gydose Conventional Dose IMRT60-63 Gy20.1 Gy58.5%45.3%34.5%45.5%6.8 Gy Escalated Dose Proton74 Gy21.1 Gy44.0%39.3%33.3%27.1%5.4 Gy Absolute improvement-(1.0) Gy14.5%6.0%1.2%18.4%21% Excess Radiation Causes Long-Term Side Effects Comparison of Dose Escalated Proton Therapy (74 Gy) and Conventional Dose IMRT (60-63 Gy) for Stage III Lung Cancer 40
 Lung without tumor Both lungs Volume receiving doseVolume receivingIntegral DoseMean Dose5 Gy10 Gy20 Gy5 Gydose Conventional Dose IMRT60-63 Gy20.1 Gy58.5%45.3%34.5%45.5%6.8 Gy Escalated Dose Proton74 Gy21.1 Gy44.0%39.3%33.3%27.1%5.4 Gy Absolute improvement-(1.0) Gy14.5%6.0%1.2%18.4%21% Excess Radiation Causes Long-Term Side Effects Comparison of Dose Escalated Proton Therapy (74 Gy) and Conventional Dose IMRT (60-63 Gy) for Stage III Lung Cancer 40")
41
Lung toxicity for inoperable NSCLC 3D CRTIMRTProtons Dose63 Gy 74 CGE % patients stage IIIA-B2 2 87%91%87% Toxicity Esophagitis – G3+18%44%5% Pneumonitis – G3+30%9%2% NSCLC treated with radiation therapy + chemotherapy 1 41

42
Protons outcomes and toxicity for radiation + chemo RTOG 0117M.D. Anderson Trial typePhase II Type of radiation3D CRTProtons Dose74 Gy74 CGE Median follow up (months)19.3 4 19.7 Survival Median months21.6 4 29.4 1-year overall rate72.7% 4 86% 1-year progression free rate50.0% 4 63% Toxicity Esophagitis – G3+40% (G2+) 5 11% 6 Pneumonitis – G3+23%2% Comparison of Phase II results from RTOG 0117 and M.D. Anderson– radiation and chemotherapy
 Survival Median months year overall rate72.7% 4 86% 1-year progression free rate50.0% 4 63% Toxicity Esophagitis – G3+40% (G2+) 5 11% 6 Pneumonitis – G3+23%2% Comparison of Phase II results from RTOG 0117 and M.D. Anderson– radiation and chemotherapy.")
43
Selection criteria RTOG 0117 1 M.D. Anderson Operable/inoperableInoperable StageI-IIIBIII Zubrod performance0 to 1NA Karnosky performanceNA70-100 Weight loss within past 6 months ≤ 5% ≤ 10% Other Expiratory volume at 1 second ≥ 1L Atelectasis < 1 lung Key dosimetry constraints 2 Volume lung V20 ≤30% Mean esophageal dose ≤ 34 Gy Volume lung V55 ≤ 30% Volume normal lung V20 ≤ 35% Mean lung dose ≤ 20 Gy Esophagus volume V50 ≤ 50% Exclusion criteria Prior radiation to thorax Prior chemo or biologics for lung cancer within past 2 years Prior concurrent malignancy unless disease free for ≥1 year

44
Protons+SBRT?

45
Proton SBRT for Stage I NSCLC Better than photon therapy? Are photons limited? –Centrally located –Previously irradiated –Close to the Chest Wall –Large Tumors? 45

46
Proton SBRT for Stage I NSCLC Dose:42-50 Gy in 3 to 5 fractions Toxicity: Median Follow-up of 24 months –2 year Overall Survival 64% and LC 100% 46 Radiation Associated Toxicity (n = 20) Graded ToxicityGrade 1Grade 2Grade 3 Chest wall pain010 Dermatitis310 Dyspnea000 Fatigue110 Pneumonitis601
 Graded ToxicityGrade 1Grade 2Grade 3 Chest wall pain010 Dermatitis310 Dyspnea000 Fatigue110 Pneumonitis601")
47
Take Home Points Technology will help our patients Efficacy and side effects will improve Careful attention to detail will be required to optimally implement new technologies Proton therapy is promising and should be considered in select patients

Similar presentations


 is effective, but can be associated with debilitating side.>")








: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")







