Download presentation
Presentation is loading. Please wait.

1
OPERATIONAL BARRIERS TO FAMILY PLANNING IN CONFLICT-AFFECTED COUNTRIES EXPERIENCES FROM SIERRA LEONE Freetown, Sierra Leone (c) 2000 Dianne Stare, Courtesy of Photoshare.
 2000 Dianne Stare, Courtesy of Photoshare.")
2
Presentation Overview Review research performed by Constella Futures under the USAID Health Policy Initiative Task Order 1 Project in Sierra Leone. Contextual Information –USAID Health Policy Initiative Project Task Order 1 –Sierra Leone –Operational Barriers Objectives of the Study Methodology Key Findings Recommendations for –Stakeholders in Sierra Leone –International Community

3
Contextual Information Health Policy Initiative Task Order 1 Sierra Leone Operational Barriers AIDS Orphan and Grandma Suzan Copyright 2004 WHO “River of Life” By Dieter Telemans

4
USAID Health Policy Initiative Task Order 1 Global 5 year project focusing on policy development and implementation –Reproductive Health –HIV/AIDS Partnership with: –White Ribbon Alliance –World Conference of Religions for Peace –Center for Development and Population Activities

5
Contextual Information: Sierra Leone Refugee and IDP Situation Ceasefire in 2001 More than half of the population displaced From 2001-2005 an estimated 230,000 refugee’s returned to Sierra Leone (UNHCR, 2007) Renewed conflict in Liberia from 1999-2003 Eight refugees camps in Sierra Leone with Liberian refugees –Approximately 60,000 Liberian refugees in 2005
 Renewed conflict in Liberia from Eight refugees camps in Sierra Leone with Liberian refugees –Approximately 60,000 Liberian refugees in 2005")
6
Contextual Information: Sierra Leone Policy Environment Contraceptive Security Strategy National Reproductive Health Policy

7
Contextual Information: Operational Barriers Definition Rules, regulations, codes, guidelines, plans, budgets, procedures, and administrative norms that governments use to translate national laws and policies into programs and services. Cross et al, 2001

8
Operational Barriers

9
hjk Study Objectives “10 Facts About Women’s Health” Copyright 2007 WHO Slide 2

10
Study Objectives Explore refugee/IDP family planning needs before, during, and after conflict Determine the root causes of the barriers to quality, accessible services Build capacity of local groups to analyze operational barriers to services Devise policy actions and recommendations for overcoming barriers—that are applicable both in-country and in other conflict-affected countries

11
Methodology “10 Facts About Women’s Health” Copyright WHO 2007, Slide 6 “Malaria in Pregnancy” Copyright WHO 2007, Slide 1

12
Study Methodology Tools Used: Focus Group Discussions –14 groups Journey of a Woman –4 groups Key Informant Interviews –20 interviews Policy Environment Score –7 respondents

13
Key Findings Focus Group Discussions Journey of a Woman Key Informant Interviews Policy Environment Score “Malaria In Pregnancy” Copyright 2007 WHO, Slide 8

14
Key Findings: Focus Group Discussions Before the Conflict Knowledge, access, and use of family planning were very limited in Sierra Leone and Liberia before the recent conflicts. Quotes “It was difficult because the clinic was seven miles away. You would have to walk. Then the clinic would not have commodities.” – Refugee woman “Availability depends on where you were. In some cases, family planning was only given if you were married or if you had 5–6 children.” – Refugee woman “People could not pay for services.” – IDP man

15
Key Findings: Focus Group Discussions During the Conflict While still limited, refugees—through camps— experienced a greater increase in access to family planning than IDPs. Both populations were concerned mainly about basic survival, though some expressed growing interest in family planning. Quotes “I was off [of family planning] for five months during the war.” – Refugee woman Given the challenges associated with forced migration, some women expressed a growing interest in family planning during the conflict. “Women were looking at suitcases and kids they had to move.” – IDP woman

16
Key Findings: Focus Group Discussions After the Conflict While most women were not using family planning before the conflict, a majority reported demand after the conflict. “I hope I will be near a clinic [when I return to Liberia] so I can continue family planning use.” – Refugee woman “If we have too many children, we can’t take care of all of their needs and some may become rebels.” – IDP man

17
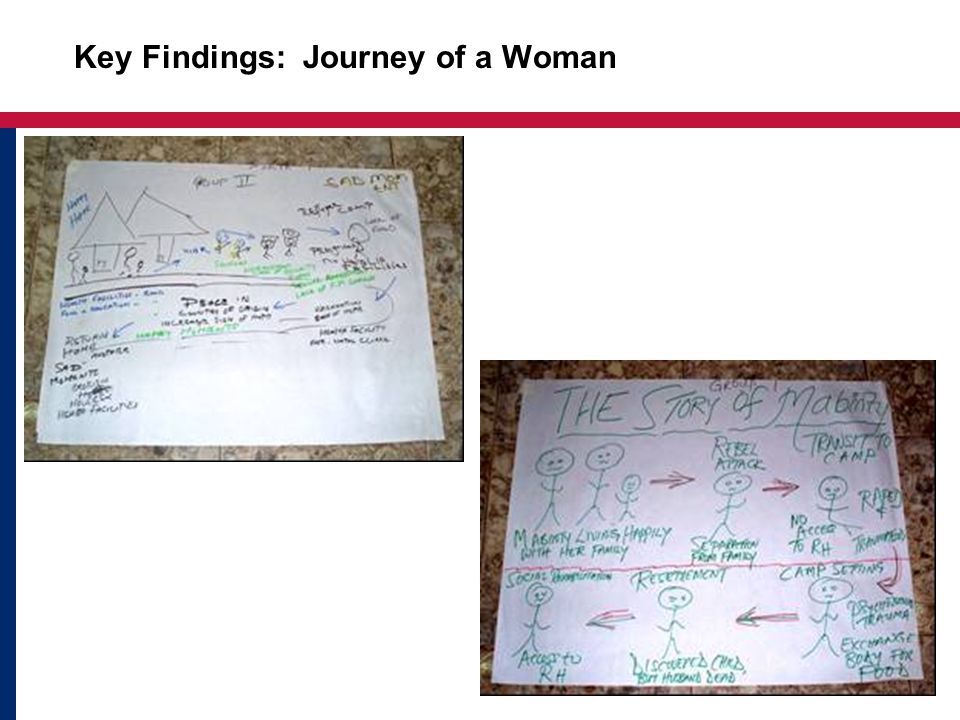
Key Findings: Journey of a Woman

19
Key Findings: Key Informants Organizations Lack Consistent Service Guidelines and Protocols Costs are Transferred to Clients Provider Bias Can Restrict Clients to Specific Methods Stock-outs of Commodities are Common Youth-friendly Services are Limited Improved Services to Address Sexual Violence are Needed

20
Key Findings: Key Informants, cont. Human resource shortages and lack of training (e.g., nurses are recruited to other countries) Limited knowledge and misconceptions about family planning among clients Lack of community-driven services Camp clinic services depend on the funding source and implementing agency; if the donor or the organization operating the clinic changes, the services offered might also change
 Limited knowledge and misconceptions about family planning among clients Lack of community-driven services Camp clinic services depend on the funding source and implementing agency; if the donor or the organization operating the clinic changes, the services offered might also change.")
21
Key Findings: Policy Environment Score

22
Recommendations Stakeholders in Sierra Leone International Community Kenya: A Family’s Health is Renewed” Copyright 2007 WHO/Evelyn Hockstein

23
Recommendations for Stakeholders in Sierra Leone A clear and comprehensive strategy to implement the newly approved National Reproductive Health Policy should be created using a participatory process similar to the one that was used to create the policy. The contraceptive security strategy developed in collaboration with the DELIVER and AWARE project should be used to reform and reinforce the logistical system to improve availability of contraceptives at all access points.

24
Recommendations for Stakeholders in Sierra Leone, cont. Given the lower levels of family planning knowledge and access, areas of the country that did not have refugee camps should be geographical priority areas for the rolling out of the new reproductive health policy. A plan to provide in-service training for all health facility personnel on reproductive health, including family planning and sexual violence, should be developed and implemented. Marie Stopes International is currently implementing a successful model of community-based distribution. This approach should be replicated and scaled up to cover a larger geographical area. Rebuilding of health facilities, with focus on upgrading and supplying equipment and improved sanitation, should be a priority.

25
Recommendations for the International Community Advocate for the inclusion of family planning in repatriation plans with a focus on providing adequate supplies of commodities for women to be used during the transition back to their country of origin. Family planning should be included in the initial package of services provided to refugees during the camp registration process.

26
Recommendations for the International Community, cont. A system for examining and strengthening the reproductive health knowledge of camp providers needs to be developed and implemented early in the intervention. A collaborative approach to importing commodities during the conflict could benefit all international organizations working in-country by allowing them to piggyback on effective logistic systems.

27
Thank You Freetown, Sierra Leone(c) 2002 Antje Becker- Benton/CCP, Courtesy of Photoshare Sierra Leone(c) 2004 D. Sombie/CARE Sierra Leone, Courtesy of Photoshare

Similar presentations










 Dr. Kwesi Aning, ‘Peacekeeping for the Long Term: Strengthening Effectiveness and Accountability’>")






 of DepoProvera (DMPA) in Kenya Alice Olawo 1, Jane Gitonga 2, Elizabeth Washika 3.>")

