Download presentation
Presentation is loading. Please wait.

1
Evaluation of Cardiac Injury and Function

2
Introduction CHD, – The most important disease affecting the heart is coronary heart disease ACS, – CHD, can lead to an acute blockage of coronary blood flow known as an acute coronary syndrome MI, – ACS with frank necrosis of any amount of myocardium is known as myocardial infarction

3
Background Ischemia – the lack of an adequate blood supply Atherosclerosis – a chronic process involving damage to endothelium and the build-up of vessel occluding lesions called plaque. angina pectoris (exertional angina) – Once the diameter of a coronary artery is reduced to less than 10-20% of its original size
 – Once the diameter of a coronary artery is reduced to less than 10-20% of its original size.")
4
Background Myocardial infarction (MI) – Complete blockage of blood flow Irreversible ischemic damage Unstable angina (UA) – When the blockage is not complete – irreversible muscle damage may be avoided – experience severe angina, even at rest
 – Complete blockage of blood flow Irreversible ischemic damage Unstable angina (UA) – When the blockage is not complete – irreversible muscle damage may be avoided – experience severe angina, even at rest")
5
Diagnosis of Cardiac diseases (Outline) Cardiac diseases discussed in this session – Coronary heart disease (CHD) – Heart failure (HF) Diagnosis of Cardiac diseases – Clinical (non laboratory) examination e.g, Clinical history, ECG, angiography, echocardiography – Biochemical markers Markers of Myocardial Damage Risk factors associated with the development and progression of CHD. ECG;ElectroCardioGraphy

6
Heart Disease Statistics for the US

7
Markers of Myocardial Damage Cardiac enzymes – Transaminases (SGOT,SGPT) – Lactate dehydrogenase (LD) – Creatine kinase (CK) Improved cardiac specificity – with separation of isoenzymes. LD 1 is relatively abundant in cardiac muscle – Flipped LD, where the normal finding LD 2 > LD 1 ] is reversed.

8
In normal heart, 15-20% of the CK is CK-MB Changes in LD observable for a much longer time than changes in CK. The isoenzyme analyses were relatively lengthy & tedious – Could only be performed about once per day CK-MB Mass Assay – Can be performed rapidly

9
Kinetics of several cardiac markers following an MI

10
Cardiac Troponin The most important laboratory test for cardiac diagnosis. TnT (tropomyosin-binding subunit, 37 kDa) Tnl (inhibitory subunit, 24 kDa), TnC (calcium-binding subunit, 18 kDa).
 Tnl (inhibitory subunit, 24 kDa), TnC (calcium-binding subunit, 18 kDa)..")
11
Cardiac Troponin Tnl has a cardiospecific form (cTnl) TnT also has distinct forms in myocardium (cTnT) – Also, Fetal skeletal muscle and diseased skeletal muscle. post-translational modifications cause detectable differences

12
Cardiac Troponin Bound form – released slowly over the course of 1-2 weeks following myocardial infarction. Free form – time frame similar to that of CK-MB, with cTn reaching a peak at about 24 h following MI cTnT and cTnl are nearly absent from normal serum Small elevations – pericarditis, myocarditis, pulmonary embolism, renal failure, sepsis, and other critical illness

13
The high sensitivity and specificity of cTn Patients with ischemic symptoms who also have elevations in cTn receive greater benefit from therapies with various antiplatelet and anti thrombotic agents

14
Myoglobin Lacking cardiac specificity, more rapidly than other proteins Within 2-3 h following onset of MI, earlier than with troponin or other markers myoglobin peaks about 6 h after MI and returns to baseline after 24 half-life,approximately 4 hours, but is longer if renal function is impaired.

15
Myoglobin Muscle mass and muscle activity – Higher in men increases with increasing age Day-to-day variation is about 10-15% offers fairly high clinical specificity (> 95%) when patients with renal failure or suspected injury to skeletal muscle are excluded. Sensitivity can be enhanced – δ Mb

16
Other Markers Carbonic Anhydrase III(CA III) – present in skeletal but not cardiac muscle, Negative cardiac marker. Creatine Kinase Isoforms – a high ratio of MB 2 /MB 1 suggests that a recent release of enzyme has occurred. – in the first 3-4 hours following symptom onset, improved sensitivity for MI detection

17
Limitations cTn – is a highly heterogeneous analyte. – Reference ranges and decision points have been a matter of some confusion

18
Diagnosis of ACS Biochemical markers play a secondary role in the initial management of patients with suspected ACS. The earliest decision-making, which should ideally take place within 10 min of the patient's arrival in the ED, is based on history, physical examination, and 12-lead ECG Likely to be negative at this early time. ACS: acute coronary syndrome. ED: emergency department

19
Choice of markers and time points – cTn (either I or T) is the preferred marker for definitive diagnosis Also for early diagnosis, – Myoglobin but possibly CK isoforms, at the 0 and 1- to 4-h time points.
 is the preferred marker for definitive diagnosis Also for early diagnosis, – Myoglobin but possibly CK isoforms, at the 0 and 1- to 4-h time points.")
20
noninvasive indicator that reperfusion has occurred, – Myoglobin was found to perform better than CK- MB or cTn early reinfarction – CK-MB appears to be superior to cTn because of its more rapid decline following MI – myoglobin is also useful.

21
Diagnosis of MI following surgical procedures – cTn is clearly the marker of choice in this situation,

22
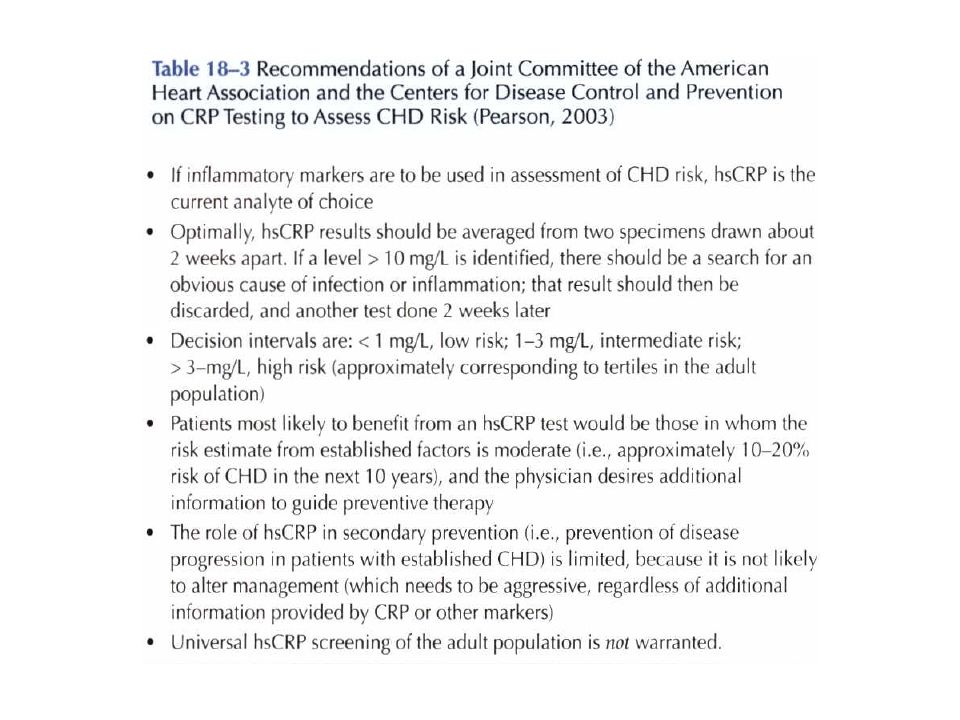
Markers of Coronary Risk Laboratory tests – Serum cholesterol LDL HDL, a negative risk factor Triglyceride C-Reactive Protein (CRP) – In acute illness, cytokines, chiefly interleukin-6, stimulate hepatic production of CRP
 – In acute illness, cytokines, chiefly interleukin-6, stimulate hepatic production of CRP")
23
Clinical (non laboratory) risk factors for CHD
 risk factors for CHD")
24
Markers of Coronary Risk the usefulness of the hsCRP test in individual patients has been controversial. – the variations in quantitative risk estimates, – the unclear role of CRP in pathogenesis of vascular disease, – the lack of specific treatment for high CRP,

26
Markers of Coronary Risk epidemiology studies – confirm a correlation between moderate Hey levels and CHD. Homocysteine (Hey) – total homocysteine (tHcy): free sulfhydryl group, as a disulfide (homocystine), as a mixed disulfide, – linked to a plasma protein via one of its cysteine residues. Excessive levels of circulating Hcy – Enzyme defect Cystathionine-β-synthase
 – total homocysteine (tHcy): free sulfhydryl group, as a disulfide (homocystine), as a mixed disulfide, – linked to a plasma protein via one of its cysteine residues. Excessive levels of circulating Hcy – Enzyme defect Cystathionine-β-synthase.")
27
Chemical structure of homocysteine and related compounds.

28
Markers of Coronary Risk Clinical manifestations – thromboembolic disease, including CHD The basis of the damaging effects of Hcy is uncertain. – Oxidant stress and inhibition of transmethylation reactions are likely Measurment – Chromatographic – Enzymatic

29
Clinical algorithm for treating patients presenting to an emergency department with symptoms suggesting ACS.

30
Markers of Congestive Heart Failure Cardiac Natriuretic Peptides – brain natriuretic peptide (BNP) produced mainly in the cardiac ventricle – Secretion enhanced by ventricular wall stretch and volume overload, as occurs in HF – Circulating half-life is approximately 22 minutes. – (N-terminal fragment)N-BNP is considerably longer (60-120 min)
N-BNP is considerably longer ( min).")
31
Markers of Congestive Heart Failure Applications of BNP testing – The best-established application For diagnosing acutely ill patients presenting to emergency service with shortness of breath. At a decision point of 100 pg/mL, the BNP test had the following characteristics for diagnosis of HF: – Sensitivity 90%, – Specificity 76%, – Positive predictive value 79%, – Negative predictive value 89%

32
Markers of Congestive Heart Failure Other applications of BNP testing – Monitoring the course and treatment of patients with HF – Risk stratification of patients with ACS – Monitoring disease severity in patients with stable CHD – Screening for ventricular dysfunction – Testing for drug cardiotoxicity

33
Markers of Congestive Heart Failure The major limitation of BNP – Decision point a wide range of values is observed in patients with and without HF – Patients with symptomatic HF especially when it is chronic and stable, can have 'normal' levels So, – the most appropriate use of the BNP test is as an adjunctive test to rule out HF in the acute setting.

34
Markers of Congestive Heart Failure BNP has natriuretic, vasodilatory, and other effects that are ameliorative for the syndrome, and is in fact available as the drug nesiritide (Natrecor) for treatment of HF
 for treatment of HF")
Similar presentations


 J. Teixeira, (2) P. Wotquenne, (2) V. D’Orio, (3) D. Gruson, (1)>")


 are enzymes that differ in amino acid sequence but catalyze the same.>")







>")





 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")