Download presentation
Presentation is loading. Please wait.

1
SOLID PHASE IMMUNOASSAYS: INTERPRETING PATTERNS Julie Houp, CHS Johns Hopkins University School of Medicine Division of Immunogenetics and Transplantation Immunology Baltimore, MD

2
INTRODUCTION SPIAs are a critical part of identification of HLA antibodies relevant to transplantation, specifically, donor-specific antibody (DSA). In the pre-transplant or evaluation setting, the availibilty of donor lymphocytes allow for crossmatch testing to be performed and SPIA results to be correlated with the crossmatch (FCXM or CDC). In the assignment of unacceptable antigens, SPIAs are utilized to virtually assess compatibility based on HLA specificity. In the post-transplant setting, therapeutic drugs (Rituximab, Thymoglobulin) and the need for live donor cells make it more difficult or impossible to perform a crossmatch. We must rely more heavily on SPIAs and attempt to predict the strength of DSA as it correlates to a crossmatch test.
. In the assignment of unacceptable antigens, SPIAs are utilized to virtually assess compatibility based on HLA specificity. In the post-transplant setting, therapeutic drugs (Rituximab, Thymoglobulin) and the need for live donor cells make it more difficult or impossible to perform a crossmatch. We must rely more heavily on SPIAs and attempt to predict the strength of DSA as it correlates to a crossmatch test..")
3
ANALYSIS D.4.1.4 Computer Programs D.4.1.4.1 All computer software programs and version upgrades used for analyses must be validated for accuracy and this validation documented, prior to release of test results. D.4.1.4.2 The laboratory must have an ongoing process (at least annually) to ensure that all computer- assisted analyses are accurate. D.4.1.4.3 The laboratory must document historic test result review when notified by a vendor of an update/revision/correction to analysis software or template that could yield a change, correction, or update to the original test result and take appropriate corrective action.
 to ensure that all computer- assisted analyses are accurate. D The laboratory must document historic test result review when notified by a vendor of an update/revision/correction to analysis software or template that could yield a change, correction, or update to the original test result and take appropriate corrective action..")
4
COMPUTERIZED ANALYSIS Inclusion analysis. The basic algorithm used by analysis. Software. Statistical analysis includes chi square, correlation coefficient (r-value), and percent inclusion. Certain pitfalls may exist in relying solely on computerized analysis!
, and percent inclusion. Certain pitfalls may exist in relying solely on computerized analysis!.")
5
TACTICS TO IMPROVE ACCURACY OF ANALYSIS Consideration of the patient’s own phenotype in analysis Identification of sensitization (previous mismatches from previous transplants or pregnancy) Analysis of sera at multiple dilutions Utilization of several screening methods (certain methods allow the ability to see the strength of the reactions, etc.) Utilization of available crossmatch results in analysis Consideration of patient information (therapeutic drugs, underlying diseases) Evaluation of sera over several different lots
 Analysis of sera at multiple dilutions Utilization of several screening methods (certain methods allow the ability to see the strength of the reactions, etc.) Utilization of available crossmatch results in analysis Consideration of patient information (therapeutic drugs, underlying diseases) Evaluation of sera over several different lots")
8
SINGLE ANTIGEN BEAD AT 1:64 DILUTION

9
DP1, DP4 DP6, DP17

10
NO DSA PRIOR TO TRANSPLANT REACTIVITY WITH DQ ENHANCED BEADS REFLECTS INCREASE IN DP ANTIBODY

11
Patient is a B35. Self reactivity?

12
Patient is B*35:03, previous transplant is B*35:01 B*35:01 and B*35:03 differ at pos 116

13
B*35:01 B*35:05 B*35:08

14
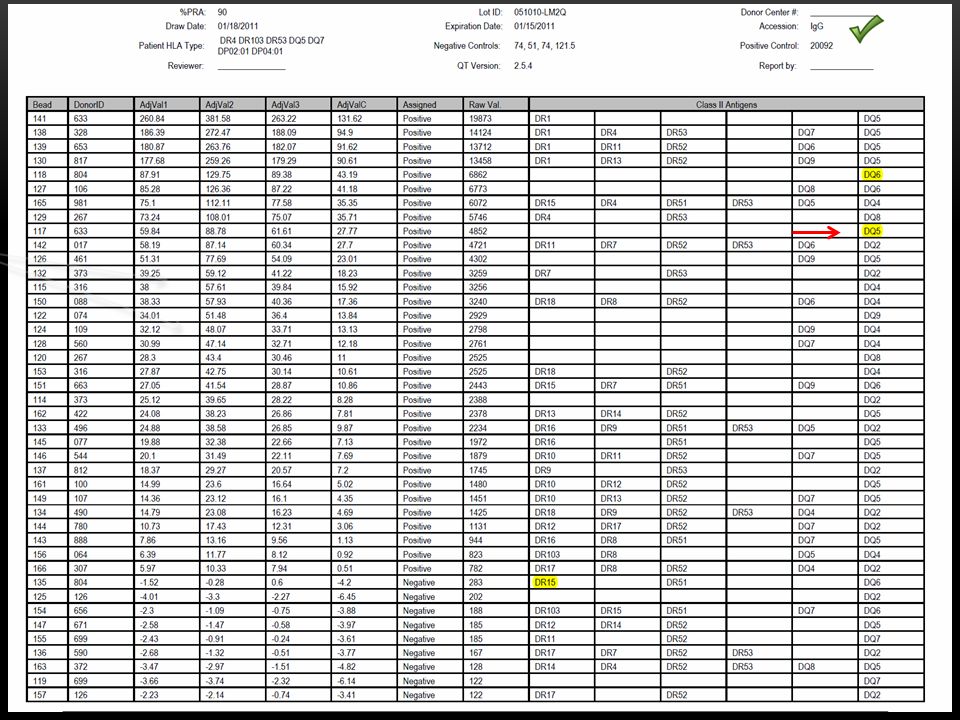
39 y.o. male CAPS syndrome 1 st TX: LURD in 2005 No HLA specific antibody detected prior to Tx 2 nd TX: LURD Repeat mismatch DR53

15
ANTIBODY TESTS PRIOR TO TX # 2 Negative? Maybe DQA5/DQB2 (a previous MM)
")
16
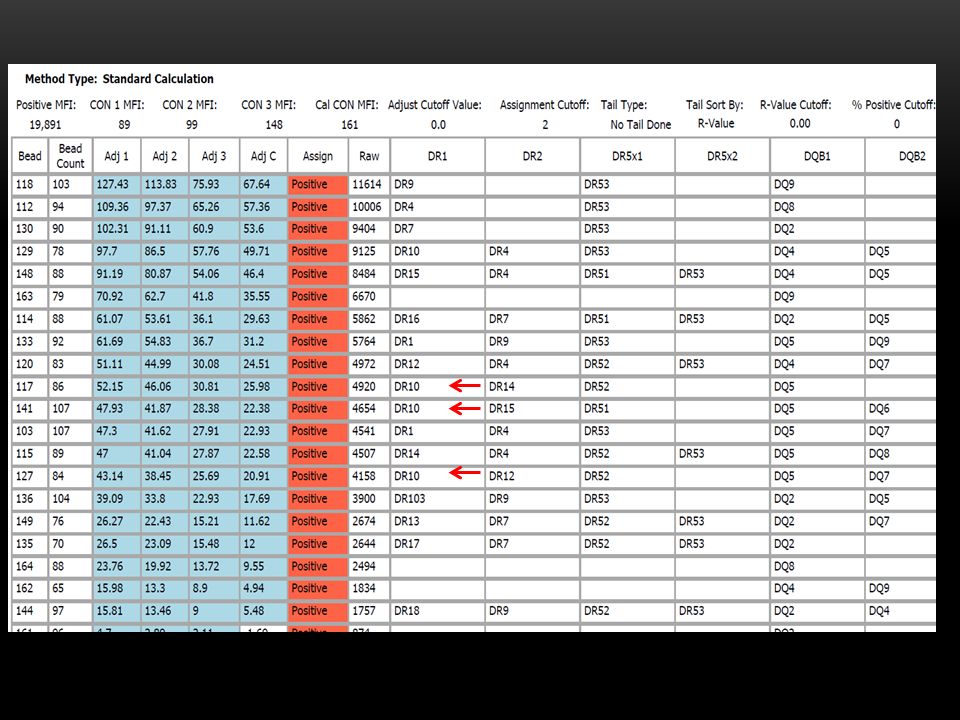
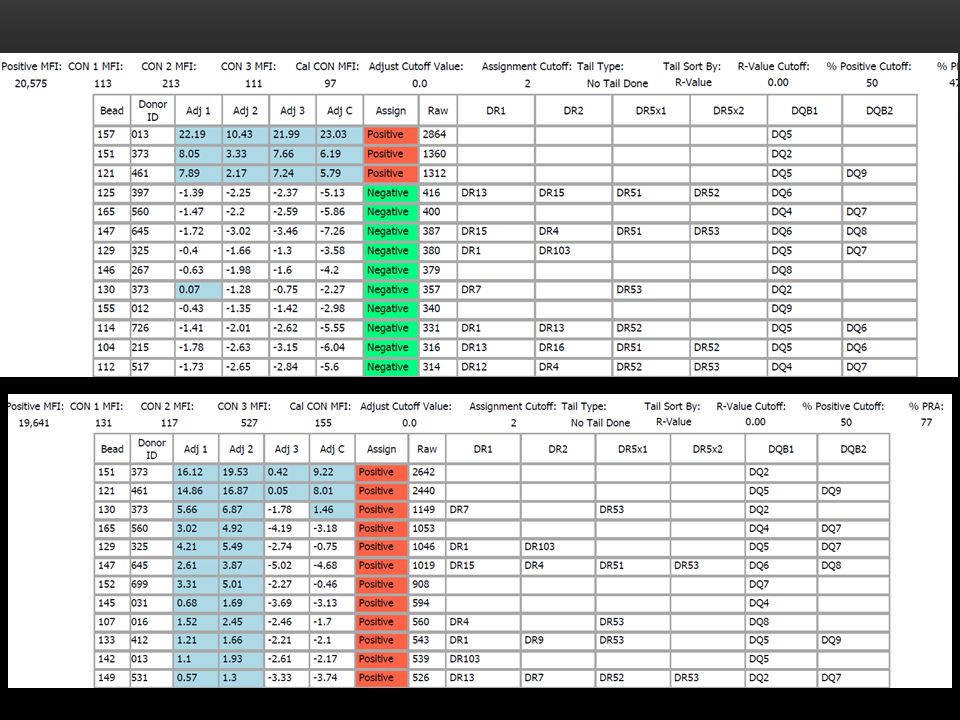
SA assay #1: DQ2 SA assay #2: DR53 DR10

17
TRANSPLANT OR NOT? FCXM was negative 2 pre-tx TPE and 7 post-tx TPE 18 months post-transplant with no rejection Eculizimab

19
SINGLE ANTIGEN BEAD RESULTS Reactivity with DR53 beads >20000MFI Reactivity with DR10 moderate 12000MFI Additional specificity DQA3 6000MFI Dilution at 1:8: DR53 >10000MFI DR10 4000MFI VIRTUAL PREDICTION: CDC POSITIVE WITH DR53; FCXM POSITIVE WITH DR10

20
CROSSMATCH RESULTS CDC One wash B cell crossmatch positive with the patient’s spouse. DR10, DR17 CDC One wash B cell crossmatch weaker positive with DR7, DR14 FCXM results confirm these findings

23
Patient had two potential donors Donor #1: B7 Donor #2: A2 Donor #2 selected to donate 5 days later…

26
Patient is DR17 DQA5 DQB2 Single antigens bead assay confirms DQA2 and DQB5 reactivity

27
Patient is a DR7 DQA2 DQB2 Single antigen bead assay does not confirm reactivity

29
Donor is child: DSA DR11, DQ7 Single Antigen Bead assay correlates strength of DSA FCXM was weakly positive, auto XM also positive

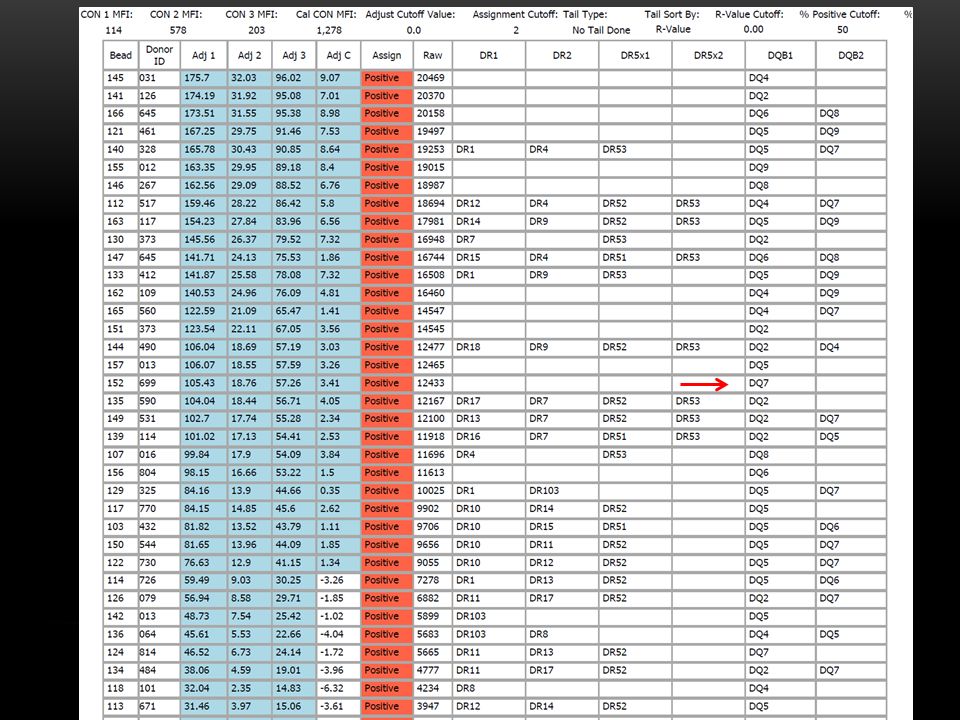
31
Single antigen bead assay confirms DQ7 reactivity >20000MFI 1:8 dilution DQ7 16000MFI

32
CONCLUSIONS Highly sensitized patient often have issues that challenge the limitations of SPIAs Patient information (sensitization, medications) can greatly assist the analysis HLA typing at the allele level may be needed Extensive expertise with the vagaries of SPIAs is needed to correctly interpret results and provide consistent results to clinicians
 can greatly assist the analysis HLA typing at the allele level may be needed Extensive expertise with the vagaries of SPIAs is needed to correctly interpret results and provide consistent results to clinicians")
33
Johns Hopkins Immunogenetics Laboratory Dr. Andrea A. Zachary, Dr. Mary S. Leffell, Dr. Annette Jackson and Renato Vega ACKNOWLEDEMENTS

35
Julie A. Houp, CHS Laboratory Manager Division of Immunogenetics and Transplantation Immunology Johns Hopkins School of Medicine Office 410.955.3600 x130 Mobile 410.926.7643 juliehoup@jhmi.edu CONTACT INFORMATION

Similar presentations









 Anti-A11 and B44.>")


 were tested using three serology tests. All testing was performed at the university.>")





>")





