Download presentation
Presentation is loading. Please wait.

1
GRAND ROUNDS Desirée Ong, M.D. PGY-2 Vanderbilt Eye Institute

2
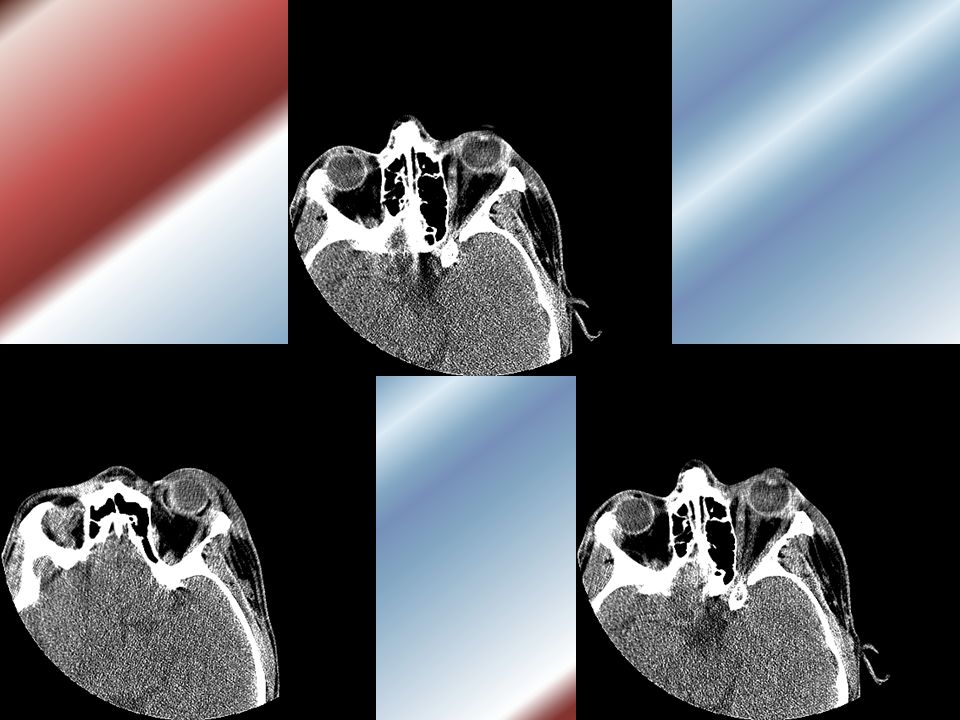
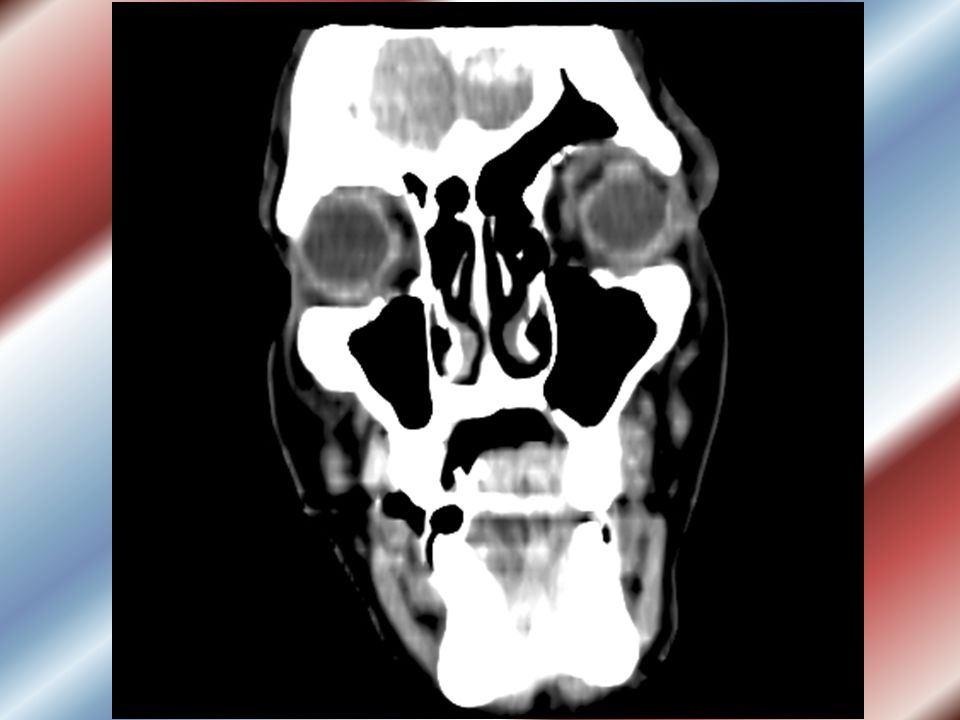
Patient CP 23 yo WM, passenger in MVA, was found unconscious next to vehicle. Driver was not at the scene In the ED, pt was noted to have swelling and ecchymosis of the left peri-ocular area ED staff noted a unilateral irregular pupil and were concerned about the possibility of an open globe

5
Exam findings Gen: unconscious, unable to be awakened No friends or family were present No witnesses were at the scene VA/VF: unable to obtain Pupils: OD 3mm-->2mm, OS irregular pupil with no constriction IOP: OD 17 OS 24,25,27

6
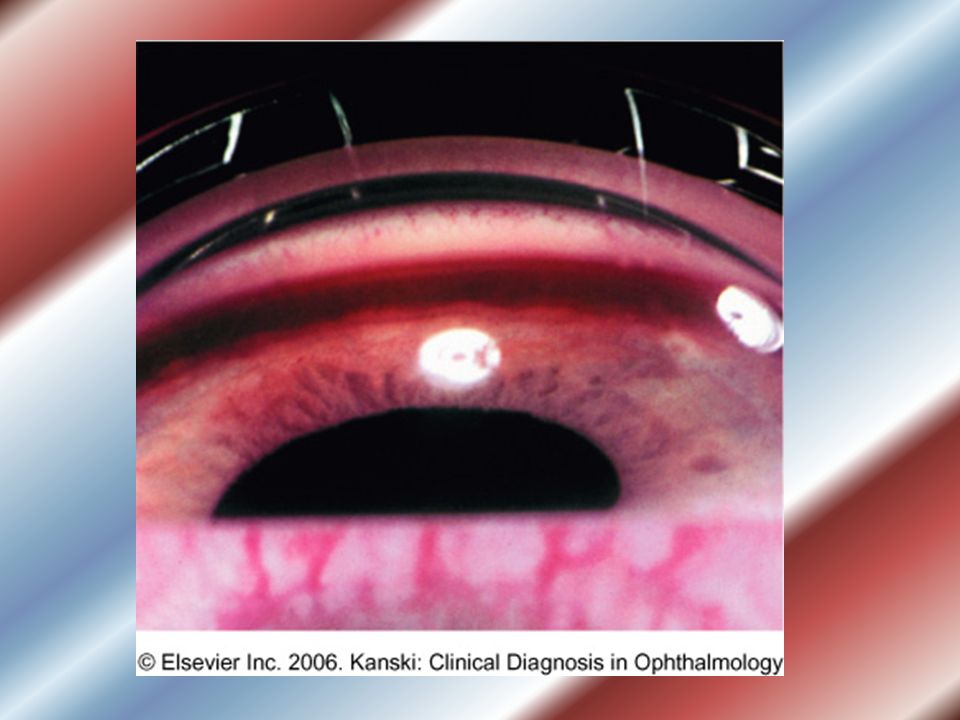
Differential Diagnosis for Corectopia?

7
Differential Diagnosis Trauma: high suspicion for open globe, FOB, corneal perforation, iridodialysis Iatrogenic: anterior segment surgery ICE syndrome Posterior synechiae/inflammatory changes Iris tumor Iris coloboma Iris stromal hypoplasia Ectropion uveae Posterior polymorphous dystrophy Posterior embryotoxin/Axenfeld-Rieger Syndrome Peter’s Anomaly Ectopia lentis et Pupillae

10
Family arrives to bedside.. Pt has a h/o Sturge-Weber syndrome with glaucoma; pt is s/p tube shunt placement at the age of 6, his left pupil has looked like that since the surgery. Pt has had laser treatments of his port wine stain. POH: as above FH: no eye disease or SWS PMH: none, no seizures or mental retardation SH: unknown tobacco/alcohol/drug use Meds: Alphagan and Azopt OS, pt has not been compliant with his medications ALL: NKDA

11
Dilated exam Lens: clear both eyes Ant vit: clear both eyes C/D: 0.2 OD, 0.65-0.7 OS D/M/V/P: margins sharp both eyes, pale disc OS, vitreous clear, macula flat, periphery flat 360 degrees of view both eyes

12
Follow-up Pt was discharged, declined to return for f/u F/u with local eye care provider No visual changes VA (sc) OD – 20/20 OS – 20/50-2 (unchanged) IOP OS 25-28 range
 OD – 20/20 OS – 20/50-2 (unchanged) IOP OS range")
13
Sturge-Weber Syndrome (encephalotrigeminal angiomatosis) Phakomatosis (“mother-spot”) Hamartomatous hemangiomas of face, eyelid, choroid, retina, meninges, brain Abnormal proliferation of blood vessels containing AV shunts Rarely bilateral Involves parietal and occipital lobes
 Phakomatosis ( mother-spot ) Hamartomatous hemangiomas of face, eyelid, choroid, retina, meninges, brain Abnormal proliferation of blood vessels containing AV shunts Rarely bilateral Involves parietal and occipital lobes")
15
Comi et al (2005): Found altered fibronectin expression in fibroblasts taken from port wine stains and brain compared to normal tissue from same subjects Fibronectin has effects on angiogenesis, vessel remodeling, and vessel innervation density No known genetic abnormality, possibly a somatic mutation Comi AM, Weisz CJ, Highet BH, Skolasky RL, Pardo CA, Hess EJ.Sturge-Weber syndrome: altered blood vessel fibronectin expression and morphology. J Child Neurol. 2005 Jul;20(7):572-7.
:")
16
Statistics No known incidence No known race or sex predilection No known prenatal or environmental risk factors Normal life expectancy Symptoms worsen with age Prognosis excellent to guarded

17
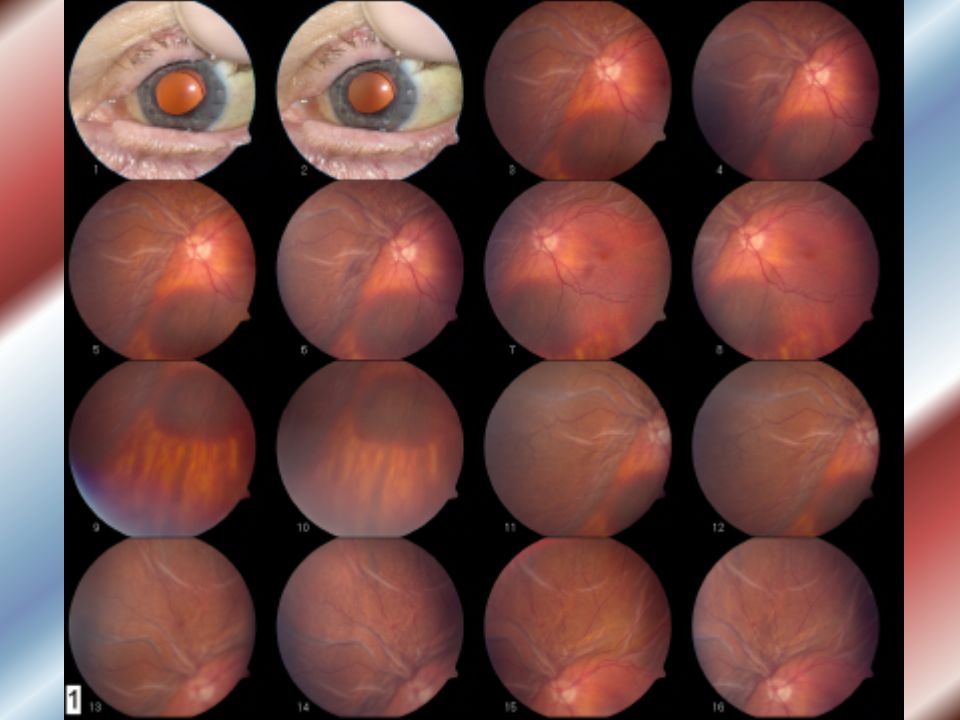
“Catsup Fundus” Doan A, Kwon YH: Sturge-Weber Syndrome: 4 y.o. child with a history of seizures and glaucoma. February 21, 2005 [cited –8/18/06-- ]; Available from: http://webeye.ophth.uiowa.edu/eyeforum/cases/case13.htm

18
Sturge-Weber Glaucoma Glaucoma in 30-70%, most common with involvement of upper lid Congenital (60%), childhood (30%) Later onset of sx usually between age 8-20 May present with photophobia, epiphora, blepharospasm, Haab’s striae, clouding of cornea, buphthalmos, amblyopia Retinal and choroidal detachments
, childhood (30%) Later onset of sx usually between age 8-20 May present with photophobia, epiphora, blepharospasm, Haab’s striae, clouding of cornea, buphthalmos, amblyopia Retinal and choroidal detachments")
19
Pathophysiology In 1973, Weiss proposed the following: Congenital cases caused by abnormal angles and increased episcleral venous pressure Childhood/adulthood cases caused by increased episcleral venous pressure only Elevated IOP directly related to decreased aqueous outflow and/or elevated EVP Weiss DI. Dual origin of glaucoma in encephalotrigeminal haemangiomatosis. Trans Ophthalmol Soc UK. 1973;93:477-493

20
Angle Abnormalities Scleral spur poorly developed Thickening of uveal and trabecular meshwork Displacement of iris root anteriorly Attachment of ciliary muscle directly to TM Neovascularization or fibrosis of the juxtacanalicular region

22
Aqueous outflow Aqueous drains from the anterior chamber through two routes: the conventional route (TM to SC) and uveoscleral outflow Hemangiomas upstream cause ↑ blood flow and pressure leading to elevated EVP
 and uveoscleral outflow Hemangiomas upstream cause ↑ blood flow and pressure leading to elevated EVP")
23
Episcleral venous pressure Normal EVP = 9 +/- 1.5 mmHg SC fills with blood when EVP>IOP (IOP is usually 5-6 mmHg higher) AV shunts Thyroid orbitopathy, artifact, body position or idiopathic Ocular hypotony
 AV shunts Thyroid orbitopathy, artifact, body position or idiopathic Ocular hypotony")
24
Treatment Resistant, may need repeat surgery Congenital cases: surgical; initial or repeated goniotomy/trabeculotomy, if ineffective, filtration surgery, shunt Later-onset: medical tx first, then trabeculectomy with MMC, shunt Diode cyclophotocoagulation last resort

25
Complications Sudden hypotony can cause large choroidal effusion or expulsive hemorrhage Prophylactic posterior sclerotomy, viscoelastic to AC or tight scleral flap sutures Increased risk for anesthesia complications including intracerebral bleed and DIC

27
Mandal et al. (1999): Retrospective study 9 patients (10 eyes) with SWS glaucoma Primary combined trabeculotomy- trabeculectomy without posterior sclerotomy performed by one surgeon No intra-op complications Post-op one pt developed shallow AC with choroidal detachment managed conservatively Mandal AM. Primary Combined Trabeculotomy-Trabeculectomy in Sturge-Weber Syndrome. Ophthalmology. 1999;1621-27.
: Retrospective study 9 patients (10 eyes) with SWS glaucoma Primary combined trabeculotomy- trabeculectomy without posterior sclerotomy performed by one surgeon No intra-op complications Post-op one pt developed shallow AC with choroidal detachment managed conservatively Mandal AM. Primary Combined Trabeculotomy-Trabeculectomy in Sturge-Weber Syndrome. Ophthalmology. 1999;")
28
Agarwal et al (1993): Retrospective study 16 pts (19 eyes) with SWS glaucoma Primary combined trabeculotomy-trabeculectomy performed in 18 eyes; repeat surgery in three eyes After average f/u of 42 mo, IOP was ≤ 22 mmHg in 11 eyes (61.1%) Intra-op complications: hyphema in four eyes (22.2%), vitreous loss in three eyes (16.7%) Post-op complications: choroidal detachment in three eyes (16.7%); vitreous hemorrhage in one (5.6%) Agarwal HC, Sandramouli S, Sihota R, and Sood NN. Sturge-Weber syndrome: management of glaucoma with combined trabeculotomy-trabeculectomy. Ophthalmic Surg. 1993:24:399–402

29
Pre-existing conditions/interventions can be confused for acute findings in the trauma setting Certain conditions place pts at risk for complications of surgery and anesthesia Take home points

30
References Agarwal HC, Sandramouli S, Sihota R, and Sood NN. Sturge-Weber syndrome: management of glaucoma with combined trabeculotomy-trabeculectomy. Ophthalmic Surg. 1993:24:399–402. Bellows AR, Chylack LT, Epstein DL, et al. Choroidal effusion during glaucoma surgery in patients with prominent episcleral vessels. Arch Ophthalmol. 1979;97:493-497 Board, RJ, Shields, MB: Combined trabeculotomy-trabeculectomy for the management of glaucoma in Sturge-Weber Syndrome. Ophthalmic Surg 12:813. 1981. Cibis GW, Tripathi RC, Tripathi BJ. Glaucoma in Sturge-Weber syndrome. Ophthalmology. 1984;91:1061-1071 Comi AM, Weisz CJ, Highet BH, Skolasky RL, Pardo CA, Hess EJ.Sturge-Weber syndrome: altered blood vessel fibronectin expression and morphology. J Child Neurol. 2005 Jul;20(7):572-7. Doan A, Kwon YH: Sturge-Weber Syndrome: 4 y.o. child with a history of seizures and glaucoma. February 21, 2005 [cited –8/18/06-- ]; Available from: http://webeye.ophth.uiowa.edu/eyeforum/cases/case13.htm http://webeye.ophth.uiowa.edu/eyeforum/cases/case13.htm Kanski J. Glaucoma. In: Clinical Diagnosis in Ophthalmology. First ed. Philadelphia: Elsevier; 2006:265-98. Mandal AM, and Gupta N. Patients with Sturge–Weber syndrome. Ophthalmology. 2004;111: 606. Olsen KE, Huang AS, Wright MM. The efficacy of goniotomy/trabeculotomy in early-onset glaucoma associated with the Sturge-Weber Syndrome. JAAPOS 1998;2:365-8. Phelps CD. Arterial anastomosis with Schlemm's canal: a rare cause of secondary open-angle glaucoma. Trans Am Ophthalmol Soc. 1985;83:304-15. Phelps CD. The pathogenesis of glaucoma in Sturge-Weber syndrome. Ophthalmology 1978;85:276-86 Weiss DI. Dual origin of glaucoma in encephalotrigeminal haemangiomatosis. Trans Ophthalmol Soc UK. 1973;93:477-493
: Doan A, Kwon YH: Sturge-Weber Syndrome: 4 y.o. child with a history of seizures and glaucoma. February 21, 2005 [cited –8/18/06-- ]; Available from: Kanski J. Glaucoma. In: Clinical Diagnosis in Ophthalmology. First ed. Philadelphia: Elsevier; 2006: Mandal AM, and Gupta N. Patients with Sturge–Weber syndrome. Ophthalmology. 2004;111: 606. Olsen KE, Huang AS, Wright MM. The efficacy of goniotomy/trabeculotomy in early-onset glaucoma associated with the Sturge-Weber Syndrome. JAAPOS 1998;2: Phelps CD. Arterial anastomosis with Schlemm s canal: a rare cause of secondary open-angle glaucoma. Trans Am Ophthalmol Soc. 1985;83: Phelps CD. The pathogenesis of glaucoma in Sturge-Weber syndrome. Ophthalmology 1978;85: Weiss DI. Dual origin of glaucoma in encephalotrigeminal haemangiomatosis. Trans Ophthalmol Soc UK. 1973;93:")
Similar presentations




 Waxman MD PhD>")

















