Download presentation
Presentation is loading. Please wait.

1
وقل رب زدنى علما سورة طه الآية (114)
")
2
By Hany A. AbdelWahab (M.Sc. Cardiology) Hypercoagulable states
 Hypercoagulable states")
3
physiological hemostasis The major components of the hemostatic system are : 1.The vessel wall. 2.Platelets (and other blood elements). 3.Plasma proteins (coagulation and fibrinolytic factors).
. 3.Plasma proteins (coagulation and fibrinolytic factors)..")
6
Subendothelial matrixEndothelial cell Vascular Phase

7
Platelet Activation Pathways Adhesion ADP Adrenaline Platelet GpIb Exposed Collagen Endothelium vWF Adhesion THROMBIN GpIIb/IIIa Aggregation COLLAGEN

9
Coagulation Factors I.Fibrinogen. II.Prothrombin. III.Thromboplastin. IV.Calcium. V.Proaccelerin (Labile factor). VII. Proconvertin (Stable factor). VIII.Antihemophilic globulin A. IX.Christmas factor. X.Stuart- Prower factor.
. VII. Proconvertin (Stable factor). VIII.Antihemophilic globulin A. IX.Christmas factor. X.Stuart- Prower factor..")
10
XI.Plasma thromboplastin antecedent. XII.Hageman factor. XIII.Fibrin Stabilizing factor.

12
Risk factors for Thrombosis In 1856, Rudolf Virchow postulated a triad of factors that leads to intravascular coagulation : 1.Local trauma to the vessel wall. 2.Hypercoagulability (Thrombophilia). 3.Stasis.
. 3.Stasis..")
14
A) Stasis: Immobility. Paralysis (e.g. CVA). Obesity. Postoperative & casting. Heart & Respiratory Failure.

15
B) Endothelial injury : Trauma & major syrgery. Central venous catheters.
 Endothelial injury : Trauma & major syrgery. Central venous catheters.")
16
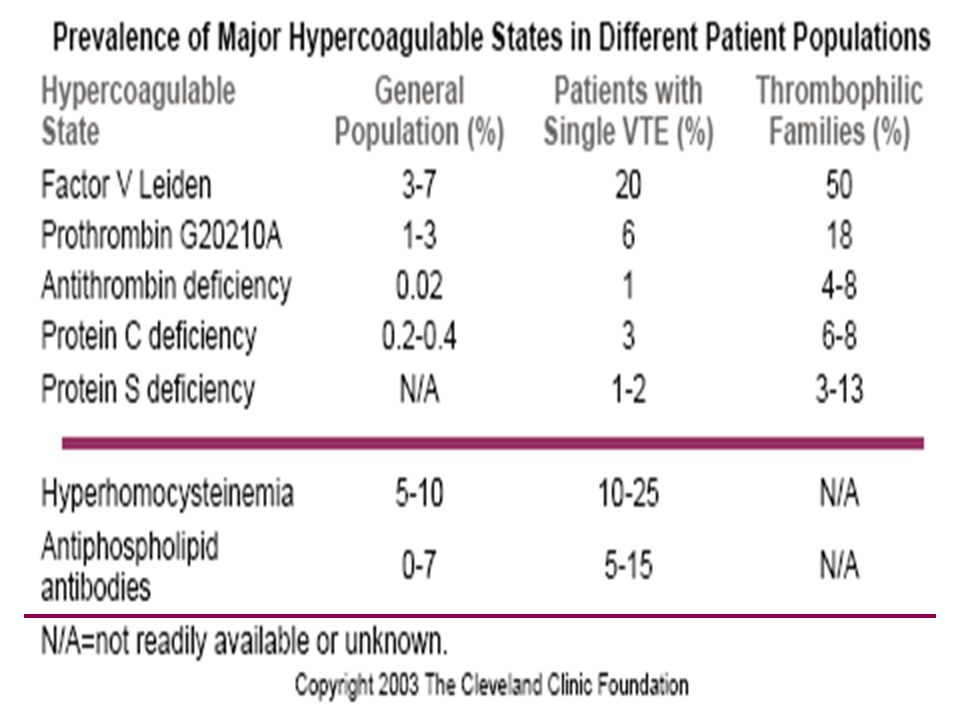
C) Hypercoagulable states (Thrombophilias) : ►Definition: Conditions that predispose to an increased risk for thrombosis either venous (most common), arterial or both. These conditions are being identified more frequently and may be classified as inherited or acquired.

17
Inherited Arterial and venousVenous Homocystinuria Factor V Leiden mutation HyperhomocystinemiaProthrombin G20210A DysfibrinogenemiaProtein C & Protein S deficiency Antithrombin deficiency Elevated Factor VIII activity

18
Acquired Arterial and venousVenous MalignancyAge Antiphospholipid antibodies syndrome Previous thrombosis Hormonal therapy (CCP) Immobilization Polycythemia veraMajor surgery Essential thrombocythemia Pregnancy & Puerperium HyperhomocystinemiaHospitalization Paroxysmal nocturnal hemoglobinuria. Activated Protein C

20
Factor V Leiden and prothrombin gene mutation Factor V Leiden mutation is the most common inherited thrombophilia. Normally, Activated protein C inactivates factors Va and VIIa and is one of the mechanisms that maintains a balance between clotting and bleeding.

21
This autosomal dominant disorder results from single mutation in the factor V gene (G1691A) which results in replacement of arginine amino acid 506 with glutamine. This renders the abnormal protein factor V Leiden resistant to inactivation by activated protein C. It is more prevalent in persons of European and Scandinavian ancestry.

22
Both homozygous and heterozygous states are at an increased risk for venous thrombosis with a 50- to 100- fold increase in the homozygous state and a 3- to 7-fold increase in the heterozygous state. Factor V Leiden doesn’t appear to be a risk factor for stroke or M.I. (supported by large cohort studies and meta- analysis evaluated 18 studies).
..")
23
The prothromin gene mutation G20210A is also inherited as an autosomal dominant mutation and leads to a higher plasma level of prothrombin probably by increase in mRNA and confers a 2.8-fold increased risk for venous thrombosis. The risk of recurrence and for arterial thrombosis is controversial.

24
Factor V Leiden and prothrombin gene mutation has been found to be associated with venous thrombosis during pregnancy and oral contraceptive use. Factor V Leiden mutation can be identified by evaluating for activated protein C resistance in the plasma or by gene analysis using polychromase chain reaction (PCR). The prothrombin gene mutation is identified by genetic analysis.
. The prothrombin gene mutation is identified by genetic analysis..")
25
There are no clear evidence-based guidelines for managing patients with these mutations. In general, acute thrombosis should be managed by the standard fashion. Patients with asymptomatic disease should receive prophylaxis in high risk situations.

26
Defects in the natural anticoagulants : Protein C (PC). Protein S (PS). Antithrombin (AT).
. Protein S (PS). Antithrombin (AT).")
28
Sites of action of the major antithrombotic pathways

29
Deficiency of any of the three natural anticoagulants is associated with an increased risk for venous thrombosis. They are inherited as AD defects. PS is bound to C4 binding protein in the plasma and acts as a cofactor in the inactivation of factors Va and VIIIa by activated PC.

30
Levels of PC & PS are lowered in conditions such as DIC, inflammatory states, acute thrombosis and liver diseases. Pregnancy and oral contraceptive pills can also decrease the levels of PS.

31
Levels of PC & PS are lowered by warfarin therapy So, initiation of warfarin therapy without concomitant anticoagulant therapy may lead to warfarin induced skin necrosis (manifested by painful skin necrosis primarily in the fatty areas), ttt includes stopping warfarin, administer vitamin K and plasma to replete levels, and using an alternative anticoagulant.
, ttt includes stopping warfarin, administer vitamin K and plasma to replete levels, and using an alternative anticoagulant.")
32
AT is produced by the liver and endothelial cells, and functions by inactivating thrombin, factor Xa and factor IXa. Homozygous states are extremely rare and incompatible with life. Levels are also low in DIC, sepsis, liver disease, nephrotic syndrome, the use of oral contraceptives, and during pregnancy.

33
In patients with AT deficiency, there may be resistance to heparin (i.e. failure to prolong the aPTT) as heparin exerts its anticoagulant effect through AT. AT concentrates are available and can be used to correct this deficiency.
 as heparin exerts its anticoagulant effect through AT. AT concentrates are available and can be used to correct this deficiency..")
34
Homocysteine It is derived from sulfur containing amino acid methionine and metabolized through pathways associated with folic acid, vitamin B6 and B12 as cofactors. Elevated plasma homocysteine levels > 15 μmol/L confer an independent risk factor for vascular disease (the relative risk for stroke and M.I. is double normal & for PVD is triple normal).
..")
36
Causes of Hyperhomocystenemia : 1.Deficiencies in the cofactors for its metabolism. 2.Defects in the genes for 5,10-methylene tetrahydrofolate reductase (MTHFR) (rare), cystathionine B-synthetase (0.5%), homocysteine methyl transferase and methionine synthetase (rare). 3.Secondary causes: age, male sex, menopause, liver and renal impairment, hypothyroidism, smoking and drugs (e.g. niacin, oral CCP, phenytoin, methotrexate and theophyllin).
 (rare), cystathionine B-synthetase (0.5%), homocysteine methyl transferase and methionine synthetase (rare). 3.Secondary causes: age, male sex, menopause, liver and renal impairment, hypothyroidism, smoking and drugs (e.g. niacin, oral CCP, phenytoin, methotrexate and theophyllin)..")
37
Possible mechanisms are that hyperhomocysteinemia may impair release of NO from endothelial cells, stimulates proliferation of atherogenic smooth muscle cells and contribute to thrombogenesis through activation of protein C kinase and expression of vascular adhesion molecule 1.

38
Patients with enzymatic deficiency especially cystathionine β-synthetase with marked elevations of homocysteine plasma level (> 100 μmol/L) suffer from premature atherosclerosis, arterial and venous thrombosis. homocysteinuria (homozygous Cβs deficiency) is very rare and manifested by mental retardation, skeletal anomalies and ectopia lenses.
 is very rare and manifested by mental retardation, skeletal anomalies and ectopia lenses..")
39
Therapy includes folate therapy (400 µg : 2 mg/day). Second line therapy 10 : 25 mg/day of pyridoxine (Vit. B6) with or without 400 µg of vit. B12/day (if there is vit. B12 deficiency). No data are available to establish the vascular benefits of reducing homocysteine values.
 with or without 400 µg of vit. B12/day (if there is vit. B12 deficiency). No data are available to establish the vascular benefits of reducing homocysteine values..")
40
Heparin induced thrombocytopenia (HIT) Two distinct types of HIT are known: 1- The more common form, which may occur in up to 15% of patients receiving therapeutic doses of heparin is a benign and self limiting side effect. This type is non immune mediated, rarely causes severe thrombocytopenia and usually doesn't require heparin discontinuation.

41
2- In contrast the immune type of HIT may cause serious arterial as well as venous thrombosis. Its pathogenesis involves the formation of antibodies (usually IgG) against the heparin- platelet factor 4 (PF 4) complex. The HIT Abs trigger procoagulant effect through platelets and endothelial cell activation, as well as thrombin generation leading to both micro- and macrovascular thrombosis.
 against the heparin- platelet factor 4 (PF 4) complex. The HIT Abs trigger procoagulant effect through platelets and endothelial cell activation, as well as thrombin generation leading to both micro- and macrovascular thrombosis..")
42
The incidence of HIT is about 3-5% in patients exposed to UFH, the incidence is much lower with the use of LMWH. In patients with de novo exposure to heparin a fall in the platelet count in those with HIT occurs between day 5 and 14.

43
The clinical diagnosis requires a fall in platelet count by 50% following heparin exposure or a fall by 30% in a setting of new thrombosis on heparin use. The clinical spectrum ranges from isolated HIT to HIT (T), where there is associated thrombosis that may be arterial (Stroke, MI, PAD) or venous in nature.
, where there is associated thrombosis that may be arterial (Stroke, MI, PAD) or venous in nature..")
44
Other manifestation include hypotension from adrenal hemorrhage secondary to adrenal infarction, skin necrosis or venous limb gangrene. Lab diagnosis includes functional assays of such as heparin induced platelet aggregation, serotonin release assay, immunoassays such as antibodies to heparin-PF 4 complexes.

45
The serotonin release assay has the highest sensitivity and specificity for the diagnosis of HIT. TTT includes stopping Heparin and starting an alternative anticoagulant unless C.I.

46
Direct thrombin inhibitors including Lepirudin and Argatorban are approved for the use in ttt of HIT (N.B. There are no available agents that reverse the effects of these drugs). As argatorban falsely INR, it should not be discontinued until the INR is > 4.
. As argatorban falsely INR, it should not be discontinued until the INR is > 4..")
47
Platelet transfusion should be avoided if possible as it may worsen the situation. Once the platelet count is > 100.000/CC warfarin may be started at low dose. It is reasonable to continue anticoagulation for at least a month in the absence of contraindications because the highest incidence of thrombosis occurs within the 1st month.

48
Antiphospholipid Antibodies Syndrome They are heterogeneous group of autoantibodies that in clinical practice can be divided into two large groups : (a) Anticardiolipin antibodies. (b) Lupus anticoagulants.
 Lupus anticoagulants..")
49
They are either not associated with an autoimmune disorder (1ry APS) or very often associated with autoimmune conditions (e.g. SLE) (2ry APS) and can cause recurrent pregnancy loss, as well as arterial or venous thrombosis. APA have also been reported in conjunction with idiopathic autoimmune hemolytic anemia, malaria, Q fever, infections by mycobacteria, Pneumocystis carinii, cytomegalovirus, and human immunodeficiency virus (HIV), and after exposure to drugs such as neuroleptics, quinidine, and procainamide.
 (2ry APS) and can cause recurrent pregnancy loss, as well as arterial or venous thrombosis. APA have also been reported in conjunction with idiopathic autoimmune hemolytic anemia, malaria, Q fever, infections by mycobacteria, Pneumocystis carinii, cytomegalovirus, and human immunodeficiency virus (HIV), and after exposure to drugs such as neuroleptics, quinidine, and procainamide..")
50
It has been reported that there is about fivefold increase in risk for thrombosis with lupus anticoagulant. Two mechanisms were proposed whereby antiphospholipid Abs promote thrombosis : 1.Interfering with the phospholipid dependant anticoagulant pathways. 2.Binding to cell surfaces and inducing cell activation.

51
Anticardiolipin antibodies are detected and quantified using an enzyme-linked immunosorbent assay and may be IgG, IgM, or IgA. IgG titers have been correlated with thrombosis. Lupus anticoagulants prolong phospholipids-dependent blood clotting times.

52
Once a thrombotic event occurs, long-term therapy with warfarin must be considered (Recurrence rate of thrombosis up to 70%). A higher target INR is used (approximately 3.0) as this may be superior to normal target INR of 2.0 to 3.0 in preventing recurrent events. Another strategy is to correlate the INR to a factor II and factor X level of 20% to 30 %.
 as this may be superior to normal target INR of 2.0 to 3.0 in preventing recurrent events. Another strategy is to correlate the INR to a factor II and factor X level of 20% to 30 %..")
53
Malignancy Many malignancies induce a hypercoagulable state and in patients with idiopathic thrombosis, a search for age- and gender- specific malignancies is necessary.

54
Hormonal Therapy Hormonal therapy carries increased risk for VTE, and the risk may be increased significantly in thrombophilic women. HRT and CCP increase the risk of thrombosis 2-4 folds. The pathogenesis of hormone induced thrombosis is not clear.

55
Estrogens have many different effects on the coagulation system including in procoagulant factors, protein S and antithrombin and acquired protein C resistance. It inceases the fibrinolytic activity but doesn’t counterbalance this procoagulant effect.

56
Other Conditions Elevated factor VIII levels, deficiency of plasminogen or tissue plasminogen activator (the fibrinolytic system), dysfibrinogenemia, and factor XIII polymorphism are emerging risk factors for hypercoagulability.
, dysfibrinogenemia, and factor XIII polymorphism are emerging risk factors for hypercoagulability.")
57
Stepwise Approach For Management of Thrombophilias

58
(A) When to suspect ?! Idiopathic (i.e., spontaneous) VTE. VTE at young age ( <45 years old). Recurrent VTE. VTE in unusual sites (e.g. U.L.) VTE in the setting of a strong family history of VTE. Recurrent pregnancy loss ( >3 consecutive first-trimester pregnancy losses without an inter-current term pregnancy).
. Recurrent VTE. VTE in unusual sites (e.g. U.L.) VTE in the setting of a strong family history of VTE. Recurrent pregnancy loss ( >3 consecutive first-trimester pregnancy losses without an inter-current term pregnancy)..")
59
(B) Diagnosis In fact, testing for an inherited hypercoagulable state is costly & likely to uncover an abnormality in more than 60% of patients presenting with idiopathic VTEs. Although the remaining 30% to 40% will have unremarkable test results, this does not imply a true absence of a hypercoagulable state. (Deitcher SR, 2000).
..")
60
In the absence of validated guidelines, testing for hypercoagulable states should be performed only in selected patients, and only if the results will significantly affect the management.

61
Confirmatory TestsScreening Tests Factor V Leiden PCR Activated protein C resistance. Antigenic assays for antithrombin, protein C, and/or protein S Prothrombin G20210A mutation testing by PCR. Antithrombin, protein C, and protein S activity (functional) levels. Confirmatory tests for lupus Anticoagulants ( Include at least one of the following: platelet neutralization procedure, hexagonal phase phospholipids, Textarin / Ecarin test, platelet vesicles, DVV Confirm.) Factor VIII activity level. Screening tests for lupus anticoagulants (sensititve aPTT, aPTT mixing studies, dilute Russell viper venom time) Anticardiolipin antibody testing by ELISA. Fasting total plasma homocysteine level. Recommended Laboratory Evaluation for Patients Suspected of Having an Underlying Hypercoagulable State
 levels. Confirmatory tests for lupus Anticoagulants ( Include at least one of the following: platelet neutralization procedure, hexagonal phase phospholipids, Textarin / Ecarin test, platelet vesicles, DVV Confirm.) Factor VIII activity level. Screening tests for lupus anticoagulants (sensititve aPTT, aPTT mixing studies, dilute Russell viper venom time) Anticardiolipin antibody testing by ELISA. Fasting total plasma homocysteine level. Recommended Laboratory Evaluation for Patients Suspected of Having an Underlying Hypercoagulable State.")
62
(C) Treatment There are no specific therapies to reverse most hypercoagulable states. Recombinant factor concentrates of antithrombin and APC do exist. Gene transfer to correct a particular genetic defect is theoretically feasible but likely cost prohibitive at this time. Attempts to eliminate APA by plasmapheresis or immunosuppressive therapy have not been very successful.

63
Initiation of oral anticoagulation for primary VTE prophylaxis in asymptomatic carriers of any hypercoagulable state has not been advised, mainly because the annual absolute risk of idiopathic VTE is either low or not high enough to be favorably balanced against the annual risk of oral anticoagulation- related major and fatal hemorrhage.

64
However, because most VTEs (50% to 70%) in patients with a predisposition to hypercoagulability occur following a situational risk factor, such as major or orthopedic surgery, aggressive VTE prophylaxis should be prescribed to asymptomatic carriers of hypercoagulable states during high- risk situations (Kearon C, 2000).
 in patients with a predisposition to hypercoagulability occur following a situational risk factor, such as major or orthopedic surgery, aggressive VTE prophylaxis should be prescribed to asymptomatic carriers of hypercoagulable states during high- risk situations (Kearon C, 2000).")
65
The presence of a hypercoagulable state should not affect acute VTE treatment (i.e., initial anticoagulation with intravenous unfractionated heparin or subcutaneous low- molecular-weight heparin followed by oral anticoagulation with warfarin) except for those with a lupus anticoagulant. Because these antibodies can prolong the aPTT, monitoring of unfractionated heparin therapy in this scenario should be performed by heparin assay (anti- factor Xa activity assay).
..")
66
If such assays are not immediately available, the use of weight-based, subcutaneous low-molecular-weight heparin should be considered instead of unfractionated heparin, because the former compounds do not require monitoring.

67
It must be emphasized that there are no current data from prospective, randomized controlled trials specifically designed to address the optimal duration of anticoagulation therapy in patients with specific hypercoagulable states.

68
Thus, any decisions regarding the ideal duration of therapy must take into account the estimates of VTE recurrence for a given disorder, the nature of the index VTE, and the risk of bleeding associated with prolonged oral anticoagulation.

69
However, it is also reasonable to consider long-term anticoagulation therapy for patients with conditions known to be associated with increased rates of VTE recurrence. These include individuals with documented persistent lupus anticoagulants, homozygous factor V Leiden, and may be patients with a deficiency of protein C or protein S, or with double heterozygosity for factor V Leiden and the prothrombin G20210A mutation.

70
Summary In summary knowledge about Hypercoagulable states is expanding. Identifying such states may alter type or intensity of therapy in some situations (e.g. HIT, antiphospholipid antibodies) and the duration of therapy in other situations. They should be suspected in patients who develop idiopathic VTE, VTE at a young age, VTE in unusual sites, recurrent VTE, and those with a strong family history of VTE and recurrent pregnancy loss.
 and the duration of therapy in other situations. They should be suspected in patients who develop idiopathic VTE, VTE at a young age, VTE in unusual sites, recurrent VTE, and those with a strong family history of VTE and recurrent pregnancy loss..")
Similar presentations









 is produced by a shift in the balance between.>")











i.>")




>")
