Download presentation
Presentation is loading. Please wait.

1
FUTURE RESEARCH IN SUBSTANCE MISUSE AN OVERVIEVW PERSPECTIVE Michael Farrell PHRN Manchester 20 th October 2006

2
Political and moral values of the social system Research Evidence SERVICE Provider AND USER VIEW A model for evidence-based clinical decisions (from Haynes et al, 1996)
")
3
Injecting

5
HIV prevalence among IDUs in the EU EMCDDA 2004 Notes: Colour indicates midpoints Local data shown in ()
")
6
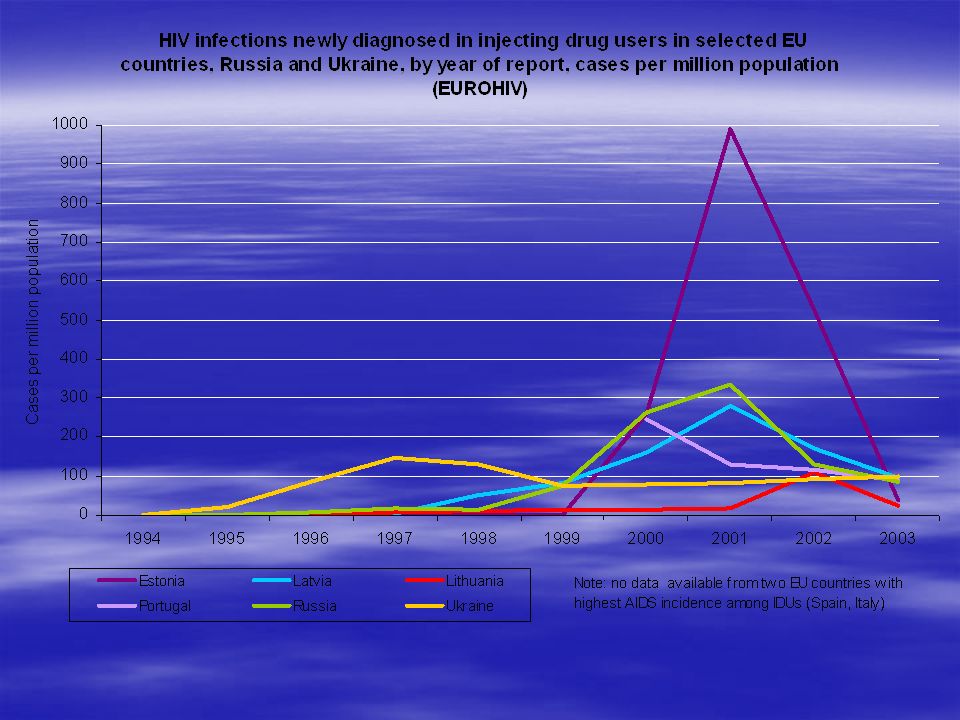
HIV in IDUs in Europe Marked difference between countries and within some countries –High prevalence countries (old MS) Italy, Spain, Portugal, followed by France –Some high prevalence estimates from new MS (Latvia, Estonia), and worries about others (Poland) –Low prevalence countries in both old and new MS including countries with high prevalence IDU –Cautious assessment is the long term trend appears to be stable or downwards Some small increases in recent data in some countries or in specific subpopulations Data quality problems so analysis must be made with caution
 Italy, Spain, Portugal, followed by France –Some high prevalence estimates from new MS (Latvia, Estonia), and worries about others (Poland) –Low prevalence countries in both old and new MS including countries with high prevalence IDU –Cautious assessment is the long term trend appears to be stable or downwards Some small increases in recent data in some countries or in specific subpopulations Data quality problems so analysis must be made with caution")
7
A note on HCV prevalence in IDUs Prevalence estimates higher and more convergent than for HIV Clear need to finding effective prevention strategies Routine disease surveillance sources of limited value Drug injecting principle route of transmission for HCV in Europe

8
50 100 150 200 250 300 Index % (1985=100%) INDEX 100,0104,5118,7136,9153,7181,0216,4223,5201,8212,2225,4252,4230,1235,6241,1255,4240,1205,8194,9 1985198619871988198919901991199219931994199519961997199819992000200120022003* Long term trend in acute drug-related deaths (1985-2003) EU 15, 1985 to 2003 index year 1985=100
 INDEX 100,0104,5118,7136,9153,7181,0216,4223,5201,8212,2225,4252,4230,1235,6241,1255,4240,1205,8194, * Long term trend in acute drug-related deaths ( ) EU 15, 1985 to 2003 index year 1985=100")
9
Introduction of MMT & NSP, 1967 to 2001 (EU, Norway and Bulgaria)
")
10
Estimated number of drug users in substitution treatment in 29 European countries (2003) per 100.000 population aged 15-64
 per population aged 15-64")
11
10-year trend in the number of substitution treatment clients in Europe (EU-15) 73,400 207,000 265,000 351,000 537,000 0 100,000 200,000 300,000 400,000 500,000 600,000 19931995199720002003
 73, , , , , , , , , , ,")
12
Proportion of substitution drugs used in medically assisted treatment in Europe, 2003 Methadone 79% Other 1% Buprenorphine 20%

13
Prevalence of HIV in Injecting Drug Users some country estimates European Union, Northern Europe low prevalence, Southern European countries higher prevalence but declining Central and Eastern European countries upward trend, especially Ukraine, Russia, USA and Canada generally stable low levels, outbreak Vancouver British Columbia related to cocaine injecting Australia less than 2% India Manipur Estimated at 50% plus China Yunnan Province 10% to 70% in three years Rapid increase in 31 provinces in China Myanmar 56% IDUs HIV positive in one study Vietnam 63% IDUs

14
HIV prevalence in injecting drug users Edinburgh Bangkok Myanmar Manipur & Yunnan Ho Chi Minh City Odessa Jakarta Lithuania

15
HIV infection rates in and out of substitution treatment (Metzger et al. 1993) Out % In %
 Out % In %")
16
Drug Overdose and Mortality Mean of 5+ non fatal overdoses in heroin using cohorts Mortality 1 to 2% In methadone treatment down to 0.2% Recent Hser 33 year longitudinal study reports over 50% mortality in cohort Suicide completion rates high and significant contributor to overall suicide

18
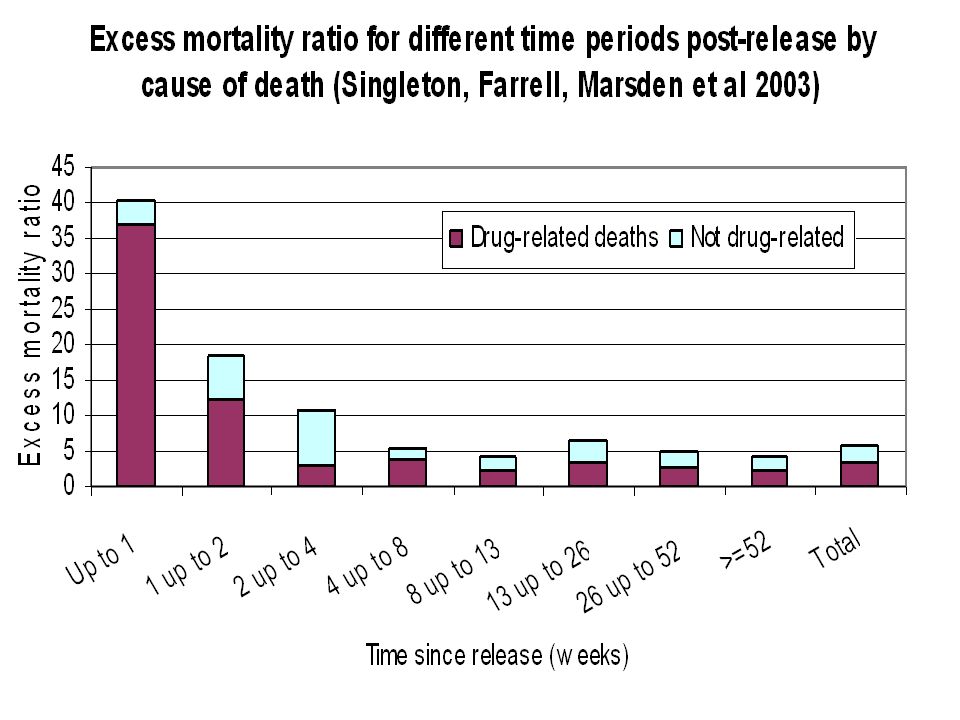
The odds of a drug-related death in the first week of release among women over 10 times greater than that observed at one year (OR 10.6; 95%CI 4.8-22.0) 70 times higher than age matched general population among men around 8 times greater than at one year (OR 8.3: 95%CI 5.0-13.3). 30 times higher than age matched general population (Singleton, Farrell et al 2003) IN SUMMARY A 8-10 FOLD INCREASED RISK OF MORTALITY IN THE EARLY RELEASE PERIOD
 IN SUMMARY A 8-10 FOLD INCREASED RISK OF MORTALITY IN THE EARLY RELEASE PERIOD.")
19
Substitution in prisons Estimated that over 30 million imprisoned annually Major risk for blood borne virus spread In most countries where measured between one third and half have drug dependence RCT of methadone in prison (Dolan et al) demonstrates role in reduction of blood borne virus, and general improvement, and post release reduction in mortality for those who continue Rapid expansion in Europe in substitution in prisons Huge challenge for Asia pacific region where insitutional incarceration standard response to opioid dependence Consistently 90% relapse to heroin use, no studies on mortality
 demonstrates role in reduction of blood borne virus, and general improvement, and post release reduction in mortality for those who continue Rapid expansion in Europe in substitution in prisons Huge challenge for Asia pacific region where insitutional incarceration standard response to opioid dependence Consistently 90% relapse to heroin use, no studies on mortality")
20
Drug Substitution Treatment Strong evidence for the benefits of oral methadone treatment RCTs +++ REASONABLE EFFECT SIZE REDUCES DRUG CRIME.70 REDUCES DRUG CRIME.70 REDUCES OPIATE CONSUMPTION.35 REDUCES INJECTING & RISK TAKING 0.22 Now good evidence for buprenorphine and LAAM RCTs ++ (LAAM CURRENTLY UNDER REVIEW) Use of injectable diamorphine and other drugs building evidence base for comparative effectiveness, more dicussion on comparative cost effectiveness.
 Use of injectable diamorphine and other drugs building evidence base for comparative effectiveness, more dicussion on comparative cost effectiveness.")
21
Gunne & Gronbladh (1981) RCT: Methadone versus no methadone 34 subjects using heroin by injection 17 experimental (methadone) 17 controls (no methadone) Controls not allowed to enter MMT for 2 years Followed up at 2 years and again at 4 years
 RCT: Methadone versus no methadone 34 subjects using heroin by injection 17 experimental (methadone) 17 controls (no methadone) Controls not allowed to enter MMT for 2 years Followed up at 2 years and again at 4 years")
22
Gunne & Gronbladh (1981): Baseline Experimental Group (methadone) Control group (no methadone) UUUUUUUU UUUUUUUU UUUUUUUU UUUUUUUU UU U – ongoing daily heroin Use
: Baseline Experimental Group (methadone) Control group (no methadone) UUUUUUUU UUUUUUUU UUUUUUUU UUUUUUUU UU U – ongoing daily heroin Use")
23
Gunne & Gronbladh (1981): 2 years Experimental group (methadone) Control group (no methadone) AAAAUUUA AAAAUUUU AAAAUUUU UUUUUUUD UD A – Abstinent U – on-going daily Use D – Deceased
: 2 years Experimental group (methadone) Control group (no methadone) AAAAUUUA AAAAUUUU AAAAUUUU UUUUUUUD UD A – Abstinent U – on-going daily Use D – Deceased")
24
Gunne & Gronbladh (1981): 4 years Experimental Group (methadone) Control group (methadone) (no methadone) AAAAUUUA AAAAAAUU AAAAAAUD UUUAAADD UD A – Abstinent U – on-going daily Use D – Deceased
: 4 years Experimental Group (methadone) Control group (methadone) (no methadone) AAAAUUUA AAAAAAUU AAAAAAUD UUUAAADD UD A – Abstinent U – on-going daily Use D – Deceased")
25
A 33 year follow-up of narcotic addicts (Hser et al., 2001) 22% 2% 6% 7% 4% 48% 12% N 581 439 354242 Age 24.5 (3.9) 36.8 (5.4) 47.6 (5.1)57.4 (4.0)
 22% 2% 6% 7% 4% 48% 12% N Age 24.5 (3.9) 36.8 (5.4) 47.6 (5.1)57.4 (4.0)")
26
A 33 year follow-up of narcotic addicts (Hser et al., 2001) 22% 2% 6% 7% 4% 48% 12% N 581 439 354242 Age 24.5 (3.9) 36.8 (5.4) 47.6 (5.1)57.4 (4.0)
 22% 2% 6% 7% 4% 48% 12% N Age 24.5 (3.9) 36.8 (5.4) 47.6 (5.1)57.4 (4.0)")
27
COMPOSITE SLIDE 3-Year Reincarceration Rates * * * *

28
Methadone maintenance for prisoners Location No. MMT Prison Population Rate % NSW1000815012.26 Austria34569154.9 Denmark29031509.2 France (Bup 879) 157 507140.3 Germany800787071.0 Spain180005065635.5 New York 400670650.5 Switzerland18049853.6 Source: NSW DCS Inmate Census, UK Home Office, World Prison Population List 4 th Ed, US Department of Justice
 Germany Spain New York Switzerland Source: NSW DCS Inmate Census, UK Home Office, World Prison Population List 4 th Ed, US Department of Justice.")
29
NSW prison methadone program 1986 as a pilot pre release program by Department of Corrective Services (DCS) Criteria 3-6 months prior to release Past or present history of opiate dependence History of returning to injecting and crime on previous releases 3 designated community clinics 1990 those entering custody on MMT were continued Since 1990 12% NSW MMT received in custody
 Criteria 3-6 months prior to release Past or present history of opiate dependence History of returning to injecting and crime on previous releases 3 designated community clinics 1990 those entering custody on MMT were continued Since % NSW MMT received in custody")
30
NDARC Methadone Study NSW prison methadone maintenance –Randomised control trail of 384 IDUs in 1997 and re-interviewed in 1998 –Heroin use was significantly less for those receiving methadone, as measured by hair analysis. Source: Dolan & Wodak

31
RCT Results MMTControl HCV incidence % 24.331.7 Heroin (hair) % 2742 Heroin (SR) %3378 No cases of HIV
 % 2742 Heroin (SR) %3378 No cases of HIV")
32
NDARC Methadone Study Follow up after release from gaol study of above 384 IDUs examining rate of: –Incarceration –Mortality –Hepatitis C

33
Mortality rates (Intent)
")
34
HCV incidence (Intent) MMT (N=52) CONTROL (N=56) Cases1423 Rate per 100 person years 18.336.5 95% CI 10 - 31 23 - 55 Previous rate at 5 months was 24 CI: 7-62 vs 31 CI: 9-81 Source: Dolan, K
 MMT (N=52) CONTROL (N=56) Cases1423 Rate per 100 person years % CI Previous rate at 5 months was 24 CI: 7-62 vs 31 CI: 9-81 Source: Dolan, K")
35
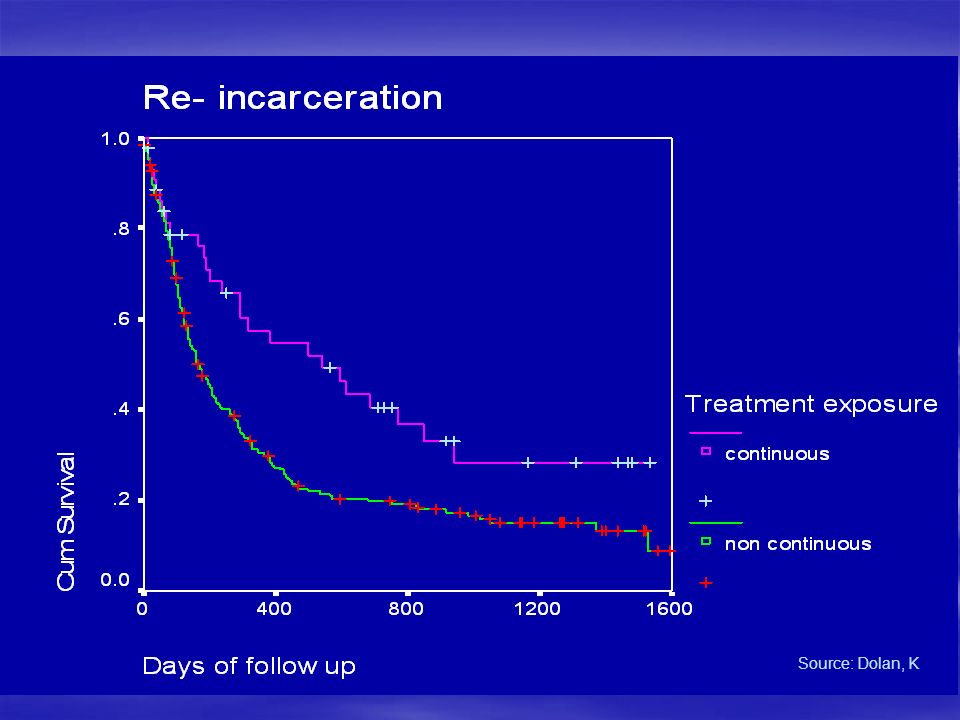
Re- incarceration up to May 2002 Continuousn=45 Non- Continuous n= 216 p Mean total weeks in prison (sd) 4167.007 Source: Dolan, K
 Source: Dolan, K")
37
Need for upscaling of treatment Urgent need in many regions for concerted effort to expand treatment Discussions and research required on the challenge of upscaling IDTS a major development within English Prisons Major expansion in substitution treatment and psychosocial treatment

38
NEED TO EVALUATE IDTS Implementation assessment Cost Effectiveness Environmental Impact Individual Outcome Impact on Recidivism Impact on Post Release Mortality

39
Research Framework Need pragmatic studies in prison context More longitudinal studies A 10 year mortality outcome study from the National Psychiatric Morbidity Survey Consider a longitudinal Study of Young Offenders and exploration of trajectory of drug histories within the criminal justice system Prisons ideal enviroments for exploration of issues of psychiatric comorbidity and substance use

40
Studies linked to community studies Linking treatment in prison up to the National Drug Treatment Monitoring System Currently Outcomes Monitoring Project Underway, Important to have Prison Treatment Linked into this. Infectious Diseases remain a big threat especially BBVs

41
Conclusions The huge challenge in all settings is to develop a comprehensive range of interventions that are humanitarian, effective and impactful for the all those who require interventions To ensure that ethical and humane treatment is delivered as effectively as possible in all settings

Similar presentations



 Department.>")



 Public Health England London,>")











