Download presentation
Presentation is loading. Please wait.

1
Unsafe Abbreviations: MultiCare Health System Will Barnes, Celeste Derheimer and Margo Forstrom Washington Patient Safety Coalition May 25, 2005 Teleconference

2
MultiCare Health System Acute Care & Surgical Centers –Allenmore Hospital –Mary Bridge Children’s Hospital & Health Center –Tacoma General Hospital –MultiCare Day Surgery Centers MultiCare Clinics Auburn Lakewood Covington Northshore East Hill Spanaway Gig Harbor University Place Kent Westgate Laboratories Northwest MultiCare HealthWorks MultiCare Home Services MultiCare Medical Associates MultiCare Urgent Care Centers Covington Lakewood Gig Harbor University Place Kent Westgate

3
National Patient Safety Goals The Joint Commission’s Board of Commissioners approved the first National Patient Safety Goals in July 2002. JCAHO established these goals to help accredited organizations address specific areas of concern in regards to patient safety. Goals and recommendations are announced in July and become effective on January 1 of the following year.

4
Unsafe Abbreviations (USA) As of January 1, 2004, all JCAHO accredited health care organizations are being surveyed for implementation of goal 2a: Improve the effectiveness of communication among caregivers. –This goal states specifically: Standardize the abbreviations, acronyms and symbols used throughout the organization, including a list of abbreviations, acronyms and symbols not to use. [Scored at Standard IM.3.10, EP #2].

5
Standard IM.3.10 Compliant Not/Compliant –The hospital has processes in place to effectively manage information, including the capturing, reporting, processing, storing, retrieving, disseminating, and displaying of clinical/service and non-clinical data and information.

6
Element of Performance: IM.3.10 - #2 Abbreviations, acronyms, and symbols are standardized throughout the hospital and there is a list of abbreviations, acronyms, and symbols not to use.

7
Institute for Safe Medication Practice (ISMP) “Absent scientific research to prove its effectiveness, the evidence for this error reduction strategy is nonetheless obvious. Similar to removing potassium chloride concentrate vials from patient care areas and providing timely pharmacy distribution of solutions, you don’t need scientific validation to prove that such action will prevent the drug from being given IV push. Similarly, we have enough obvious evidence that using “U” for “units” has led to countless tenfold overdoses of insulin, heparin, and penicillin G (including an infant death from hyperkalemia).”
. .")
8
The Challenge Developing and implementing a plan that would result in successfully eliminating the use of Unsafe Abbreviations throughout MultiCare Health System (MHS). One of the elements that added to the complexity is the fact that the goal relates to multiple disciplines; basically – anyone who documents in the patient record.

9
The Real Challenge Change daily practice that was previously acceptable and is an ingrained habit for our medical, nursing and pharmacy staff. –These abbreviations are taught to medical and allied health personnel in school as part of our training and are in use in everyday practice – making the challenge considerable.

10
Team Members J.D. Fitz, MD, Hospitalist Medical Director Karen Nilsen, MD, Acting Medical Director Mary Bridge Hospital Daniel Ginsberg, MD, Allenmore Hospital Executive Committee Richard Stubbs, MD, Vice President Medical Affairs Candace Smith, Allenmore Hospital Sue Hale, Mary Bridge Hospital Vicki Skorupski, Tacoma General Hospital Peg Isenhower, Home Health Margo Forstrom, Pharmacy Kathy Smoots, Pharmacy Diane Leaton, MMG Celeste Derheimer, Quality Management

11
Process The first step in the process was development of the unsafe abbreviations list. –To promote consistency in the community the list was developed in collaboration with other area hospitals and health systems. –It was felt that this regional list would facilitate implementation since the area physicians would get the same message regardless of where they practiced

12
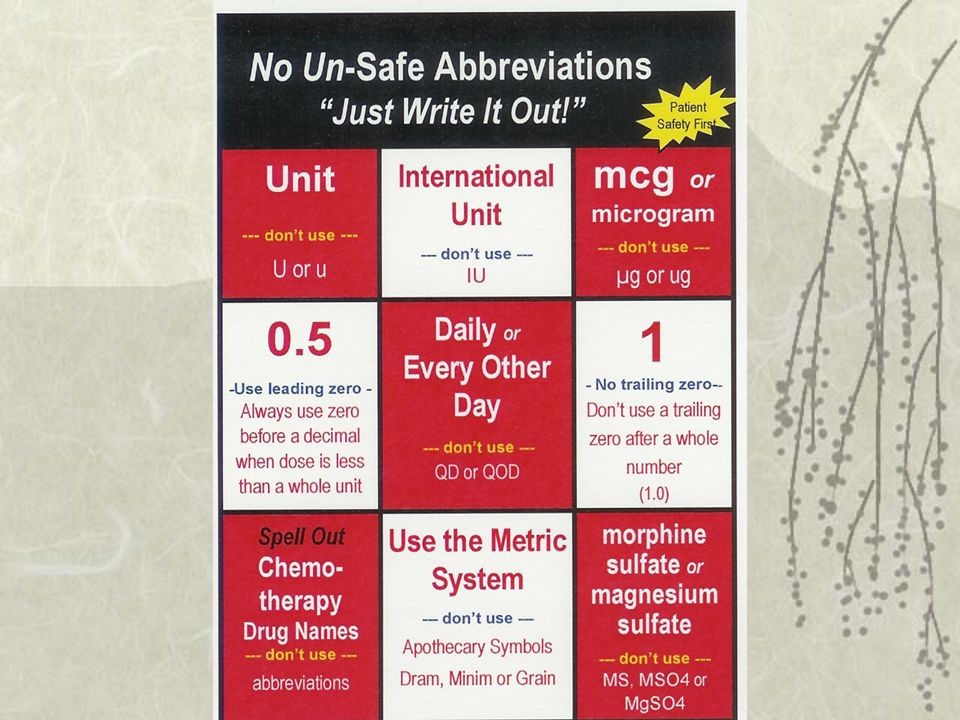
USE THIS DON’T USE THIS MISINTERPRETATION unitU or u (for unit)Read as a zero (0) or a four (4), causing a 10 fold overdose or greater (4U seen as “40 or 4u seen as 44”) International unitsIU (for international unit)Misread as IV (intravenous) instead of international units 1 mg (Do not use terminal zeros for doses expressed in whole numbers) Zero after decimal point (1.0) Misread as 10 mg if the decimal point is not seen 0.5 mg (Always use zero before a decimal when the dose is less than a whole unit) No zero before decimal dose (.5 mg) Misread as 5 mg Write “daily” and “every other day” QD or QOD (Latin abbreviation for once daily & every other day) Mistaken for each other. The period after the Q can be mistaken for an “I” and the “O” can be mistaken for and “I” (QID). Write “morphine sulfate” or “magnesium sulfate” MS, MSO4 or MgSO4Confused for one another. Can mean morphine sulfate or magnesium sulfate mcgugMistaken for “mg” when handwritten resulting in a thousand-fold overdose Use the Metric System Apothecary Symbols Dram, Minim, Grain Misunderstood or misread (symbol for dram misread for “3” and minim misread as “mL”) Spell out all chemotherapy names Chemotherapy drug name abbreviations Misread and wrong agent administered.
. Write morphine sulfate or magnesium sulfate MS, MSO4 or MgSO4Confused for one another. Can mean morphine sulfate or magnesium sulfate mcgugMistaken for mg when handwritten resulting in a thousand-fold overdose Use the Metric System Apothecary Symbols Dram, Minim, Grain Misunderstood or misread (symbol for dram misread for 3 and minim misread as mL ) Spell out all chemotherapy names Chemotherapy drug name abbreviations Misread and wrong agent administered..")
13
Initial Focus The initial JCAHO goal related to any handwritten documentation –The team identified that the area of focus would be on abbreviations used in patient orders – since implementation of orders that are not clear would most likely result error more often than unclear handwritten documentation in the progress or other notes.

14
Implementation Tools for implementation were developed –Discipline specific learning modules –Job aides such as the unsafe abbreviations “checker board” –Electronic billboards –Listing the unsafe abbreviations on the back of the order sheets so they would be readily visible to anyone responsible for writing orders.

16
Communication A communication plan was developed that identified the various forums, such as face-to-face meetings, written and electronic mechanisms, and audiences (e.g. physician, nursing, management and staff). In addition key themes that kept the message consistent regardless of the mode and/or audience were developed. A letter to all physicians that practice at a MultiCare hospital was sent out in December 2003
. In addition key themes that kept the message consistent regardless of the mode and/or audience were developed. A letter to all physicians that practice at a MultiCare hospital was sent out in December")
17
Communication Articles in Medical Staff News, MultiNews and other written forums –As compliance results became available, data was included in all communications Updates at various forums such as Medical Staff Meetings, Management Forum and the Profession Nurse Practice Council A second letter to all physicians in July and individual practitioner letters with copies of orders (patient de-identified) where they had used unsafe abbreviations in September
 where they had used unsafe abbreviations in September")
18
Communication Pharmacist and Nursing Education –Self learning modules –Department level training Included in various orientation packets –New employee –Medical Staff and Medical Students –Nursing and other allied health students

19
Implementation The final major implementation task was initiation of order clarification: Hand written orders that contained any of the MHS designated “Do Not Use” Abbreviations are considered incomplete orders; –The individual who wrote the order is contacted to clarify the intended meaning of the abbreviation prior to carrying out the order. –Confirm the intended meaning of the abbreviation or symbol and document in the medical record.

20
Implementation The team determined that the call verification process would begin September 1, 2004. –Decision primarily based on use of USA reduction to a manageable level –An update was presented at the second combined Medical Staff meeting in July; with input from that group, the decision was made to postpone the call verification process until October 1, 2004.

21
Measurement Baseline data for this project was obtained in December 2003. –Approximately one hundred orders per acute care facility (Allenmore, Mary Bridge and Tacoma General) and for the Neonatal Intensive Care Unit (NICU) were reviewed for use of unsafe abbreviations. –The indicator was defined as the number of unsafe abbreviations used per order. An “order” is specifically defined as a written entry into the chart, consisting of at least one line, by one practitioner at one time.
 and for the Neonatal Intensive Care Unit (NICU) were reviewed for use of unsafe abbreviations. –The indicator was defined as the number of unsafe abbreviations used per order. An order is specifically defined as a written entry into the chart, consisting of at least one line, by one practitioner at one time..")
22
Measurement The data was collected by chart abstraction at least quarterly. Results were provided by facility, by provider (Physician, Nursing and Pharmacy) and by specific unsafe abbreviation.
 and by specific unsafe abbreviation..")
23
Use of Unsafe Abbreviations Results - MHS

24
Use of Unsafe Abbreviations Results – Tacoma General/Allenmore

25
Use of Unsafe Abbreviations Results – Mary Bridge Children’s

26
Unsafe Abbreviation Use by Profession

27
% of total by Un-Safe Abbreviation

28
JCAHO Survey Three surveys in two weeks –Tacoma General/Allenmore –Mary Bridge Home Infusion –Mary Bridge Children's Hospital Different teams; different styles; VERY different experience –2 physicians, 3 nurses, 1 ambulatory surveyor and 1 engineer

29
National Summit on Medical Abbreviations As a result of recommendations in November 2004, the Executive Committee of the Joint Commission has approved the following changes addressing the scope of the requirements for NPSG 2b for 2005: –It now applies to ALL orders and ALL medication-related documentation that are handwritten, utilize free text entry or employ pre-printed forms. –The minimum expected level of compliance for handwritten documentation and free text entry is 90 percent.The minimum expected level of compliance for preprinted forms is 100 percent. –Clarification of an order prior to implementation is expected but does not eliminate that occurrence from being counted. Similarly, after-the-fact correction of the order by the clinician does not eliminate that occurrence from being counted.

30
JCAHO Scoring Changes Surveyors will count occurrences of Do Not Use Abbreviations. One occurrence equals one or more "slips" per clinician per record. Three occurrences equal a Requirement for Improvement. (Revised 1/21/05) There is no "partial compliance" for NPSGs. This requirement will not be surveyed in electronic documentation or computerized order entry in 2005. (New 12/20/04)
 There is no partial compliance for NPSGs. This requirement will not be surveyed in electronic documentation or computerized order entry in (New 12/20/04).")
31
Institute for Safe Medication Practice "Organizations are no longer considered compliant if pharmacists or nurses call a prescriber for clarification and document the intended meaning. –The goal is to remove responsibility for prescriber compliance from nurses and pharmacists, who've previously been placed in a position of enforcement, and redirect it to the medical and administrative staff. –As ISMP and others have pointed out, an unintended and serious consequence of having pharmacists and nurses shoulder this responsibility has been friction created by numerous phone calls and interruptions to clarify orders and educate prescribers."

32
JCAHO Survey Experience Tacoma General/Allenmore Hospitals (April ’05) –Although the hospital had a list of abbreviations, acronyms and symbols not to use, this list was not consistently followed throughout the institution. –Four uses of unacceptable abbreviations (qd, u and MSO4) by four different practitioners (2 physicians, a nurse and a pharmacist) were found on 3 different patient tracers.
 by four different practitioners (2 physicians, a nurse and a pharmacist) were found on 3 different patient tracers..")
33
JCAHO Survey Experience Mary Bridge Children’s Hospital and Mary Bridge Home Infusion Services (April ’05) –No unsafe abbreviations observed!!
 –No unsafe abbreviations observed!!")
34
Addressing the RFI Don't need to revise our policy or develop a new/different list!! –Provide additional training/education in areas were we know there is need –Focus on unit-level data collection and "immediate" results feedback (positive as well as improvement opportunities)
.")
35
Lessons Learned The people/areas impacted by the goal/standard have to own the work As Task Force members change jobs/leave – need a clear replacement process Need to provide direct feedback to change individual behavior – especially to those that are resistent

36
Keys to Success Collaboration with the Medical Staff and Leadership and involvement of multiple disciplines. Communicating information, including results, in multiple ways, multiple times. Clearly defining the indicator and data collection process and obtaining baseline data. Development of tools and processes for implementation that will be useful in other topic areas.

37
Keys to Success National Standard – not a MultiCare “mandate” Community Push –Regional P&T committees agreed on list –Providers hear the same message at all area hospitals Focus on Patient Safety, not compliance with JCAHO standard One of our Focus Objectives for the system – emphasized importance to organizational success

38
Next Steps Beyond hand written orders –Forms Committee inventory, search and destroy –Electronic Medical Record Beyond acute care –Home Health/Hospice –MultiCare Medical Associates

Similar presentations

 Carl Eagleton and Hannah O’Malley on behalf of the SMART Working Group.>")












 introduced.>")


 715-6418>")

